Page 2 of 15
OR8.1 | Post-polio Residual Paralysis — SDL Guide (Part 2)
Management Principles: Physiotherapy, Orthoses, and Conservative Measures
Management of PPRP follows a strict, clinically-grounded hierarchy: conservative and rehabilitative measures form the foundation, corrective procedures address established deformity, and functional (reconstructive) procedures restore muscle power balance. The rationale for this rigid sequence is that performing a functional procedure — such as a tendon transfer — onto an uncorrected rigid deformity or an unstable joint guarantees a poor or failed result. The transferred tendon will be placed under abnormal tension, the joint will lack the full passive range of motion the tendon needs to act through, and the patient's functional outcome will be no better than without surgery. This principle of hierarchy is one of the most clinically tested and important tenets in orthopaedic management of paralytic conditions.
Physiotherapy and rehabilitation are the foundation of all stages. Active assisted exercises maintain range of motion, strengthen innervated muscles, prevent disuse atrophy, and improve gait pattern. Hydrotherapy (buoyancy-assisted exercise in warm water) is particularly valuable for MRC grade 2–3 muscles because buoyancy offloads body weight and allows exercise that would be impossible on dry land. Occupational therapy addresses functional independence in activities of daily living.
Orthotic devices (callipers and orthoses) substitute for paralysed muscle function, prevent deformity progression, and enable safe ambulation:
- Ankle-foot orthosis (AFO) — polypropylene AFO: standard for isolated foot drop (absent dorsiflexors) or equinus; maintains the ankle at 90° during swing phase
- Knee-ankle-foot orthosis (KAFO): for combined quadriceps + ankle weakness; provides knee stability in stance
- Hip-knee-ankle-foot orthosis (HKAFO): for proximal paralysis with hip extensor and abductor involvement; bulky and rarely tolerated long-term
- Floor-reaction AFO / posterior-leaf spring AFO: exploits ground-reaction force to extend the knee in stance — useful for mild-to-moderate quadriceps weakness without fixed deformity
- Thomas calliper: long-leg iron with ischial ring; weight transmitted through the ischium rather than the joint; useful in resource-limited district hospitals for flail hip
Critical principle: An orthosis must fit a plantigrade foot. Any equinus contracture must be corrected — by serial plaster, tenotomy, or tendon lengthening — BEFORE orthosis prescription; otherwise the device simply immobilises the foot in equinus without benefit.
Serial plaster splinting: For dynamic equinus contractures in children under 10, progressive manipulation and cast wedging can achieve full correction non-surgically over 6–8 weeks. After correction, a night splint maintains position until skeletal maturity.
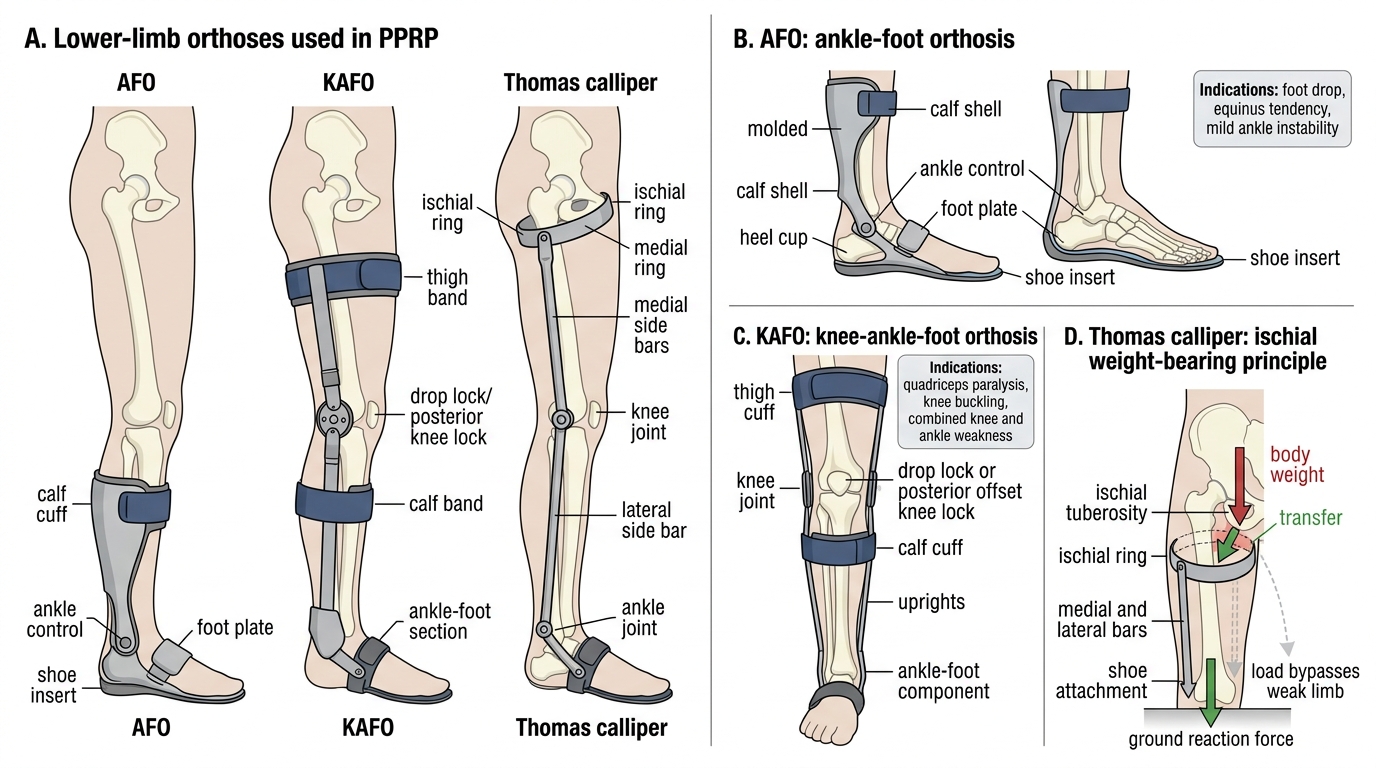
Lower-Limb Orthoses in PPRP
Surgical Management: Tendon Transfers and Arthrodesis
Surgical intervention in PPRP aims to correct established deformity and restore functional muscle balance across paralysed joints. The two broad categories of procedure are soft-tissue procedures — tenotomy, tendon lengthening, fasciotomy, and tendon transfer — and bony procedures including corrective osteotomy, arthrodesis, and epiphysiodesis for leg-length equalisation. The overarching cardinal rule of PPRP surgery is to perform all corrective procedures before any functional procedures: never attempt a tendon transfer across a joint that still harbours a fixed deformity or significant ligamentous instability. A transferred tendon inserted onto an uncorrected foot functions only in the plane of deformity, not in the intended corrective direction, and the patient gains nothing — or is left worse. This sequencing rule must be internalised before learning any individual procedure.
Tendon transfer is the cornerstone of functional reconstruction in PPRP. The concept is straightforward in principle: a muscle with redundant or expendable action in one plane is detached from its insertion and re-routed to substitute for the function of a paralysed muscle in another plane. The technical and biological demands, however, are exacting — hence the four prerequisites that must ALL be met before any transfer is planned.
Prerequisites for tendon transfer — all four must be satisfied before any transfer is attempted:
- Donor muscle grade ≥ 4 (MRC): A transferred muscle loses approximately one MRC grade due to altered mechanical advantage and the physiological demands of reinnervation at the new attachment site. A grade 4 muscle therefore transfers as a functional grade 3; a grade 3 muscle becomes non-functional (grade 2) and the patient is worse off than before surgery.
- Supple joint: The joint across which the transfer acts must have a full passive range of motion. A fixed contracture must be corrected first (by tenotomy, Achilles lengthening, or corrective osteotomy); otherwise the transferred muscle has no range to work in.
- Neurological stability: Recovery must be complete — at least 2 years post-acute illness. Transferring a muscle before the convalescent phase is complete risks sacrificing a muscle that would have recovered spontaneously.
- Correct direction of pull: The transferred tendon must run in a straight line from its new origin to its new insertion, in the precise direction of desired action. Angulation or routing over a pulley significantly reduces mechanical efficiency.
Common tendon transfers in PPRP:
| Deformity | Procedure | Donor → Recipient |
|---|---|---|
| Equinus (paralysed dorsiflexors) | Tibialis posterior transfer | Tibialis posterior → dorsum of foot through interosseous membrane |
| Paralytic calcaneus (paralysed plantarflexors) | Peroneus longus transfer | Peroneus longus → calcaneum / Achilles tendon |
| Hip abductor weakness (Trendelenburg) | Mustard procedure | Iliopsoas → greater trochanter |
| Flail knee (paralysed quadriceps) | Hamstring transfer | Biceps femoris / semitendinosus → patella / patellar ligament |
| Valgus foot | Split tibialis anterior transfer | Half of tibialis anterior → lateral cuneiform |
Arthrodesis (joint fusion) is reserved for flail joints where no reconstructable muscle function exists, where orthosis fitting is impractical or has failed, or to supplement a tendon transfer when ligamentous laxity is excessive. Key arthrodeses:
- Triple arthrodesis (fusion of talocalcaneal + talonavicular + calcaneocuboid joints): corrects rigid hindfoot deformity (equinovarus or equinovalgus) and produces a stable, plantigrade foot. Must wait for skeletal maturity (typically 12–14 years) to avoid growth disturbance.
- Knee arthrodesis: for a flail flaccid knee unresponsive to orthosis; trades mobility for stability; enables gait without a KAFO but with a permanently stiff knee.
- Pantalar arthrodesis: fuses all ankle and hindfoot joints simultaneously; for the most severely flail foot where no active muscle function is reconstructable.
Timing principle: Correct rigid deformities first (soft-tissue releases, osteotomy), then perform functional procedures (tendon transfer) once joints are supple and correction is maintained. Never combine a tendon transfer with a corrective osteotomy at the same joint in the same sitting.
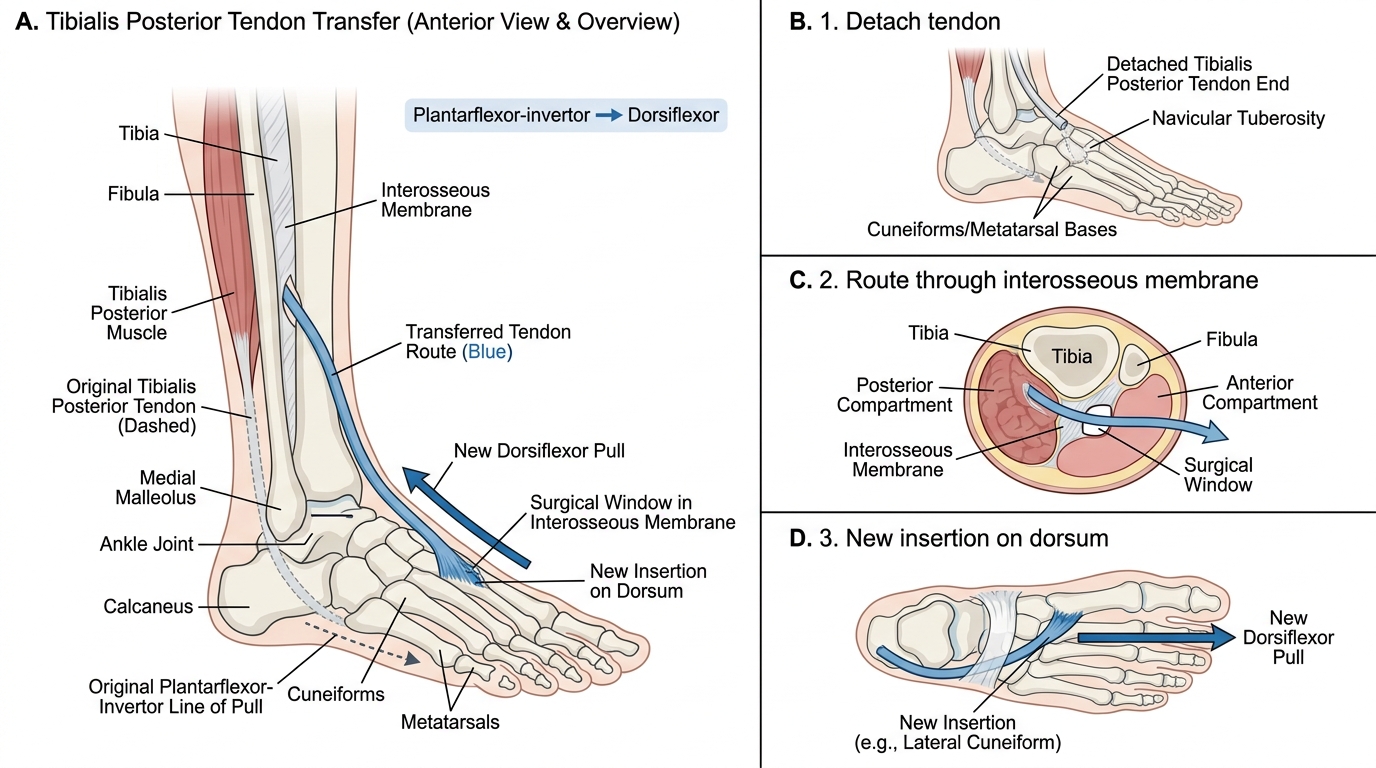
Tibialis Posterior Transfer for Equinus Foot
Specific Deformity Patterns and Their Management
Each specific deformity pattern in PPRP is directly predictable from the muscle chart — knowing which muscles are paralysed tells you which deformity will develop. The following pairs illustrate the most commonly encountered clinical problems at a district hospital orthopaedic clinic.
Equinus (most common PPRP foot deformity): Paralysis of tibialis anterior and other dorsiflexors with intact gastrosoleus. Dynamic equinus in young children: serial plaster correction over 6–8 weeks. Fixed equinus requiring surgery: percutaneous Achilles tendon lengthening (Hoke triple hemisection or Vulpius recession) followed by tibialis posterior transfer (through interosseous membrane to dorsum of foot) when tibialis posterior is grade ≥4.
Equinovarus: Combined equinus and inversion from paresis of peronei and dorsiflexors with intact tibialis posterior and gastrosoleus. Correction: Achilles lengthening + tibialis posterior tenotomy or split transfer; triple arthrodesis for rigid fixed cases.
Paralytic calcaneus: Isolated paralysis of gastrosoleus with functioning dorsiflexors. The patient bears weight on the heel with absent push-off — a characteristic 'calcaneal' gait with rapid heel-strike and no propulsion phase. Correction: peroneus longus transfer to reinforce the Achilles tendon; Lambrinudi arthrodesis (a variant of triple arthrodesis) produces a plantigrade foot without relying on active plantarflexion power.
Genu recurvatum: Quadriceps weakness leads to compensatory hyperextension of the knee in stance (locking the knee mechanically against the ground-reaction force). Over years, posterior capsule and cruciate ligaments stretch, producing a structural recurvatum deformity. Prevention: floor-reaction AFO early; correction of established deformity: knee extension stop orthosis; severe cases: supracondylar extension osteotomy.
Paralytic hip dislocation: Combined paralysis of hip abductors and extensors with intact adductors and flexors produces progressive adduction-flexion deformity and eventual lateral dislocation. Management: adductor tenotomy + flexor release (soft tissue); shelf acetabuloplasty or Chiari osteotomy for established dislocation.
Paralytic scoliosis: Asymmetric paralysis of trunk muscles; unlike idiopathic scoliosis, may be severe and rapidly progressive. Management: Milwaukee brace/TLSO for curves <40° in growing children; posterior spinal instrumentation and fusion for curves >50° or rapidly progressive curves.
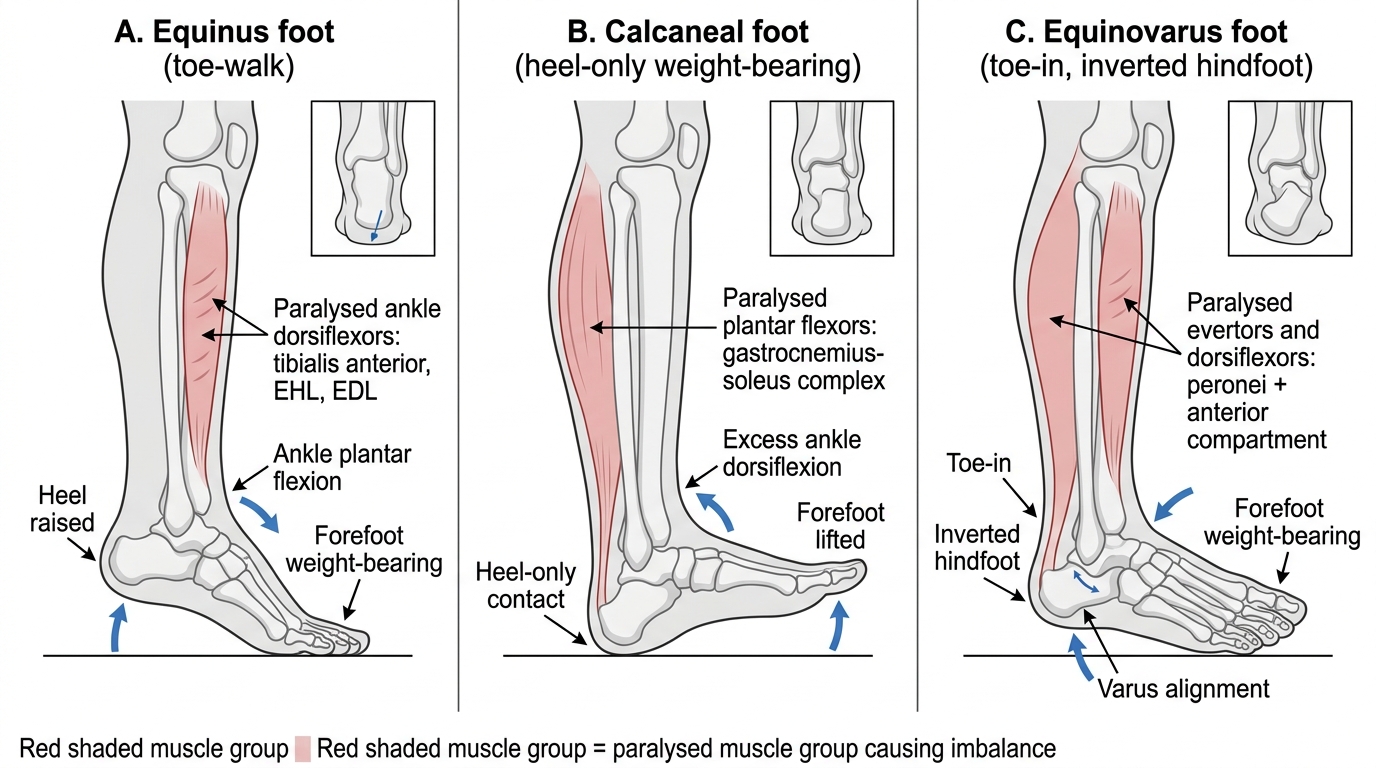
Common PPRP Foot Deformities and Paralysed Muscle Groups
SELF-CHECK
You plan a tibialis posterior tendon transfer for equinus foot in a 12-year-old with PPRP. On muscle charting, tibialis posterior is MRC grade 3. The ankle has a 15-degree fixed equinus contracture. Which of the following best describes the situation?
A. Both prerequisites are met; proceed with tibialis posterior transfer immediately
B. Donor muscle grade is insufficient (need ≥4); fixed contracture must also be corrected first — address both before transfer
C. Only the fixed contracture needs correction; grade 3 donor is acceptable for transfer
D. Neurological stability is the missing prerequisite; wait 6 more months for further recovery
Reveal Answer
Answer: B. Donor muscle grade is insufficient (need ≥4); fixed contracture must also be corrected first — address both before transfer
Two prerequisites are unmet. First, the donor muscle is MRC grade 3 — below the required minimum of grade 4. After transfer, the muscle loses approximately one MRC grade; a grade 3 donor would function as a non-functional grade 2, producing no active dorsiflexion. Second, a fixed equinus contracture of 15 degrees means the joint is not supple — the contracture must be corrected (by Achilles tendon lengthening or serial plaster) before transfer, or the transferred tendon has no useful arc of motion to work in. Neurological stability is not the issue here: the child is 12 years old, well beyond 2 years post-acute illness.