Page 37 of 44
EN2.12 | National ENT Prevention Programs — SDL Guide
Learning Objectives
- Describe the objectives, target populations, and components of the National Programme for Prevention and Control of Deafness (NPPCD)
- Explain the 1-3-6 rule for newborn hearing screening and its importance
- Describe the prevention strategies for noise-induced hearing loss and the relevant occupational exposure limits
- Identify the significance of World Hearing Day (3 March) and Deafness Week as public health activities
- Describe the role of the clinician in national ENT cancer prevention programs (NTCP)
INSTRUCTIONS
ENT prevention programs operate at the intersection of clinical medicine and public health. Understanding these programs is required for EN2.12 (KH level) and for participation in the community-based activities that the NMC mandates during your clinical posting. This module covers the key national programs relevant to ENT — deafness prevention (NPPCD), noise control, cancer prevention (NTCP), and the awareness campaigns that every medical graduate is expected to participate in.
References
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery, 8th ed. Appendix: National Health Programs (textbook)
- Ministry of Health and Family Welfare, India. NPPCD Programme Guidelines (textbook)
- WHO. World Hearing Day Reports; Noise and Health WHO guidelines (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is World Hearing Day (3 March). Your medical college has organised a free hearing screening camp at a nearby government school. You are part of the student team. A teacher brings a 6-year-old girl who 'doesn't pay attention in class' and 'doesn't respond when called.' On screening with an otoacoustic emission (OAE) device, you get a 'refer' result bilaterally. Her parents say 'she has always been a quiet child; we thought she was just shy.' What does this result mean — and what does your program require you to do next?
WHY THIS MATTERS
EN2.12 is unique among the ENT competencies in that it is designated Knowledge/Habit (KH) level — meaning the competency is assessed not only on what you know but on habitual participation: you must actively participate in deafness week and World Hearing Day activities, not merely be able to describe them. This reflects the NMC's recognition that prevention programs in India succeed or fail based on whether healthcare professionals at the community level are actively engaged in them. India has an estimated 63 million people with significant hearing loss, making it the second highest burden country for hearing loss globally. The majority of this burden is preventable — through newborn screening, avoidance of ototoxic medications, noise control, and early intervention for otitis media. A doctor who knows about these programs but does not participate in them is leaving preventable disability unaddressed.
RECALL
Recall from your community medicine and preventive medicine curriculum: the primary, secondary, and tertiary prevention framework. Primary prevention removes the cause of disease before it occurs (noise protection, tobacco cessation, maternal rubella vaccination). Secondary prevention detects disease at the earliest possible stage when treatment is most effective (newborn hearing screening, audiological screening in schools). Tertiary prevention reduces the impact of established disease (hearing aids, cochlear implants, rehabilitation). The NPPCD operates across all three levels. Recall also from physiology: OAE (otoacoustic emissions) are sounds generated by the outer hair cells of the cochlea in response to an acoustic stimulus — a device measures these emissions. If the outer hair cells are functioning normally, OAEs are detected ('pass'); if damaged (from congenital SNHL, noise, ototoxicity), OAEs are absent ('refer'). OAE is an objective, non-invasive test requiring no behavioural response — making it ideal for screening neonates and young children.
Clinical Indication: Why National ENT Programs Matter to the Clinician
National prevention programs are not abstract public health policy — they are the institutional infrastructure that allows individual clinicians to deliver preventive care at scale, and their effectiveness depends directly on whether clinicians at the point of care understand and apply their protocols. The ENT prevention programs in India address three distinct disease burdens: (1) hearing loss and deafness (affecting approximately 6.3% of the Indian population, with over a million children born with significant hearing loss each year); (2) noise-induced hearing loss (affecting millions of industrial and agricultural workers); and (3) head-and-neck cancer (India has among the highest rates of oral and laryngeal cancer globally, driven by tobacco and betel nut use).
The clinical relevance of these programs to the individual doctor is threefold. First, the doctor is a screener: every encounter with a young child, a factory worker, or a tobacco user is an opportunity to apply program screening protocols — asking about hearing, checking occupational noise exposure, or examining the oral cavity for premalignant lesions. Second, the doctor is a referrer: a patient who screens positive (a child with abnormal OAE, a worker with a 4 kHz notch on audiogram, a patient with leukoplakia) needs to be referred through the correct program pathway for diagnosis, intervention, and follow-up. Third, the doctor is an educator: prevention programs succeed when communities receive accurate information about risk factors, protective behaviours, and available services — and doctors are the most trusted source of health information in most Indian communities.
The NMC specifically mandates participation in Deafness Week and World Hearing Day as a component of ENT competency attainment — recognising that these national awareness events are the primary mechanism by which prevention messages reach community level, and that medical students represent a large, available, motivated workforce for community health education.
National Programme for Prevention and Control of Deafness (NPPCD)
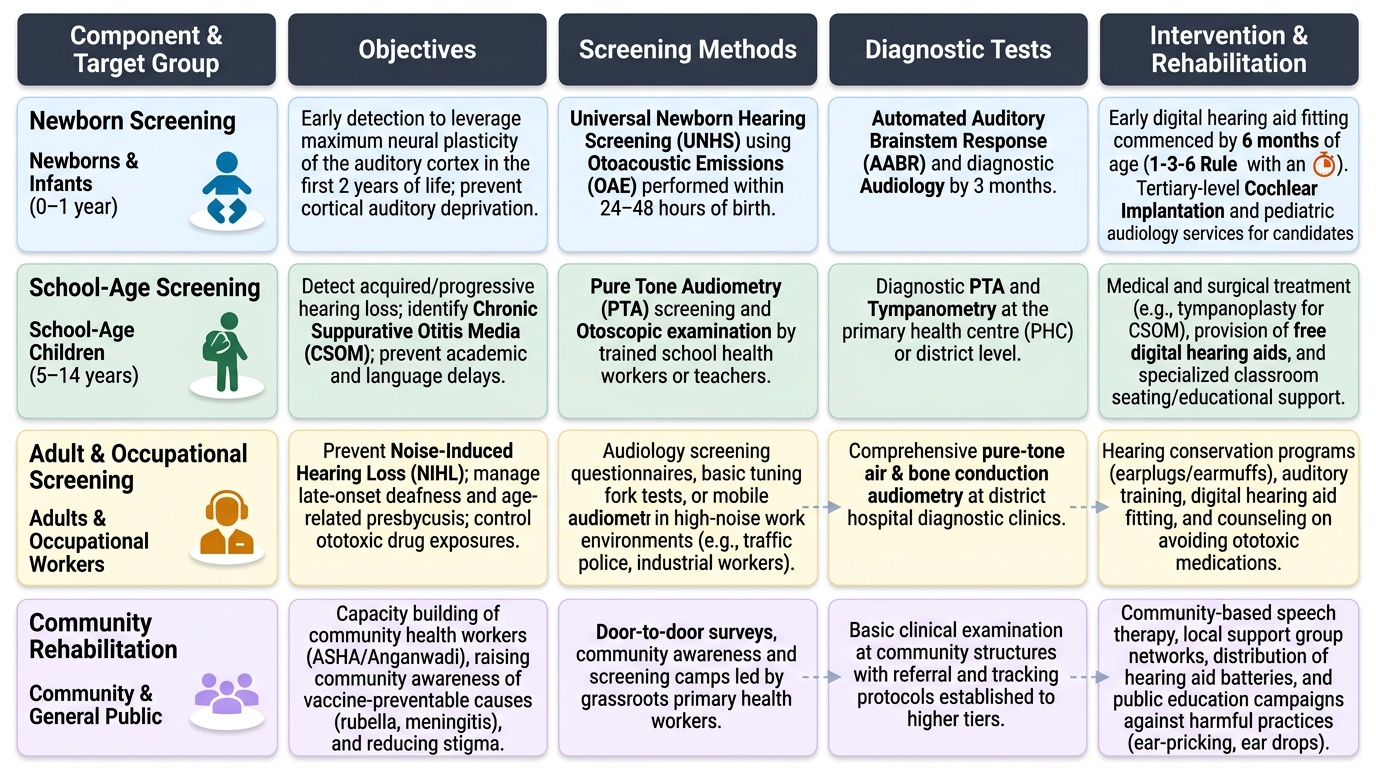
The NPPCD (National Programme for Prevention and Control of Deafness) was launched in 2006 by the Ministry of Health and Family Welfare, Government of India, and has been integrated into the National Health Mission (NHM) framework. It addresses the full spectrum of hearing loss prevention, early detection, and rehabilitation across all age groups. India's hearing loss burden justifies the programme's ambition: with an estimated 63 million persons affected by significant hearing loss, and over 100,000 children born deaf every year, India has one of the highest absolute burdens of hearing disability globally. The majority of this disability is preventable or reversible if identified early — which is the central premise of the NPPCD. The programme operates through a cascading service delivery system: at the community level, health workers conduct screening camps and distribute awareness messages; at the primary health centre level, audiological screening devices are provided and referral protocols are implemented; at the district level, audiological clinics provide diagnostic testing and hearing aid fitting; and at the apex level, tertiary ENT centres provide cochlear implantation and paediatric audiology services.
Provided image
Programme objectives:
1. Prevention of avoidable causes of hearing loss (e.g. ototoxic medications, noise, vaccine-preventable causes such as rubella and meningitis).
2. Early identification of hearing loss at the earliest possible stage.
3. Rehabilitation of persons with hearing loss through hearing aids, speech therapy, and cochlear implantation for eligible candidates.
4. Capacity building of healthcare workers at all levels for hearing screening and early intervention.
Target populations and screening strategies:
Newborns: Universal newborn hearing screening (UNHS) using OAE (otoacoustic emissions) as the primary screening tool. OAE is performed within 24–48 hours of birth or before discharge from hospital. The international target, adopted by NPPCD guidelines, is the 1-3-6 rule: hearing loss identified by 1 month, diagnosed by 3 months, and intervention (hearing aid fitting) commenced by 6 months of age. Early fitting is critical — the auditory cortex has maximum plasticity in the first 2 years of life; delayed amplification results in cortical auditory deprivation and permanent deficits in speech and language development even if the peripheral hearing loss is corrected later.
School-age children: Audiological screening at entry into school and at regular intervals, using pure tone screening audiometry (500, 1000, 2000, 4000 Hz at 20–25 dB HL as the pass criterion). Detects acquired hearing loss from otitis media, noise, or other causes that were not present at birth.
Adults and occupational groups: Audiological surveillance for workers in high-noise industries (manufacturing, construction, mining, agriculture) — serial PTA to detect the emerging 4 kHz notch of noise-induced hearing loss. Linked to occupational health regulations.
Community rehabilitation: Hearing aid dispensing through government programs; cochlear implantation for children with profound bilateral SNHL not benefiting from hearing aids (ADIP scheme — Assistance to Disabled Persons, under the Ministry of Social Justice).
SELF-CHECK
According to the 1-3-6 rule for newborn hearing screening under NPPCD, by what age should a hearing aid be fitted for a child diagnosed with significant congenital hearing loss?
A. By 1 month of age
B. By 3 months of age
C. By 6 months of age
D. By 12 months of age
Reveal Answer
Answer: C. By 6 months of age
The 1-3-6 rule: hearing loss identified by 1 month (OAE screening at birth), diagnosed by 3 months (diagnostic audiometry confirming degree and type), and intervention (hearing aid fitting) commenced by 6 months of age. The 6-month target for hearing aid fitting is critical because the auditory cortex is maximally plastic in the first 2 years of life; fitting before 6 months optimises speech and language development outcomes. Delay to 12 months or beyond results in auditory cortex deprivation effects that cannot be fully reversed even with late hearing aid fitting.
Noise and Environmental Pollution: Prevention and Programme Components
Noise-induced hearing loss (NIHL) is the most prevalent preventable cause of occupational hearing loss worldwide, and it is entirely irreversible once established — unlike conductive hearing loss from otitis media, SNHL from cochlear hair cell death does not recover. The prevention strategy is therefore primary prevention: reduce exposure before damage occurs.
Occupational noise standards:
The international and Indian occupational safety standard (per the Factories Act 1948 and NIOSH/WHO guidelines) sets the permissible noise exposure limit at 85 dB(A) for 8 hours per day as a time-weighted average. This is equivalent to the 85 dB(A) action level, above which hearing protection must be provided and audiological surveillance must be conducted. For every 3 dB increase in noise level, the permissible exposure duration is halved (the 3 dB exchange rate): at 88 dB(A), maximum 4 hours; at 91 dB(A), maximum 2 hours; at 94 dB(A), maximum 1 hour.
Engineering controls (preferred over PPE):
- Reduce noise at source: quieter machinery, enclosures, mufflers.
- Increase distance between worker and noise source.
- Reduce transmission: acoustic barriers, sound-absorbing materials.
Personal protective equipment (PPE):
Ear muffs or ear plugs when engineering controls are insufficient. Ear plugs (foam or pre-moulded) reduce noise by 15–30 dB; ear muffs reduce noise by 25–35 dB. Custom-moulded ear plugs are the most comfortable for all-day use.
Environmental noise:
Urban environmental noise from traffic, construction, and entertainment venues is a significant public health concern. WHO guidelines recommend outdoor noise below 55 dB(A) day-time and below 40 dB(A) night-time for community health. Fireworks, music concerts (>100 dB), and heavy traffic are common causes of acute acoustic trauma and recreational NIHL. The WHO/ITU 'Safe Listening' standard for personal audio devices recommends limiting exposure to 80 dB(A) for a maximum of 40 hours per week.
Medical prevention of NIHL:
- Avoid ototoxic drugs when alternatives exist (aminoglycosides, cisplatin, loop diuretics at high doses) — particularly in patients already exposed to industrial noise.
- Treat acute otitis media and chronic ear disease early to prevent additional acquired hearing loss.
- Genetic counselling for hereditary hearing loss.
Student participation activities (NMC mandate):
- Organising noise awareness stalls at college health fairs.
- Distributing hearing protection information leaflets in industrial areas, construction sites, and farming communities.
- School education programs on 'safe listening' and personal audio device use.
- Participation in World Hearing Day camps (3 March): OAE screening, PTA, and hearing health counselling.