Page 25 of 44
EN2.8 | Premalignant and Malignant ENT Screening — SDL Guide (Part 2)
Recognising Premalignant and Malignant Lesions by Site
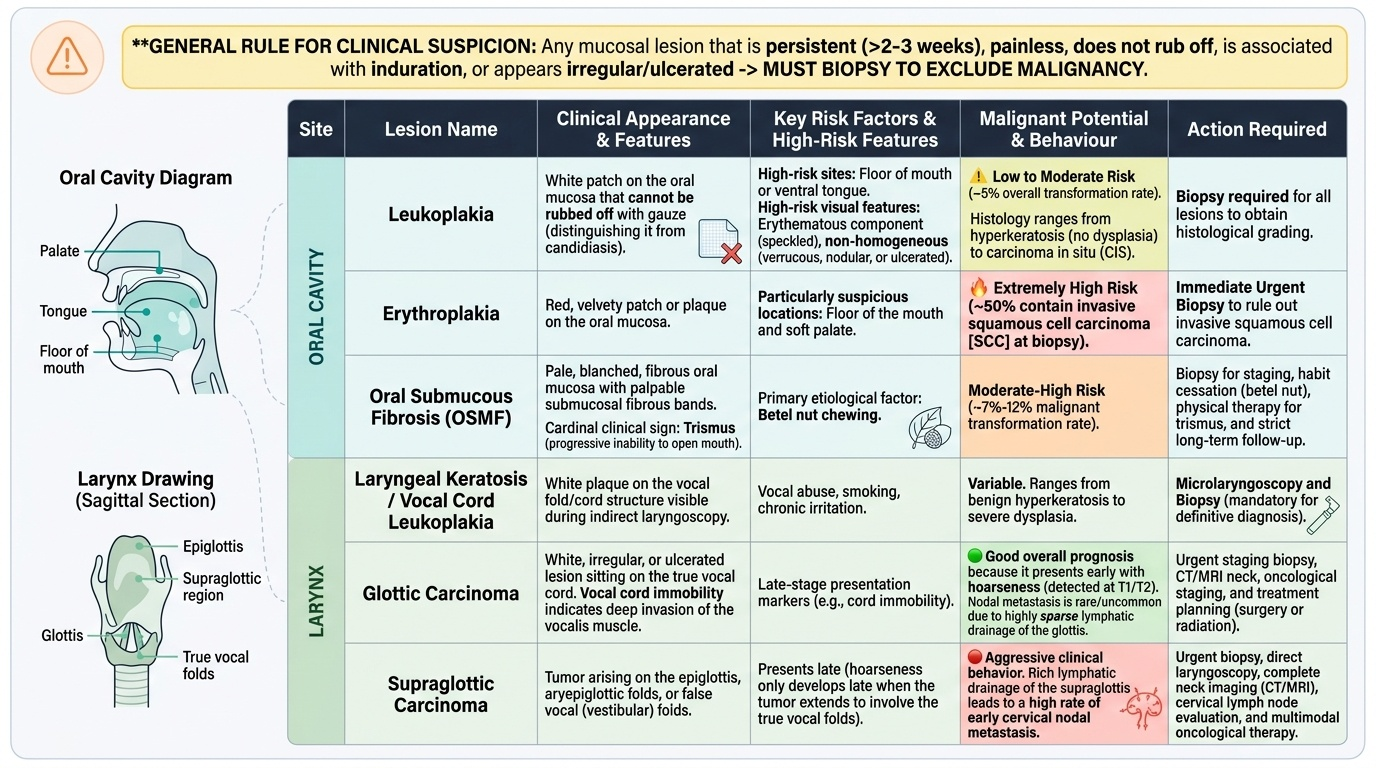
Site-specific recognition is the most directly testable component of EN2.8. The following summary covers the key lesions at each anatomical site, their appearance, and their clinical significance. The principle of recognition is simple: any mucosal lesion that is persistent (>2–3 weeks), painless, does not rub off, is associated with induration, or appears irregular or ulcerated must be biopsied to exclude malignancy.
Provided image
Oral cavity premalignant lesions:
Leukoplakia: A white patch on the oral mucosa that cannot be rubbed off with a gauze (distinguishes it from candidiasis, which CAN be rubbed off). Histologically ranges from hyperkeratosis (no dysplasia) to carcinoma in situ. Overall malignant transformation rate approximately 5%. Higher risk: lesion on the floor of the mouth or ventral tongue; erythematous component (speckled leukoplakia); non-homogeneous (verrucous, nodular, or ulcerated surface). All leukoplakia requires biopsy for histological grading.
Erythroplakia: A red velvety patch on the oral mucosa. Far higher malignant transformation rate than leukoplakia (approximately 50% contain invasive SCC at biopsy). Lesions on the floor of mouth and soft palate are particularly suspicious.
Oral submucous fibrosis (OSMF): Pale, blanched, fibrous oral mucosa with palpable submucosal fibrous bands; trismus is the cardinal clinical sign (progressive inability to open the mouth due to fibrosis of the pterygomandibular raphe and buccal mucosa). Caused by betel nut chewing. Premalignant — malignant transformation rate approximately 7–12%.
Laryngeal lesions:
Laryngeal keratosis / vocal cord leukoplakia: White plaque on the vocal cord seen at indirect laryngoscopy. May be benign hyperkeratosis or contain dysplasia. All cases require microlaryngoscopy and biopsy.
Glottic carcinoma: White, irregular, or ulcerated lesion on the true vocal cord; vocal cord immobility on indirect laryngoscopy = deep invasion of the vocalis muscle. Presents early with hoarseness (hence good prognosis — most are detected at T1/T2). Lymphatic drainage of the glottis is sparse — nodal metastases are uncommon in early disease, unlike supraglottic carcinoma.
Supraglottic carcinoma: Arises from the epiglottis, aryepiglottic folds, or vestibular folds. Presents late — hoarseness occurs only when the vocal cord is involved. Cervical nodal metastases are common at presentation due to rich supraglottic lymphatic drainage.
CLINICAL PEARL
The single most dangerous clinical mistake in ENT cancer screening is reassuring a patient with a persistent mucosal lesion because it is 'painless.' Oral SCC and laryngeal SCC are classically painless in the early stages — pain develops with infiltration of pain-sensitive structures (nerves, bone, muscle), which occurs only in more advanced disease. A painless white patch, a painless ulcer, or a painless neck node in an adult with risk factors is a cancer until proven otherwise. Painlessness is NOT reassuring in ENT oncology — it is the reason these cancers are detected late.
Applied Practice: Screening Scenarios
These scenarios represent the clinical encounters in which ENT cancer screening is most commonly performed. For each scenario, identify the lesion, categorise it (premalignant or malignant), and state the appropriate action — including whether biopsy is indicated and how urgently.
Scenario 1 — Oral leukoplakia in a tobacco user:
A 48-year-old male gutka chewer presents with a white patch on the right buccal mucosa present for 6 months. The patch is well-defined, homogeneous white, and cannot be rubbed off. No ulceration. No adjacent erythema. Mouth opens fully.
Classification: Premalignant — leukoplakia (homogeneous type, lower immediate risk than speckled or erythroplakic variants).
Action: Biopsy under local anaesthesia for histological grading (the clinical appearance cannot grade dysplasia; only histology can). Advise cessation of gutka and tobacco. Follow up the histology result to determine if treatment (laser excision, topical vitamin A) is required.
Scenario 2 — Supraglottic carcinoma:
A 60-year-old male smoker presents with 4 months of difficulty swallowing (dysphagia), right otalgia (referred via CN X), and recently noticed a right neck swelling. His voice is currently normal. Indirect laryngoscopy: there is an irregular, friable, red-grey mass on the right epiglottis and aryepiglottic fold. The vocal cords are mobile bilaterally.
Classification: Malignant — supraglottic carcinoma (SCC most likely). Mobile vocal cords = T3 or lower. Cervical node = N+ at presentation.
Action: Urgent referral to ENT oncology. CT neck and thorax for staging. Panendoscopy under GA for biopsy. The otalgia (referred via vagus) and neck node at presentation are typical of supraglottic carcinoma. The voice is normal because the vocal cords are not yet involved — this is why supraglottic carcinoma presents late.
Scenario 3 — Neck node with unknown primary:
A 55-year-old female non-smoker, non-drinker presents with a painless right neck swelling at level II, 3 × 3 cm, firm, for 8 weeks. She has no nasal, throat, or ear symptoms. Oral cavity and oropharynx examination appear normal. Indirect laryngoscopy: normal.
Action: FNAC of the neck node (first-line tissue investigation). If FNAC = SCC: imaging (CT neck + chest) + panendoscopy under GA to find the primary (nasopharyngoscopy and biopsy of Waldeyer's ring even when grossly normal — SCC in a neck node from an unknown primary in a non-smoker raises the probability of HPV-related oropharyngeal carcinoma or NPC). A negative FNAC does not exclude malignancy — if the node persists, repeat FNAC or excision biopsy.
Self-Assessment: ENT Cancer Screening Competency Check
Test your recognition and risk stratification skills with these questions.
Q1: Describe the difference between leukoplakia and oral candidiasis on examination. Why does this distinction matter clinically?
Answer: Leukoplakia is a white patch that CANNOT be rubbed off — it is a keratotic/dysplastic epithelial change. Candidiasis is a white patch that CAN be rubbed off with a gauze, leaving a red, bleeding base — it is a fungal infection. This distinction is critical because leukoplakia requires biopsy and follow-up for malignancy risk, while candidiasis requires antifungal treatment. Confusing the two means either missing a premalignant lesion (if you treat leukoplakia as candidiasis) or subjecting a patient to unnecessary biopsy (if you biopsy every candidal lesion).
Q2: A patient with oral submucous fibrosis can open his mouth only 2 cm. What is the pathogenesis, the causative habit, and the malignancy risk?
Answer: OSMF is caused by betel nut (areca nut) chewing. Arecoline (the active alkaloid) stimulates fibroblasts to produce excess collagen in the submucosal layer. Progressive fibrosis of the buccal mucosa, pterygomandibular raphe, and palate causes progressive trismus (reduced mouth opening, normal = >3.5 cm). Malignant transformation rate approximately 7–12%. The pallor and fibrous texture of the mucosa are visible on examination.
Q3: Why does glottic carcinoma present earlier and have a better prognosis than supraglottic carcinoma?
Answer: Glottic carcinoma (vocal cord) presents early because even a small lesion causes hoarseness — the vocal cord's function (phonation) is immediately impaired. The glottis has sparse lymphatic drainage — nodal metastases are uncommon in early disease. Supraglottic carcinoma (epiglottis, aryepiglottic folds) does not cause hoarseness until the vocal cords are involved — presentation is therefore late. The supraglottis has rich lymphatic drainage — nodal metastases are common at presentation. Early = good prognosis; late + nodes = poor prognosis.
SELF-CHECK
A 45-year-old male tobacco chewer has a red, velvety patch on the floor of his mouth, 1.5 × 1 cm, present for 3 months. He is otherwise well. The most appropriate immediate action is:
A. Prescribe topical antifungal and review in 4 weeks
B. Urgent biopsy — erythroplakia has a very high rate of malignancy on histology
C. Reassure and advise tobacco cessation; review in 6 months
D. Refer to a dentist for dental extraction as the likely cause
Reveal Answer
Answer: B. Urgent biopsy — erythroplakia has a very high rate of malignancy on histology
A red velvety patch on the oral mucosa (erythroplakia) in a tobacco user that has been present for 3 months requires urgent biopsy. Erythroplakia has an approximately 50% chance of containing invasive SCC on histology — far higher than leukoplakia (~5%). The floor of the mouth is a particularly high-risk site. Antifungal treatment is inappropriate (this is not candidiasis — it is a keratotic/dysplastic lesion). Watchful waiting or dental referral wastes critical time in a potentially malignant lesion.