Page 27 of 44
EN2.9 | ENT Surgical Consent Counselling — SDL Guide
Learning Objectives
- Describe the legal and ethical requirements for valid surgical consent
- Conduct a consent counselling session for each named ENT operation (tympanoplasty, mastoidectomy, myringotomy/grommet, FESS, septoplasty, nasal bone reduction, adenotonsillectomy, foreign body removal, tracheostomy)
- Disclose operation-specific risks using patient-appropriate language
- Respond to common patient questions and concerns about ENT surgery
- Demonstrate the consent counselling skill in a simulated environment
INSTRUCTIONS
Surgical consent is both a legal requirement and an ethical obligation. In ENT, where surgery carries specific risks (facial nerve injury, hearing loss, haemorrhage) that are not obvious to patients, the quality of consent counselling directly affects patient trust and medicolegal protection. This module teaches the structure and content of consent counselling for every ENT operation listed in EN2.9.
References
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery, 8th ed. Pre-operative counselling sections (textbook)
- Medical Council of India/NMC guidelines on informed consent (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed. Surgical consent chapters (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are about to consent a 38-year-old male schoolteacher for a mastoidectomy for cholesteatoma. His wife, who is present, asks: 'Doctor, is there any risk to the nerve of the face during this operation? My brother had facial paralysis after an ear operation somewhere else.' You have 10 minutes. How do you explain the facial nerve risk honestly, without terrifying the patient enough to refuse a surgery he medically needs — and without minimising it so much that you have failed your legal duty of disclosure?
WHY THIS MATTERS
Surgical consent in ENT is assessed at the Skills/Attitude (S/A) level in EN2.9 — meaning both the verbal communication skill and the professional attitude toward patient autonomy are being evaluated. Beyond the examination, valid consent protects the doctor legally (a patient who was not warned of a known complication can sue even if the surgery was technically perfect) and protects the patient ethically (the right to make an informed decision about their own body is foundational to medical ethics). ENT surgery carries a specific set of serious complications — facial nerve injury, sensorineural hearing loss, CSF leak — that are rare but not negligible, and that patients have no framework for anticipating without explanation. The consent counselling session is the mechanism by which the doctor transfers this understanding to the patient in an accessible, honest, and humane way.
RECALL
Recall the legal requirements for valid consent from your community medicine and medical ethics modules. Valid consent requires three elements: (1) Capacity — the patient must be mentally competent to understand the information, weigh options, and communicate a decision (adults are presumed competent unless demonstrated otherwise; for paediatric patients, parents or guardians provide consent, but the child's assent should be sought for older children); (2) Voluntariness — the decision must be free from coercion by the clinician, family, or institutional pressure; (3) Information — the patient must receive enough information to make a meaningful decision, including the nature of the procedure, its benefits, its risks (including material risks — those that a reasonable patient in the patient's position would consider significant, and any risks specific to this individual patient), alternative treatments (including no treatment), and post-operative course. The Bolam test (what a reasonable body of medical opinion would disclose) has been largely replaced in Indian and international law by a patient-centred standard: disclose what this patient would want to know. Written consent forms are documentation of the process, not a substitute for the counselling conversation.
Clinical Indication: The Purpose of Surgical Consent in ENT
Surgical consent serves three simultaneous purposes — ethical, legal, and therapeutic — and the best consent consultations serve all three simultaneously. The ethical purpose is to respect patient autonomy: the patient's right to make decisions about their own body, based on accurate and comprehensible information, is a foundational principle of modern medical ethics. The legal purpose is to establish that the patient was informed of the material risks of the procedure before consenting — this is the primary determinant of liability in consent-related litigation. The therapeutic purpose is often underappreciated: patients who have received good pre-operative counselling have lower pre-operative anxiety, better adherence to post-operative instructions, more realistic expectations of outcomes, and higher satisfaction with care — even when complications occur.
In ENT specifically, the consent consultation is heightened in importance by three factors. First, many ENT operations are performed under general anaesthesia, which itself carries risks that must be mentioned (allergic reaction, aspiration, post-anaesthetic nausea — though the anaesthetist will cover these in their own consent). Second, ENT operations carry procedure-specific risks that are invisible to the layperson: the facial nerve runs through the middle ear and mastoid — its injury is the most feared complication of mastoidectomy, and patients do not know this without being told. The orbit abuts the medial wall of the ethmoid sinus — an orbital injury is a specific risk of FESS. Third, the expected benefit of many ENT operations is improvement in function (hearing, breathing, voice) rather than cure of a life-threatening illness — patients may legitimately choose observation over surgery if they understand the risk-benefit balance.
EN2.9 lists nine specific ENT procedures for which you must be competent to counsel: tympanoplasty, mastoidectomy, myringotomy/grommet, FESS, septoplasty, nasal bone reduction, adenotonsillectomy, foreign body removal from airway/food passage, and tracheostomy.
Principles and Framework of Surgical Consent Counselling
A well-structured consent consultation follows a consistent framework regardless of the operation being discussed. The framework provides both a logical order that makes the information digestible for the patient and a completeness check that ensures all legally required elements are covered. Without a framework, consent consultations tend to be asymmetric: surgeons spend the most time on the parts they are comfortable with (the operation itself) and the least time on the parts that are most important to the patient (what could go wrong, and what happens if they choose not to proceed). The six-part framework below has been adopted from best-practice guidelines on surgical communication and is applicable to any ENT operation — and to most surgical specialties beyond ENT. Practising this framework on every consent simulation until it is automatic is the goal of this SDL section: in the OSCE, an examiner watching you consent a patient is checking whether all six elements are present, whether the risk disclosure is specific (not generic), and whether your language is appropriate for a patient without medical training.
The six-part consent consultation framework:
- Opening and context-setting: Establish rapport. Confirm the patient's identity and understanding of why they are in hospital. 'Mr Rajan, as you know, you are here today to discuss the ear operation we have planned for you. Before we proceed, I would like to explain what the operation involves, what we hope to achieve, and what risks you should be aware of. Please feel free to ask me any questions.'
- Indication: Why is this operation recommended? 'The reason we are recommending this operation is that [the cholesteatoma/the perforation/the middle ear fluid] is causing [hearing loss/risk of serious complication/recurrent infection] and we believe surgery is the best way to address this.'
- Procedure description (in lay language): What will be done? Keep this accurate but non-technical. 'During the operation, which is performed under general anaesthesia, the surgeon will make a small cut behind the ear and use a microscope to look inside the ear and remove the [abnormal skin/cholesteatoma]. This is a procedure that takes approximately 2–3 hours.'
- Benefits: What is the expected outcome? State the realistic benefit — not a guarantee. 'The main goal of this operation is to remove the disease and prevent it from spreading. In approximately 80–90% of cases, the hearing either stays the same or improves.'
- Risks (specific and general): What could go wrong? This is the most critical part and is operation-specific (see table below). Both common risks (that many patients experience) and serious risks (that are rare but severe) must be disclosed.
- Alternatives and no-treatment option: 'An alternative to surgery is to continue monitoring the ear with regular examinations and audiograms. However, cholesteatoma will continue to grow and erode bone if left untreated — the risk of serious complication (facial paralysis, meningitis) increases over time without surgery. Surgery is therefore strongly recommended.'
Consenting Technique: What to Say and How
The operation-specific risk disclosures are the most examination-critical component of this SDL. Each operation has a set of procedure-specific risks that must be mentioned, in addition to the generic risks of any surgery (bleeding, infection, anaesthetic complications, DVT).
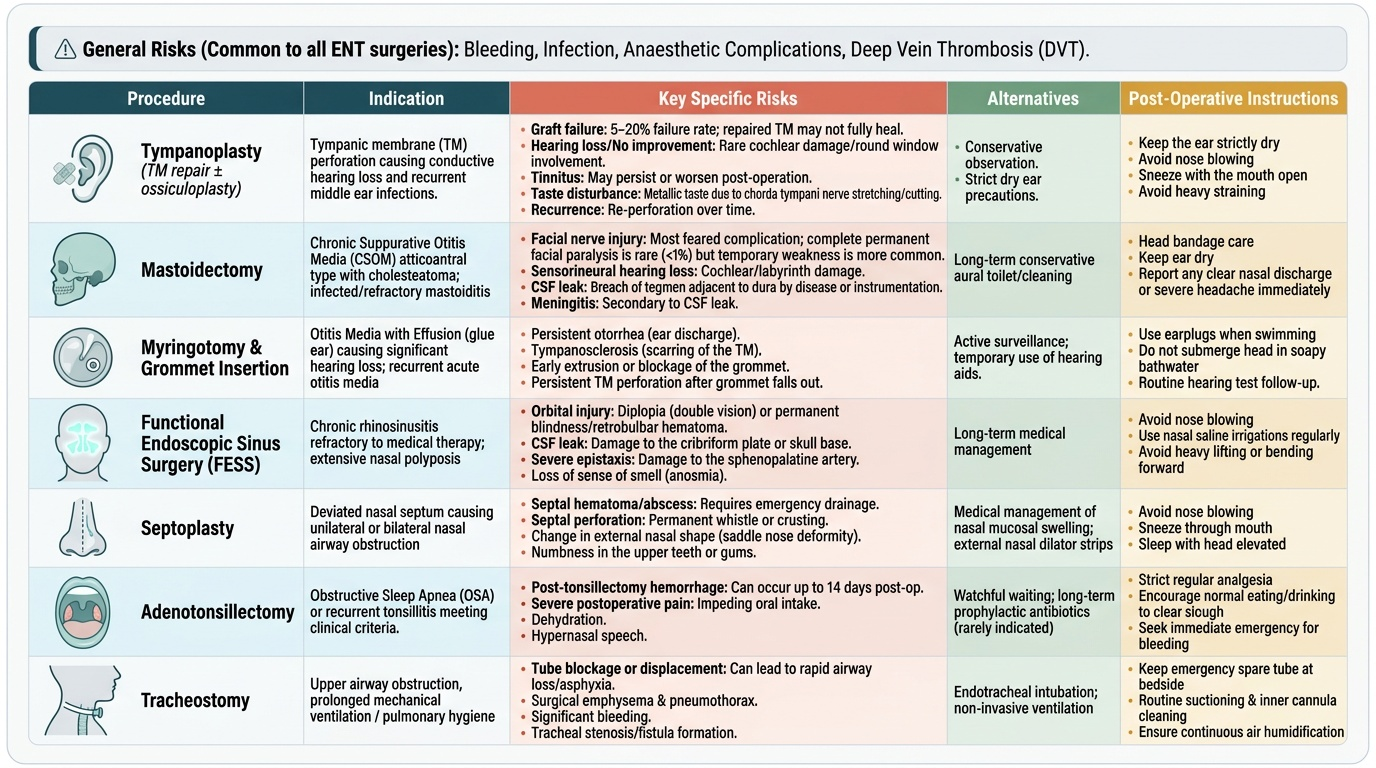
Provided image
Tympanoplasty (TM repair ± ossiculoplasty):
Indication: TM perforation causing hearing loss and recurrent infections.
Specific risks: (1) Graft failure — the repaired TM may not heal (5–20% failure rate for first operation); (2) hearing not improved or worsened — damage to the cochlea is possible but rare (round window involvement); (3) tinnitus — may persist or worsen; (4) taste disturbance — the chorda tympani nerve runs through the middle ear and may be stretched or cut, causing altered taste on the ipsilateral side (metallic taste); (5) recurrence of perforation.
Alternatives: observation and ear care (dry ear precautions); the perforation will not close spontaneously in most adults.
Mastoidectomy:
Indication: CSOM atticoantral type with cholesteatoma; infected mastoid.
Specific risks: (1) Facial nerve injury — the most feared complication; the facial nerve runs through the mastoid and middle ear in a bony canal adjacent to the surgical field. Complete facial paralysis is rare (<1%) in experienced hands but must be disclosed; temporary weakness is more common; (2) sensorineural hearing loss — damage to the cochlea or labyrinth during surgery; (3) CSF leak — if the tegmen (roof of mastoid/middle ear, adjacent to the dura) is eroded by cholesteatoma or inadvertently breached; (4) meningitis — as a consequence of CSF leak or intracranial extension; (5) dizziness/vertigo — from labyrinthine irritation; (6) recurrence of cholesteatoma (second-look surgery is sometimes required).
Alternatives: No safe alternative — cholesteatoma is progressive and fatal if left untreated.
Myringotomy + grommet insertion:
Indication: Otitis media with effusion (glue ear) causing persistent conductive hearing loss.
Specific risks: (1) Persistent perforation after grommet extrusion (1–2%); (2) tympanosclerosis (white calcification in TM); (3) recurrence of middle ear effusion after grommet falls out; (4) grommet blockage.
Alternatives: watchful waiting (OME resolves spontaneously in many children within 3 months), hearing aids.
FESS (Functional Endoscopic Sinus Surgery):
Indication: Chronic rhinosinusitis with polyps not responding to medical treatment; anatomical obstruction of ostiomeatal complex.
Specific risks: (1) Orbital injury — the medial wall of the ethmoid (lamina papyracea) is paper-thin and adjacent to the orbit; breach can cause orbital haematoma, diplopia, or rarely visual loss; (2) CSF leak — through the cribriform plate/anterior skull base, with risk of meningitis; (3) bleeding; (4) recurrence of polyps (FESS controls, does not cure, allergy-driven polyposis); (5) loss of smell (anosmia).
Alternatives: prolonged nasal steroid therapy, saline irrigation; appropriate if disease is mild.
Adenotonsillectomy:
Indication: Recurrent tonsillitis, obstructive sleep apnoea due to tonsillar hypertrophy.
Specific risks: (1) Primary haemorrhage — within 24 hours of surgery; requires return to theatre; (2) secondary haemorrhage — most common, occurring on days 5–10 post-operatively when the slough over the tonsillar fossa separates; may require return to theatre and is potentially life-threatening; (3) throat pain — significant for 10–14 days post-operatively; (4) velopharyngeal insufficiency (hypernasal voice, very rare — more common in patients with submucous cleft palate); (5) anaesthetic complications.
Post-operative instructions: soft diet for 2 weeks; no aspirin or NSAIDs (anti-platelet effect increases bleeding risk); return to hospital immediately if any bleeding from the mouth or vomiting of blood.
Tracheostomy:
Indication: Upper airway obstruction, prolonged ventilation, failed intubation.
Specific risks: (1) Haemorrhage — from the thyroid or innominate artery (if tracheostomy is performed too low); (2) tube displacement — displacement before the tract is established (within 7–10 days) is a surgical emergency; (3) subcutaneous emphysema and pneumothorax; (4) tracheomalacia — softening of the tracheal wall at the cuff site with long-term tubes; (5) swallowing and speech difficulty (tube occludes larynx partially); (6) scarring of the anterior neck.
Post-operative care: inner cannula cleaning twice daily; humidification of inhaled air; suction as needed; regular wound care.
SELF-CHECK
During adenotonsillectomy consent, a parent asks: 'If there is bleeding after the operation, when does it most commonly happen?' The correct answer is:
A. Immediately in the recovery room, before the patient wakes up
B. During the first 24 hours (primary) or most commonly on days 5–10 (secondary) when the slough separates
C. Only if the patient eats hard food on the first post-operative day
D. Bleeding is rare and occurs only in patients on blood-thinning medications
Reveal Answer
Answer: B. During the first 24 hours (primary) or most commonly on days 5–10 (secondary) when the slough separates
Post-tonsillectomy haemorrhage has two distinct types: primary (within 24 hours, usually due to inadequate haemostasis at surgery) and secondary (most common, on days 5–10 post-operatively when the slough over the tonsillar fossa separates). Secondary haemorrhage is the most important to warn patients and families about because it occurs after hospital discharge, at home, and can be life-threatening. Parents must be explicitly told to return to hospital immediately if any bleeding from the mouth occurs in the first 2 weeks after surgery.