Page 30 of 44
EN2.10 | ENT Emergency Simulation Workflow — SDL Guide
Learning Objectives
- Apply the ABCDE resuscitation framework to ENT emergency presentations
- Describe the indications for and technique of tracheostomy and cricothyroidotomy as emergency airway procedures
- Perform anterior nasal packing for epistaxis with correct technique
- Describe the correct approach for foreign body removal from the ear, nose, throat, upper respiratory tract, and food passages
- Triage ENT emergencies by urgency and initiate appropriate initial management in a simulated setting
INSTRUCTIONS
ENT emergencies include life-threatening airway obstruction, severe epistaxis, and aspirated or impacted foreign bodies — all of which require immediate, protocol-driven action. This module covers the simulation-based workflow for each emergency, emphasising the decision points, technique, and the specific complications that arise from incorrect management.
References
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery, 8th ed. Emergency chapters (textbook)
- Hazarika P. Textbook of Ear, Nose and Throat & Head Neck Surgery, 3rd ed. Emergency section (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed. Airway and epistaxis chapters (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 11 PM in the casualty department. Three emergencies arrive simultaneously: (1) a 55-year-old male with hypertension who has been bleeding from both nostrils for 45 minutes — the pillow is soaked in blood; (2) a 2-year-old child brought in by panicking parents — she had a 20-paisa coin in her hand and suddenly started choking; now she is cyanotic and stridor is audible; (3) a 35-year-old male post-road traffic accident — his face is crushed and he is making gurgling, straining efforts to breathe. Which emergency do you attend to first, and what do you do in the first 60 seconds for each?
WHY THIS MATTERS
EN2.10 is one of only two NMC ENT competencies requiring Action (A) level attainment alongside Knowledge and Skills — reflecting the NMC's recognition that ENT emergencies occur outside the ENT department and must be managed by any doctor in any setting. A child with a coin in the larynx will die without airway intervention within minutes; a hypertensive elderly patient with a posterior nasal bleed can exsanguinate if the bleeding is managed with the technique for an anterior bleed; a patient with facial trauma whose airway is compromised cannot wait for an ENT specialist. This SDL provides the protocol-driven simulation framework for each emergency — not to make you a specialist, but to give you the initial management skills that save the patient's life in the first critical minutes.
RECALL
Recall the ABCDE resuscitation framework: Airway (open, clear, and maintain), Breathing (assess respiratory effort, SpO₂, rate), Circulation (heart rate, blood pressure, bleeding), Disability (neurological status — GCS, pupils), Exposure (full exposure to identify injuries). In ENT emergencies, the 'A' step dominates because most ENT emergencies either directly compromise the airway (foreign body, laryngeal oedema, laryngeal trauma) or lead to airway compromise if not controlled (uncontrolled posterior epistaxis → blood swallowed or aspirated; retropharyngeal abscess → impending airway obstruction). Recall also: anterior epistaxis arises from Little's area (Kiesselbach's plexus) on the anterior nasal septum (5 vessels: anterior ethmoidal, posterior ethmoidal, greater palatine, sphenopalatine, superior labial); posterior epistaxis arises from the sphenopalatine or Woodruff's plexus in the posterior nasal cavity. The cricothyroid membrane lies between the thyroid cartilage (superior) and the cricoid cartilage (inferior), approximately 2–3 cm below the thyroid notch, in the midline — accessible to needle or surgical cricothyroidotomy.
Clinical Indication: ENT Emergencies Requiring Immediate Action
ENT emergencies are defined by the clinical principle that delayed or incorrect management leads to death or permanent disability within a short timeframe. This is not a principle unique to ENT — but the anatomical concentration of airway, major vessels, and critical nerves in the head and neck means that ENT emergencies can become fatal within minutes of presentation. The head and neck region contains the only passage for air into the lungs (the laryngotracheal airway), major vessels capable of producing exsanguinating haemorrhage (the internal and external carotid arteries, the sphenopalatine vessels), and critical nerve structures whose injury causes permanent functional loss (facial nerve, recurrent laryngeal nerve, vestibulocochlear nerve). This anatomical density is what gives ENT emergencies their characteristic urgency — and why the ABCDE framework (Airway first) must be applied to every ENT emergency presentation, even when the presenting complaint appears straightforward. Recognising the urgency tier of each presentation is the first management decision, and it must be made within the first minute of assessment.
Immediately life-threatening ENT emergencies (act within minutes):
- Airway obstruction — stridor (inspiratory = supraglottic/glottic obstruction; expiratory = lower airway; biphasic = tracheal/subglottic). Any increasing respiratory distress with stridor is an impending complete airway obstruction and requires airway intervention within minutes. Causes: laryngeal foreign body, epiglottitis (supraglottic swelling), laryngeal trauma, anaphylaxis (laryngeal oedema), retropharyngeal abscess.
- Major haemorrhage from epistaxis — a patient losing blood at a rate that cannot be controlled by simple pressure, or showing signs of haemodynamic compromise (tachycardia, hypotension), has a life-threatening posterior nasal bleed until proven otherwise.
- Button battery in ear or nose — tissue necrosis from the electrical and chemical action of a lithium button battery begins within 1–2 hours of contact with mucosa; nasal septal perforation can occur within 4 hours. Requires immediate removal under GA if the battery cannot be retrieved quickly and safely in the ED.
Urgent but not immediately life-threatening (act within 1–4 hours):
- Foreign body in the ear (no airway compromise, no button battery)
- Foreign body in the nose in a cooperative child without respiratory distress
- Acute suppurative otitis media with impending perforation
Important but can wait for specialist (hours to day):
- Aural foreign body without complications in an adult
- Rhinolith (long-standing nasal foreign body)
The ABCDE framework is applied at every ENT emergency encounter: assess Airway first, then Breathing, then Circulation. A patient with a nose bleed who is cyanotic from a simultaneously obstructed airway needs the airway secured BEFORE nasal packing.
Airway Emergency Principles and Equipment
Airway management is the highest-priority skill in ENT emergency practice. The decision between different airway interventions — ventilate with bag-valve-mask, orotracheal intubation, tracheostomy, or cricothyroidotomy — must be made rapidly and correctly based on the clinical situation. The key decision point is: can the upper airway be bypassed by conventional intubation, or is the obstruction at or above the glottis preventing intubation?
Tracheostomy vs cricothyroidotomy — the critical distinction:
Cricothyroidotomy is the emergency airway procedure when the upper airway is completely obstructed AND intubation is impossible. It is performed through the cricothyroid membrane — the fibrous membrane between the inferior border of the thyroid cartilage and the superior border of the cricoid cartilage. The membrane is palpated just below the thyroid notch and above the hard cricoid ring in the midline. Technique: needle cricothyroidotomy (large-bore cannula through the membrane, connected to high-flow oxygen — provides oxygenation for approximately 30–40 minutes while a definitive airway is established); surgical cricothyroidotomy (horizontal incision through the membrane, dilate with artery forceps, insert a small cuffed tube). Cricothyroidotomy is a TEMPORARY measure — it must be converted to a formal tracheostomy within 24–48 hours because the cricoid provides the only complete ring supporting the subglottic airway, and prolonged stenting risks subglottic stenosis.
Tracheostomy is performed electively between the 2nd and 3rd tracheal rings as a planned airway procedure (e.g. for a patient with laryngeal carcinoma, for prolonged ventilation). It is not the first-choice procedure in a crash airway situation because it takes longer and requires better surgical conditions. In an impending (not complete) airway obstruction where time permits, tracheostomy under local anaesthesia is the procedure of choice.
Equipment for emergency airway:
- Suction apparatus (must be working)
- Bag-valve-mask + oxygen
- Laryngoscope + ET tubes (range of sizes)
- Cricothyroidotomy kit (needle + cannula, or scalpel + dilator + tube)
- Tracheostomy tray (scalpel, retractors, Trousseau dilator, tracheostomy tubes of varied sizes)
SELF-CHECK
A 40-year-old male arrives in casualty with severe facial trauma. He is conscious but has markedly decreased respiratory effort, blood pooling in his mouth, and a severely disrupted midface. The anaesthetist cannot intubate him. The immediate airway procedure is:
A. Tracheostomy between the 2nd and 3rd tracheal rings
B. Cricothyroidotomy through the cricothyroid membrane
C. Nasotracheal intubation
D. Bag-mask ventilation and wait for ENT
Reveal Answer
Answer: B. Cricothyroidotomy through the cricothyroid membrane
When intubation is impossible (failed airway) and the patient requires immediate ventilation, cricothyroidotomy through the cricothyroid membrane is the emergency procedure of choice. It is faster than formal tracheostomy, uses a readily accessible midline membrane, and provides immediate oxygenation. Tracheostomy is the elective airway between the 2nd and 3rd rings — it is not performed in a crash situation because it requires more surgical dissection and time. Nasotracheal intubation is contraindicated in midface fractures (risk of intracranial passage). Waiting with bag-mask ventilation is inappropriate if intubation has already failed.
Anterior Nasal Packing and Epistaxis Management Technique
Anterior nasal packing is the first-line treatment for anterior epistaxis that does not respond to simple first-aid measures (pinching the soft part of the nose for 15–20 minutes while leaning forward). The technique must be performed correctly — packing along the wrong axis or at the wrong level will compress the wrong area and fail to stop the bleeding.
First-aid measures (always attempt first):
Ask the patient to sit upright and lean FORWARD (not back — backward tilt causes blood to flow into the throat, be swallowed, and mask ongoing blood loss while causing nausea and aspiration risk). Pinch the soft cartilaginous part of the nose (NOT the bridge — the bony part) firmly between thumb and index finger for 15 minutes continuously without releasing. Apply an ice pack to the forehead and bridge of the nose. This controls the majority of anterior bleeds from Little's area.
Anterior nasal packing — technique:
Step 1 — Prepare the patient. Seat the patient with a receiver bowl under the chin. Explain the procedure. Apply a topical vasoconstrictor and local anaesthetic to the nasal cavity (e.g. Co-phenylcaine spray — lidocaine + phenylephrine) and allow 2–3 minutes for effect.
Step 2 — Identify the bleeding point. Use a headlamp and nasal speculum. The bleeding point is most commonly on the anterior nasal septum (Little's area). If visible and accessible, cauterise with silver nitrate stick (applied for 5–10 seconds to the bleeding point — NOT to both sides of the septum simultaneously, as this risks septal perforation).
Step 3 — Pack the nasal cavity. If cautery is not possible or fails:
- Merocel (BIPP or PVA foam pack): Insert the dry Merocel pack along the NASAL FLOOR (not upward — the floor direction is horizontal, posterior, and this ensures the pack reaches the posterior nasal cavity where the bleeding may be). Then irrigate with saline to expand the foam — it expands to fill the nasal cavity and compress the bleeding vessels. Bilateral packing may be required.
- Ribbon gauze (BIPP — bismuth iodoform paraffin paste): Layer the ribbon gauze in horizontal layers from the nasal floor upward, using Tilley-Henkel nasal packing forceps. The layers are packed from posterior to anterior, filling the nasal cavity layer by layer.
Step 4 — Assess result. After packing, check the oropharynx — if blood is still flowing down the posterior pharyngeal wall, the packing is inadequate (not reaching the posterior choana) or the bleed is posterior.
Posterior epistaxis — when to suspect and what to do:
If anterior packing fails to control bleeding AND blood continues to flow down the throat, the bleed is posterior (from the sphenopalatine or Woodruff's plexus). Posterior bleeds are more common in elderly, hypertensive patients. Posterior packing (Foley catheter balloon or posterior nasal balloon) is required: a Foley catheter is passed through the nose to the nasopharynx, the balloon inflated, and the catheter pulled forward to compress the posterior choana. This requires hospital admission, blood pressure control, and often ENT review for possible endoscopic sphenopalatine artery ligation.
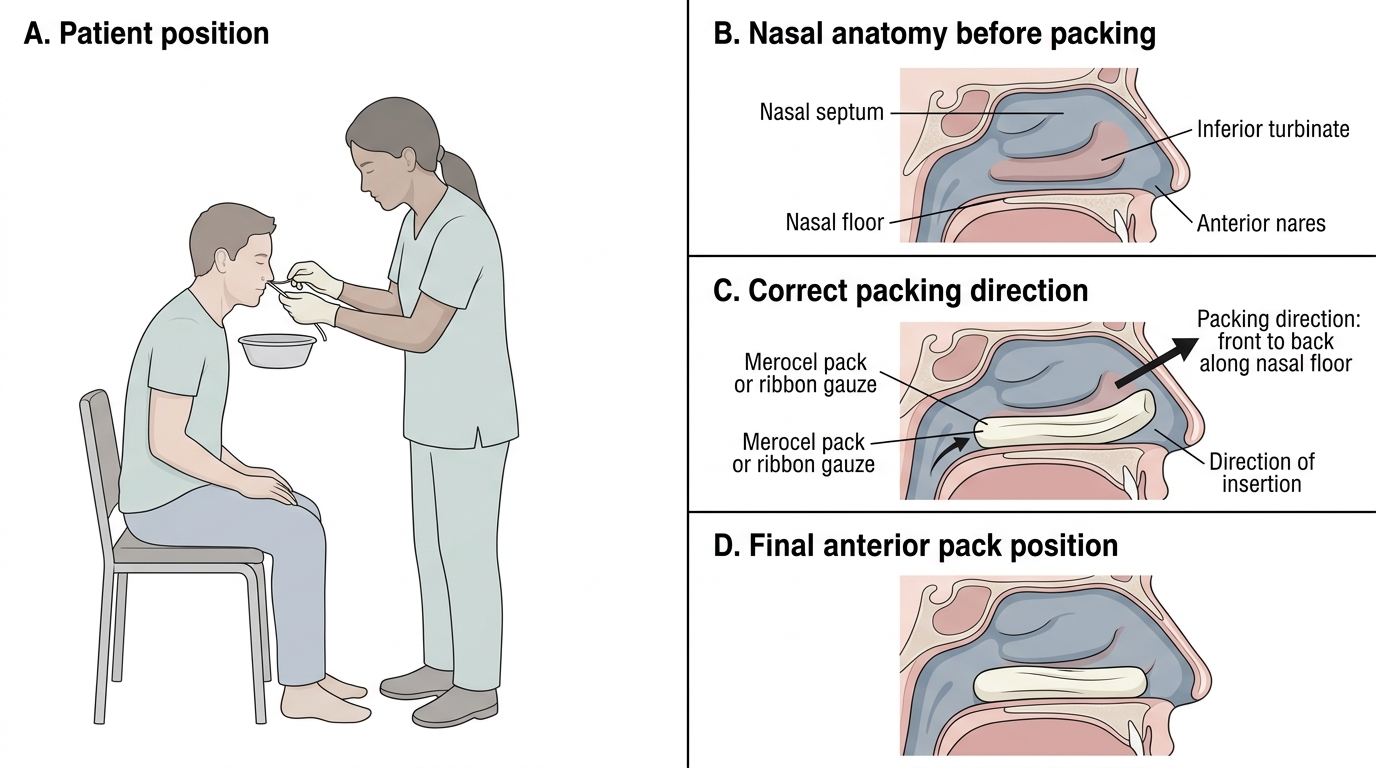
Anterior Nasal Packing Technique