Page 34 of 44
EN2.11 | Topical Medication Instillation Technique — SDL Guide
Learning Objectives
- Demonstrate correct ear drop instillation technique including patient positioning and pinna traction
- Identify which ear drops are contraindicated with a tympanic membrane perforation and explain why
- Demonstrate correct nasal drop (including Moffett's position) and nasal spray instillation technique
- Counsel patients on self-administration of topical ENT medications
- Explain the rationale for topical vs systemic routes in ENT treatment
INSTRUCTIONS
Topical medication instillation is an EN2.11 skill-level competency: the technique must be demonstrated in a simulated setting. Incorrect ear drop instillation is extremely common — most patients hold the bottle incorrectly, do not pull the pinna, and sit upright immediately after instillation, wasting the medication. This module teaches the correct technique for each region, with emphasis on the most clinically important safety rule: never use aminoglycoside ear drops in an ear with a tympanic membrane perforation.
References
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery, 8th ed. Treatment sections (textbook)
- Hazarika P. Textbook of Ear, Nose and Throat & Head Neck Surgery, 3rd ed. Medical management chapter (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed. Topical therapy sections (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old female with CSOM comes to your clinic with worsening discharge. Her previous doctor had prescribed neomycin-containing ear drops, which she has been using for 3 weeks. On audiometry today, she has developed a new sensorineural hearing loss component that was not present 3 months ago. On otoscopy, she has a large central perforation. Her previous doctor did not check the TM before prescribing. What mistake was made — and what should have been prescribed instead?
WHY THIS MATTERS
EN2.11 is a Skill level competency because the technique for topical ENT medication instillation is specific, teachable, and demonstrable — and because incorrect technique leads to treatment failure (patient gets no benefit from correctly prescribed medication) or harm (ototoxic drops in a perforated ear cause iatrogenic SNHL). The OSCE will test your instillation technique on a model ear and ask you to counsel a standardised patient on how to use their nasal steroid spray. Both skills require practical demonstration, not just verbal description. This SDL provides the theoretical foundation and the step-by-step technique that will make your simulation session productive.
RECALL
Recall the anatomy of the external auditory canal: the outer third is cartilaginous, the inner two-thirds are bony; total length approximately 2.4 cm. The tympanic membrane separates the EAC from the middle ear. In a patient with an intact TM, ear drops remain in the EAC and cannot reach the middle ear. In a patient with a TM perforation, ear drops pass directly through the perforation into the middle ear and can contact the round window membrane — the entry point to the cochlea. Aminoglycosides (neomycin, gentamicin) are directly cochleotoxic when they contact the round window membrane, causing irreversible SNHL. Quinolone drops (ciprofloxacin) are safe for middle ear use and are preferred in CSOM. For the nose: the inferior turbinate is the main target of intranasal medications; the nasal steroid spray must be aimed at the lateral nasal wall (inferior turbinate), not the nasal septum — repeated spray onto the septum causes mucosal atrophy and may lead to septal perforation.
Clinical Indication: When Topical ENT Medications Are Used
Topical medications are preferred over systemic medications in ENT when the target tissue is directly accessible and when local application achieves higher drug concentrations at the site of action with lower systemic exposure. This pharmacological principle — targeted delivery with minimal systemic effect — is particularly important in ENT because many ENT drugs (aminoglycoside antibiotics, topical corticosteroids) have significant systemic toxicity when used parenterally but are effective and relatively safe when applied topically to accessible mucosal surfaces.
The main topical ENT medication categories are: (1) ear preparations — antibiotic ear drops (for otitis externa and CSOM), steroid-antibiotic combinations (for eczematous canal disease and post-surgical ear), antifungal drops (for otomycosis), and ceruminolytic/softening agents (for wax); (2) nasal preparations — topical corticosteroid sprays (first-line for allergic rhinitis and nasal polyps), decongestant drops and sprays (oxymetazoline, xylometazoline — for acute congestion, limited to 3–5 days to avoid rhinitis medicamentosa), saline nasal douches (chronic rhinosinusitis), and antibiotic nasal drops/ointments; (3) throat preparations — antiseptic gargles, topical anaesthetic sprays (lidocaine — for procedures), and lozenges.
The clinical indication for each preparation is determined by the diagnosis. For CSOM: the first-line topical treatment is aural toilet (careful cleaning of the canal and middle ear) followed by antibiotic ear drops — the choice depends on TM status (quinolone drops if perforated, aminoglycoside-steroid if intact TM). For allergic rhinitis: intranasal corticosteroid spray is the first-line pharmacological treatment (more effective than antihistamines for nasal symptoms, per evidence-based guidelines). For otomycosis: topical antifungal drops (clotrimazole, or diluted acetic acid) after thorough aural toilet.
Types of Topical ENT Medications and Their Principles
Understanding the pharmacological basis of each topical preparation prevents the most serious prescribing and instillation errors in ENT practice. The critical distinction in ear drop prescribing is the ototoxicity risk with TM perforation — and this distinction exists because the tympanic membrane is not merely a physical barrier to ear drops but a pharmacological one: when it is intact, topically applied drops remain in the external auditory canal and cannot reach the cochlea; when it is perforated, the middle ear becomes accessible and any ototoxic compound in the drops can contact the round window membrane and enter the cochlea directly. This single anatomical fact generates the entire ear drop safety classification below. For nasal and throat preparations, the main prescribing and technique errors are less about toxicity and more about incorrect positioning, incorrect direction of application, or incorrect duration of use — all of which lead to treatment failure or preventable complications such as rhinitis medicamentosa and nasal septal perforation.
Ear drops — safety classification:
Safe with TM perforation:
- Quinolone drops (ciprofloxacin 0.3%, ofloxacin) — safe because quinolones are not ototoxic in the concentrations used topically; ciprofloxacin ear drops are the first-line antibiotic ear drop for CSOM with perforation (per Dhingra).
- Normal saline and Burow's solution (aluminium acetate) — safe for ear irrigation and aural toilet.
- Ceruminolytics (olive oil, sodium bicarbonate drops, 5% sodium bicarbonate solution) — safe for wax softening before syringing.
Contraindicated with TM perforation (OTOTOXIC):
- Aminoglycoside-containing drops (neomycin-sulfate, gentamicin, tobramycin) — directly cochleotoxic when they contact the round window membrane through a perforation. These drops must NOT be prescribed for a patient with CSOM or a known TM perforation. They are safe only when the TM is intact (used in otitis externa with an intact TM).
- Spirit/alcohol-based drops — painful and cytotoxic in the middle ear.
Nasal preparations:
Intranasal corticosteroid sprays (beclomethasone, mometasone, fluticasone, budesonide): First-line treatment for allergic rhinitis. Require 1–2 weeks of regular use before measurable effect; full effect at 4–6 weeks. Must be aimed at the inferior turbinate (lateral nasal wall), not the septum. Systemic absorption is minimal at recommended doses.
Decongestant drops/sprays (oxymetazoline 0.1%, xylometazoline 0.1%): Alpha-adrenergic agonists that cause vasoconstriction of the inferior turbinate mucosa, reducing congestion within minutes. Limited to 3–5 days maximum — prolonged use causes rhinitis medicamentosa (rebound congestion and drug dependence).
Saline nasal douches (isotonic or hypertonic saline): Safe for all ages, no contraindications; used to irrigate the nasal cavity and sinuses, thin secretions, and enhance mucociliary clearance in chronic rhinosinusitis. Technique: head over a sink, insert the irrigation nozzle into one nostril, squeeze the bottle — saline flows through the nasal cavity and out the other nostril (or the mouth if the palate is closed).
SELF-CHECK
A 45-year-old male with CSOM and a known central TM perforation is prescribed antibiotic ear drops. Which drop is safe to use, and which must be avoided?
A. Ciprofloxacin 0.3% ear drops are safe; neomycin-containing drops must be avoided due to ototoxicity risk
B. Neomycin-containing drops are safe with a perforation; ciprofloxacin must be avoided
C. Both ciprofloxacin and neomycin are safe with a TM perforation
D. Both are equally ototoxic; neither should be used
Reveal Answer
Answer: A. Ciprofloxacin 0.3% ear drops are safe; neomycin-containing drops must be avoided due to ototoxicity risk
Ciprofloxacin (quinolone) ear drops are safe for use with a TM perforation because quinolones are not ototoxic at topical concentrations and are the first-line antibiotic ear drop for CSOM. Neomycin (aminoglycoside) ear drops are CONTRAINDICATED with a TM perforation — the drug passes through the perforation to the middle ear and contacts the round window membrane, causing irreversible cochleotoxicity and SNHL. This is a classic medicolegal ENT error and the most important safety point in ear drop prescribing.
Ear Drop and Nasal Medication Instillation Technique
Correct instillation technique is as important as the correct drug choice. Even when the correct medication is prescribed, incorrect instillation technique means the drug does not reach the target tissue — the drops pool in the outer canal or evaporate, while the patient reports 'I have been using the drops but they are not working.' Teaching the technique explicitly, with demonstration, is part of the clinical encounter for every ENT topical prescription.
Ear drop instillation technique (step by step):
Step 1 — Warm the drops. Cold ear drops cause sudden vestibular stimulation (caloric effect) — the patient experiences dizziness or nausea. Warm the bottle by holding it between the palms for 2–3 minutes, or by keeping it at room temperature.
Step 2 — Position. The patient lies on their side with the affected ear UPPERMOST. This ensures gravity carries the drops toward the TM and middle ear (if perforated) rather than allowing them to pool at the canal opening.
Step 3 — Pinna traction. Using the free hand, pull the pinna UPWARD and BACKWARD (as in otoscopy) to straighten the EAC and ensure the drops travel the full length of the canal.
Step 4 — Instil drops. Hold the drop nozzle just outside the canal opening (not inside — the tip should not touch the canal). Instil the prescribed number of drops (usually 3–5 drops). After instilling, gently press the tragus (the small cartilaginous projection anterior to the canal opening) inward and outward several times — this tragal pumping action helps propel the drops down the canal and through the perforation into the middle ear if present.
Step 5 — Maintain position. The patient should remain lying with the treated ear UP for at least 5–10 minutes to allow the drops to flow to the tympanic membrane. Then sit up and allow excess drops to drain. A cotton ball may be placed loosely at the canal entrance — but a tightly packed cotton ball blocks drainage and should not be used.
Nasal drop instillation technique:
Standard position (head-down): For drops to reach the middle meatus and paranasal sinuses, the head must be positioned with the nose lower than the pharynx — the patient kneels over the edge of a bed and lowers the head toward the floor (Moffett's position), or lies supine with the head hanging over the side of the bed. In Moffett's position, the nose points toward the floor and gravity carries the drops to the middle meatus.
Nasal spray technique:
Step 1 — Blow nose first. Clear nasal secretions before applying the spray so the medication contacts the mucosa, not the mucus layer.
Step 2 — Position. Head slightly forward, NOT hyperextended (which directs the spray into the nasopharynx, not the inferior turbinate).
Step 3 — Correct hand — cross-technique. Use the RIGHT hand for the LEFT nostril and the LEFT hand for the RIGHT nostril. This naturally angles the spray nozzle toward the lateral nasal wall (inferior turbinate) rather than toward the nasal septum.
Step 4 — Angle the nozzle. Point the nozzle toward the OUTER CORNER of the SAME EYE (not toward the midline septum). This directs the spray toward the inferior turbinate.
Step 5 — Press and breathe. Press the pump while sniffing gently. Do not sniff forcefully (drug reaches the pharynx, not the turbinate). Breathe out through the mouth.
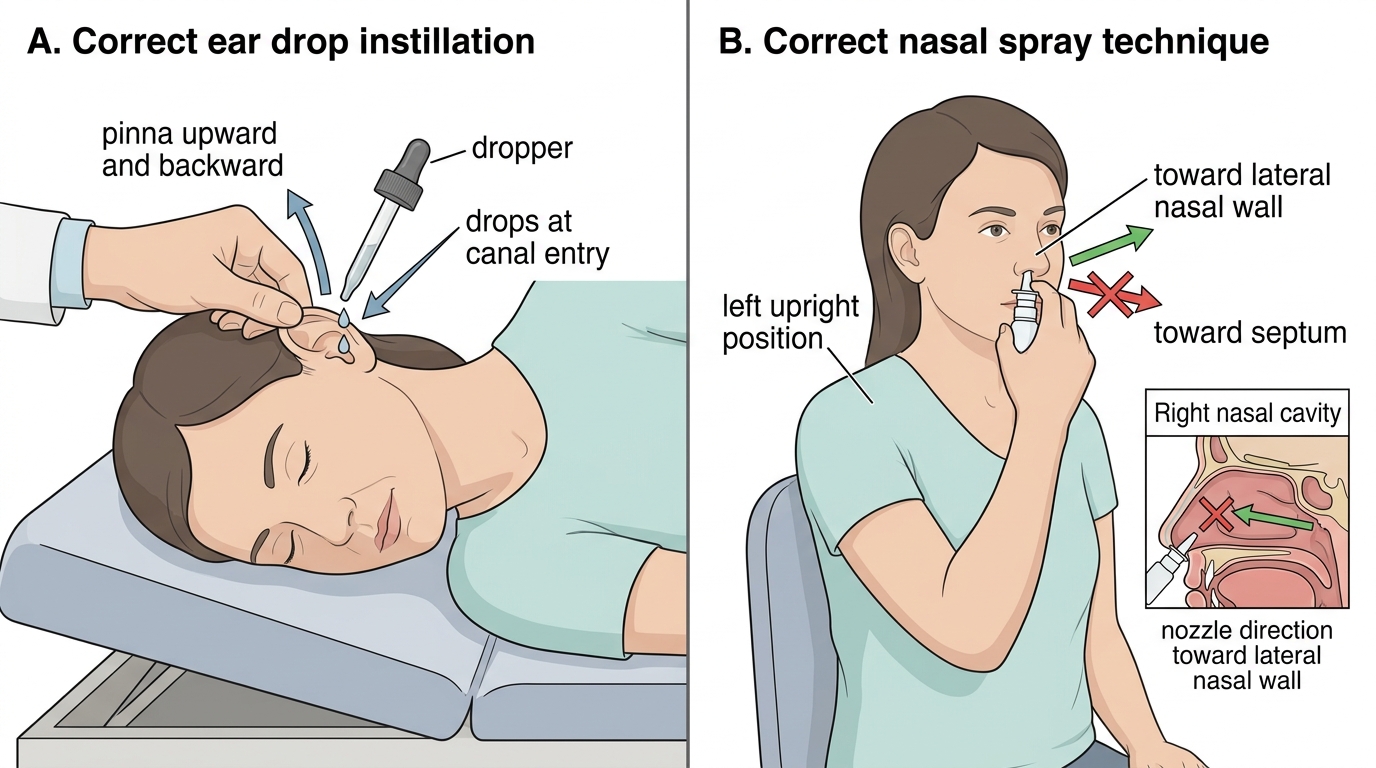
Correct Technique for Ear Drops and Nasal Spray