Page 20 of 44
EN2.7 | ENT Surgical Instruments — SDL Guide
Learning Objectives
- Identify and name the common instruments used in nasal surgery (FESS, septoplasty, nasal bone reduction)
- Identify and name the common instruments used in ear surgery (tympanoplasty, mastoidectomy, myringotomy)
- Identify and name the common instruments used in throat and airway surgery (adenotonsillectomy, foreign body removal, tracheostomy)
- Describe the function and surgical context of each instrument
- Match a set of instruments to the correct ENT surgical procedure
INSTRUCTIONS
ENT surgical instrument knowledge is tested in OSCEs through instrument identification stations, where you are shown a physical instrument or photograph and asked to name it and describe its use. This module systematically covers the key instruments for all three ENT regions, with emphasis on function and clinical context rather than rote naming.
References
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery, 8th ed. Surgical chapters (textbook)
- Hazarika P. Textbook of Ear, Nose and Throat & Head Neck Surgery, 3rd ed. Surgical instruments chapter (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed. Surgical technique chapters (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are in the ENT OSCE examination. The examiner places a curved metal instrument on the table — it has two blades connected at a pivot, with the blades designed to open in a controlled way when a handle is squeezed. She asks: 'Name this instrument, describe its parts, and tell me in which ENT surgery it is used and at which anatomical site.' Then she replaces it with a long-handled instrument with a cup-shaped end and asks the same questions. Can you answer both?
WHY THIS MATTERS
Instrument knowledge is a component of surgical readiness — the ability to assist at and eventually perform ENT operations. EN2.7 is a Knowledge/Habit (K/SH) competency: you must be able to identify instruments and describe their use in the named operations. Beyond the examination, this knowledge matters in the operating theatre when you are asked to pass instruments, set up the trolley, or understand what the surgeon is doing. It also provides the conceptual framework for understanding ENT surgical procedures — knowing that a myringotomy requires a dedicated knife and that the antero-inferior quadrant is the safe site means you understand WHY the surgery is performed there, not just that it is.
RECALL
Recall the anatomical structures relevant to each surgical region. The nasal cavity is divided by the septum into two passages; the paranasal sinuses drain via the ostiomeatal complex. The septum consists of the quadrilateral cartilage (anterior) and the perpendicular plate of the ethmoid and vomer (posterior bony parts). The tympanic membrane is divided into four quadrants by the handle of malleus (vertical line) and a horizontal line through the umbo: antero-superior, antero-inferior, postero-superior, and postero-inferior. Safe myringotomy site: antero-inferior quadrant — the ossicles are positioned supero-posteriorly, and the jugular bulb is infero-posteriorly. The trachea is a midline structure; the cricothyroid membrane lies between the thyroid cartilage and cricoid cartilage, accessible for emergency airway. Tracheal rings 2 and 3 are the standard tracheostomy site — not ring 1 (risk of subglottic stenosis) and not too low (risk of innominate artery erosion).
Clinical Indication: Why ENT Instrument Knowledge Matters
ENT surgery is a specialty that relies on a distinctive set of specialised instruments, many of which are unique to the specialty and unrecognisable without specific training. Unlike general surgery, where instruments are largely standardised across procedures, ENT instruments are often procedure-specific and region-specific: the Boyle-Davis gag is used only in adenotonsillectomy; the Hopkins rod endoscope is specific to nasal endoscopy and FESS; the Rosen needle and Plester knife are used exclusively in middle ear microsurgery. This specificity means that instrument identification in ENT functions as a proxy test for procedural knowledge: a student who can correctly identify the Trousseau dilator and explain that it is used to dilate the tracheal incision during tracheostomy has demonstrated understanding of the tracheostomy procedure, not merely a memory feat.
The EN2.7 competency specification is comprehensive: it covers instruments for six named ENT operations (FESS, septoplasty, nasal bone reduction, tympanoplasty, mastoidectomy, myringotomy for the nose and ear; and adenotonsillectomy, foreign body removal from airway and food passage, and tracheostomy for the throat and airway). This module covers each operation's key instruments with their function and the anatomical context that explains their design.
A secondary clinical reason for this knowledge is patient safety: the doctor who knows ENT instruments can more accurately assist in emergency procedures — particularly emergency airway management (where Trousseau dilators and tracheostomy tubes are used) and foreign body removal (where the choice between oesophagoscope and Chevalier Jackson laryngoscope depends on the level of the foreign body). These are situations where instrument confusion can cost a life.
Nasal Surgical Instruments
Nasal surgery encompasses three distinct procedural categories, each with its own instrument set. Understanding the anatomical target of each procedure explains why each instrument has its specific design.
FESS (Functional Endoscopic Sinus Surgery) instruments:
Hopkins rod endoscope (rigid nasal endoscope): A rigid rod-lens telescope available in multiple angles — 0° (straight forward view, for the nasal cavity and nasopharynx), 30° (angled upward, for the middle meatus and ethmoid bulla), 45° and 70° (for the frontal recess and sphenoid). The rod lens system provides a wide, bright image through a narrow diameter shaft. Connected to a camera and monitor for image-guided surgery.
Blakesley-Weil forceps (through-cutting forceps): Straight or angled cup-shaped forceps used to bite away ethmoidal air cells and polyps during FESS. The cup-bite design allows tissue to be bitten, not torn — reducing bleeding.
Stammberger punch forceps: Angled cutting forceps for opening the maxillary ostium and removing tissue from the ostiomeatal complex.
Microdebrider (powered shaver): A powered instrument with a rotating blade and suction; used for removal of polyps and soft tissue in FESS with simultaneous aspiration of debris.
Septoplasty instruments:
Killian nasal speculum: Long-bladed bivalve speculum used in septoplasty to retract the nasal alae and provide access to the nasal cavity under direct vision or endoscopic control. Distinct from the short Thudichum speculum used for bedside examination.
Cottle's elevator (Cottle's knife-elevator): A flat instrument with one side sharp (to incise the mucoperichondrium) and one side blunt (to elevate the mucoperichondrial flap from the cartilage). Used to raise the septal flap that allows access to the septal cartilage and bone.
Freer's periosteal elevator: Double-ended elevator with one sharp and one blunt end; used similarly to Cottle's for mucoperichondrial and mucoperiosteal elevation from the septal cartilage and bony septum.
Nasal bone reduction instruments:
Walsham's forceps: Designed for closed reduction of fractured nasal bones. One blade is introduced inside the nasal cavity along the lateral wall; the other is placed externally over the displaced nasal bone. The two blades are then squeezed together to manipulate the fractured nasal bone back into position.
Ash's (Boies) forceps: Similar in function to Walsham's forceps, used for nasal bone reduction.
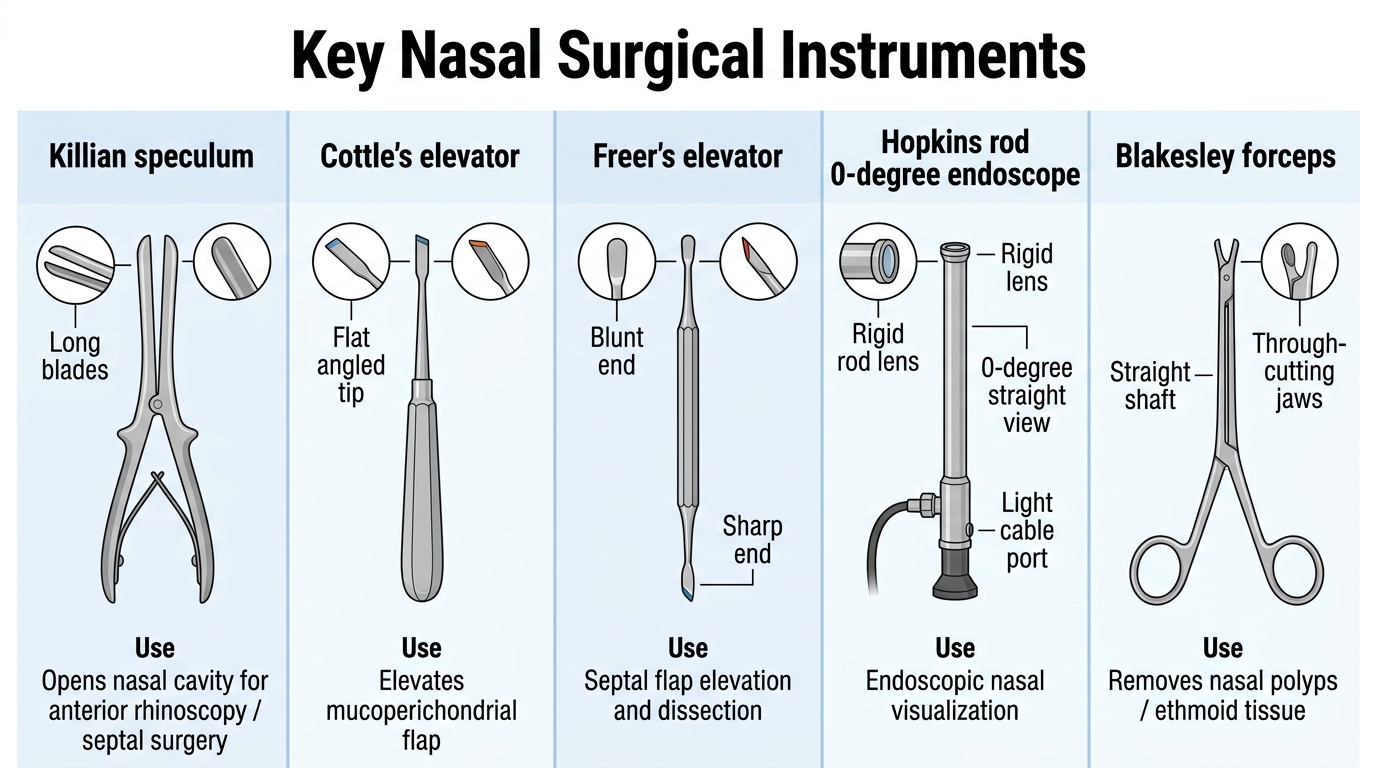
Key Nasal Surgical Instruments
Ear Surgical Instruments
Ear surgery is performed under an operating microscope because the structures of the middle ear — ossicles, facial nerve, chorda tympani, tympanic membrane — are millimetres in size and require high magnification and co-axial illumination to operate safely. The instruments are correspondingly miniaturised, and their design is dictated by the need to work within the narrow confines of the external auditory canal and middle ear space.
Tympanoplasty instruments:
Operating microscope: The essential enabling instrument for all middle ear surgery. Provides 6–40× magnification with coaxial illumination through a lens system. The surgeon operates through the eyepieces while instruments are passed through the EAC.
Hartmann (aural) speculum: A cone-shaped metal speculum that dilates and holds open the EAC during operating microscope-based ear surgery, providing a clear working channel to the TM and middle ear.
Rosen needle (Rosen's elevator): A right-angled needle used to elevate the tympanomeatal flap (TM and attached canal skin) to enter the middle ear space. The sharp angled tip cuts the incisions needed to reflect the flap.
Plester knife (Plester's sickle knife): A sickle-shaped microscalpel used to make circumferential incisions in the EAC skin and TM margin during tympanoplasty.
Mastoidectomy instruments:
Mollison's (Weitlaner) self-retaining retractor: Placed in the post-auricular incision wound to hold the skin and soft tissue back and provide a clear operating field for mastoid access.
Lempert's periosteal elevator: Used to elevate the periosteum from the mastoid cortex, exposing the mastoid bone before drilling.
Mastoid chisels and bone curettes: Used to remove the mastoid cortex and exenterate mastoid air cells. Bone curettes are used to remove softer bone and granulation tissue.
Mastoid drill (electric burr): The principal tool for modern mastoidectomy; removes bone with rotating carbide or diamond-coated burrs of varying sizes. Larger cutting burrs for initial cortex removal; smaller diamond burrs near the facial nerve canal and ossicles.
Myringotomy instruments:
Myringotomy knife (Beaver blade): A very small, curved blade used to make the myringotomy incision in the antero-inferior quadrant of the TM. The small size and precise curve allow the incision to be made in the correct quadrant without trauma to surrounding structures.
Grommet (ventilation tube) inserter: A fine forceps used to insert a small ventilation tube (grommet) through the myringotomy incision into the middle ear, to maintain middle ear ventilation in otitis media with effusion.
SELF-CHECK
The safe site for a myringotomy incision is the antero-inferior quadrant of the TM. The main reason for avoiding the postero-superior quadrant is:
A. The postero-superior quadrant is too thick for a blade to penetrate
B. The ossicular chain (incus and stapes) lies postero-superiorly, and a blade in that quadrant risks ossicular damage
C. The light reflex is in the postero-superior quadrant, and it must be preserved
D. The postero-superior quadrant has the poorest blood supply and heals poorly after incision
Reveal Answer
Answer: B. The ossicular chain (incus and stapes) lies postero-superiorly, and a blade in that quadrant risks ossicular damage
The antero-inferior quadrant is the safe site for myringotomy because the ossicular chain — specifically the incudo-stapedial joint and the stapes — lies in the postero-superior quadrant. A myringotomy blade in the postero-superior quadrant risks penetrating and dislocating the stapes, causing sensorineural hearing loss. The jugular bulb lies infero-posteriorly, making the postero-inferior quadrant also relatively unsafe. The antero-inferior quadrant is the anatomically safest location.