Page 4 of 12
OR7.1 | Metabolic Bone Disease Assessment — SDL Guide (Part 4)
Rickets: Deformity Management — Medical and Surgical
The management of rickets deformities is a two-phase strategy: first, correct the metabolic disease so that bone remineralises and has the capacity to remodel; second, address any residual mechanical deformity once metabolic control is confirmed. The medical phase is identical in principle to osteomalacia treatment: vitamin D replacement (ergocalciferol or cholecalciferol, high-dose loading then maintenance) combined with adequate calcium supplementation. In X-linked hypophosphataemic rickets, treatment requires oral phosphate supplementation and calcitriol (active vitamin D) rather than plain vitamin D, and more recently burosumab (anti-FGF23 monoclonal antibody) has been approved for this condition. Response to medical treatment is judged by normalisation of ALP, resolution of hypocalcaemia and hypophosphataemia, and radiological evidence of remineralisation — the previously frayed metaphyses sharpen, and the growth plate width returns toward normal. The critical principle is that no surgical correction should be attempted while rickets is metabolically active, because softened bone will not hold fixation reliably and deformity will recur unless the underlying biochemical defect is controlled first.
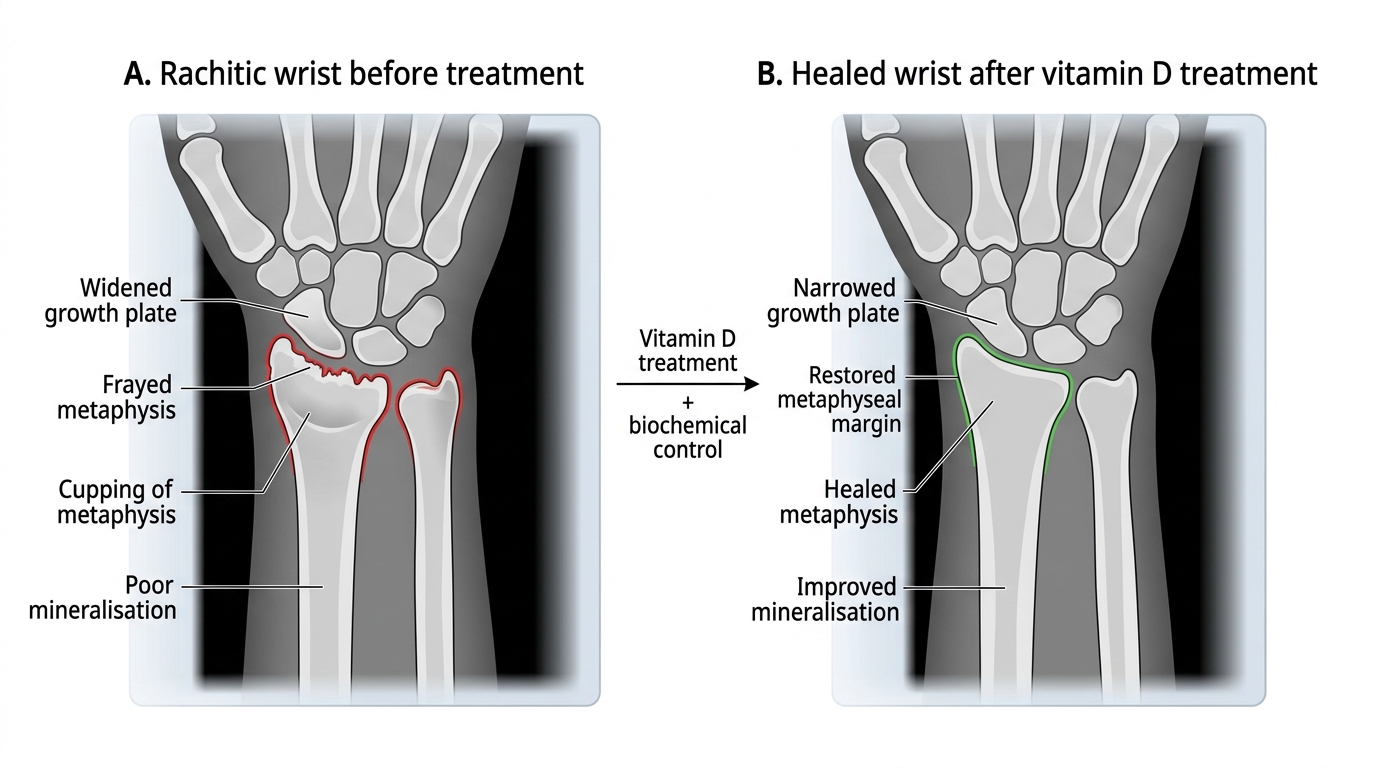
Rachitic Wrist Before and After Vitamin D Treatment
Once the disease is biochemically controlled (confirmed ALP normalised, vitamin D replete), residual angular deformities are managed according to the child's age and severity. Observation and watchful waiting is appropriate in children under 2 years, because the normal remodelling potential of young bone often corrects mild-to-moderate genu varum spontaneously once the metabolic drive is removed. For children aged 2-10 years with persistent deformity, corrective osteotomy is the definitive intervention: a valgus-producing osteotomy (for genu varum) or varus-producing osteotomy (for genu valgum) is performed, typically through the supracondylar femoral region or proximal tibia, and the corrected position held with plates, intramedullary rods, or a corrective cast depending on age and bone quality. Hemi-epiphysiodesis (physeal stapling or tension-band plating) is an elegant minimal-invasive technique in children with adequate remaining growth — tethering the convex side of the physis causes gradual guided growth correction over 12-18 months, avoiding formal osteotomy. Bracing alone is not curative but may be used as a temporising measure while awaiting metabolic stabilisation in very young children.
Paget's Disease: Management
Treatment is indicated for symptomatic Paget's disease, for patients with skull, spinal, periarticular, or weight-bearing bone involvement regardless of symptoms, and for patients at risk of complications. Asymptomatic monostotic disease with low ALP may simply be monitored with ALP levels annually. The mainstay of treatment is bisphosphonate therapy: zoledronic acid 5 mg IV as a single infusion is now the preferred agent, producing disease remission (normalisation of ALP) in approximately 85-95% of patients with a single treatment; this is superior to etidronate or pamidronate. Oral bisphosphonates (risedronate 30 mg daily for 2 months) are alternatives. The goal of treatment is to normalise ALP, which correlates with histological and radiological suppression of pagetic activity. Analgesics (NSAIDs, paracetamol) provide symptomatic relief. Specific complications require targeted management: pathological fractures are managed by orthopaedic fixation — intramedullary nailing is preferred for femoral fractures, although healing may be delayed in pagetic bone; nerve compression causing progressive neurological deficit may require surgical decompression; arthritis adjacent to pagetic bone (typically hip or knee) may need arthroplasty, but cement fixation in pagetic bone requires careful surgical technique due to altered bone architecture and vascularity; high-output cardiac failure requires medical cardiac management plus aggressive bisphosphonate treatment to reduce the arteriovenous shunting through hypervascular bone. Osteosarcoma arising in Paget's disease carries a very poor prognosis — 5-year survival is less than 5% — reinforcing the importance of early diagnosis.
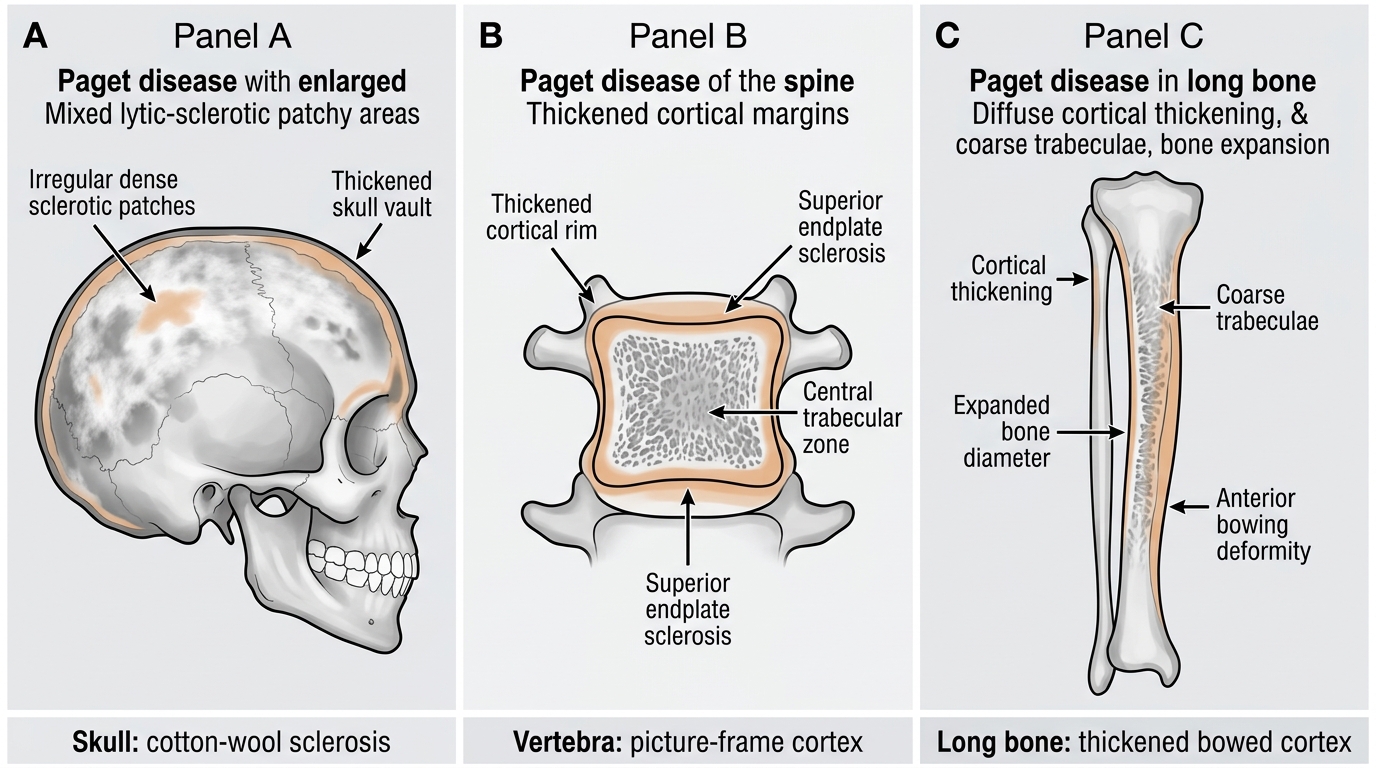
Radiological Features of Paget Disease of Bone
Self-Assessment: Integrating Clinical and Biochemical Reasoning
By this point in the module you should be able to approach any patient with bone pain, deformity, or fracture and immediately construct a biochemical hypothesis. The five-parameter panel — serum calcium, serum phosphate, serum ALP, serum PTH, and 25-hydroxyvitamin D — is your primary diagnostic tool, and the four diseases covered in this module each occupy a distinct region of the parameter space. Test your understanding against the following integrated scenarios. A 70-year-old woman with a wrist fracture after a minor fall, no bone pain, and normal calcium/phosphate/ALP: this is primary osteoporosis — the biochemical normalcy is the clue, and the next step is DEXA scanning and FRAX calculation. A 40-year-old woman with proximal myopathy, pelvic pain, and waddling gait with low calcium (7.8 mg/dL), low phosphate (2.0 mg/dL), ALP 420 U/L, and 25-OH vitamin D of 6 ng/mL: this is osteomalacia, and the X-ray of her pelvis should be scrutinised for Looser's zones at the pubic rami and femoral necks. A 2-year-old boy with bow legs, rachitic rosary, and ALP of 750 U/L: active nutritional rickets — start vitamin D and calcium, hold surgery. A 58-year-old man with deep skull, hip, and shin pain, hat size increase, hearing loss, and ALP of 1200 U/L with normal calcium, phosphate, PTH, and vitamin D: Paget's disease — arrange a bone scan to map all affected sites and initiate zoledronic acid.
The therapeutic implications follow directly from the diagnosis: osteoporosis is treated anti-resortively; osteomalacia/rickets is treated by replacing the missing mineral/vitamin; Paget's disease is treated with bisphosphonates targeted at the disorganised osteoclastic activity. Getting the diagnosis right from the biochemical panel — rather than treating empirically — is the clinical skill this module has trained you to deploy.
CLINICAL PEARL
The ALP as the metabolic compass: If a patient presents with bone pain and the ALP is five to twenty times normal with normal serum calcium, phosphate, and PTH, Paget's disease is almost certainly the diagnosis. If the ALP is two to five times normal with low calcium and low phosphate, think osteomalacia. If the ALP is very markedly elevated in a child with bone pain and deformity, think active rickets. Primary osteoporosis does not produce a biochemical signal — normal bone biochemistry in an elderly person with a fragility fracture is osteoporosis by default. A useful clinical trick: ask the patient if their hat has stopped fitting. Skull enlargement in middle-aged to elderly patients is almost pathognomonic of Paget's disease. And always remember the rickets management rule: never correct bow legs or knock knees surgically until the metabolic disease is fully controlled — operating on active rickets is futile and potentially harmful.