Page 4 of 17
EN4.2 | External Ear Diseases — SDL Guide
Learning Objectives
- Elicit and document a structured history from a patient presenting with diseases of the external ear
- Describe the clinical features distinguishing the major conditions affecting the pinna and external auditory canal
- Choose appropriate investigations for diseases of the external ear, including culture, imaging, and microscopy
- Describe the principles of management of the common and important conditions of the pinna and external auditory canal
INSTRUCTIONS
The external ear — comprising the pinna and the external auditory canal — is affected by a wide range of conditions, from trivially common (wax impaction, swimmer's ear) to potentially life-threatening (malignant otitis externa). The external ear is also the most accessible part of the ear for clinical examination, making a systematic approach to its diseases an essential clinical skill. This module covers the full spectrum from inflammatory and infectious to structural and neoplastic conditions, with special emphasis on conditions where delayed diagnosis causes irreversible harm.
References
- Dhingra PL, Dhingra S — Diseases of Ear, Nose and Throat, 8th ed., Ch. 6: Diseases of the External Ear (textbook)
- Hazarika P — Textbook of Ear, Nose and Throat and Head-Neck Surgery, 3rd ed., Ch. 6: Diseases of the External Ear (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed., Vol 3, Ch. 238: Diseases of the External Ear (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 68-year-old man with poorly controlled type 2 diabetes presents to the emergency department with severe left ear pain that has progressively worsened over three weeks. He has been taking over-the-counter ear drops without relief. On examination, the pinna is tender, and there is oedema of the EAC with granulation tissue visible at the floor of the canal at the bony-cartilaginous junction. His left ear canal discharge grows Pseudomonas aeruginosa on culture. He is started on topical antibiotics alone and sent home. Two weeks later he returns with a left lower motor neurone facial palsy. A CT scan of the temporal bones shows skull base erosion. He is admitted to hospital for six weeks of intravenous antibiotics. Could the facial palsy have been prevented?
WHY THIS MATTERS
Diseases of the external ear are among the most common clinical presentations in ENT outpatient practice and in primary care. Acute diffuse otitis externa alone accounts for an estimated 1 in 10 ENT consultations, and wax impaction is the single most frequent reason for an adult to consult a GP about their ears. Most external ear conditions are managed at primary care and cause significant but self-limiting morbidity. However, malignant otitis externa — predominantly a disease of elderly diabetics and immunocompromised patients — can progress to skull base osteomyelitis, cranial nerve palsies, and death, with mortality in unrecognised cases historically exceeding 50% (Scott-Brown's). The NMC EN4.2 competency requires you to take a structured history, demonstrate and describe clinical features, choose investigations, and describe management principles for the full spectrum of external ear disease — from the benign to the life-threatening.
RECALL
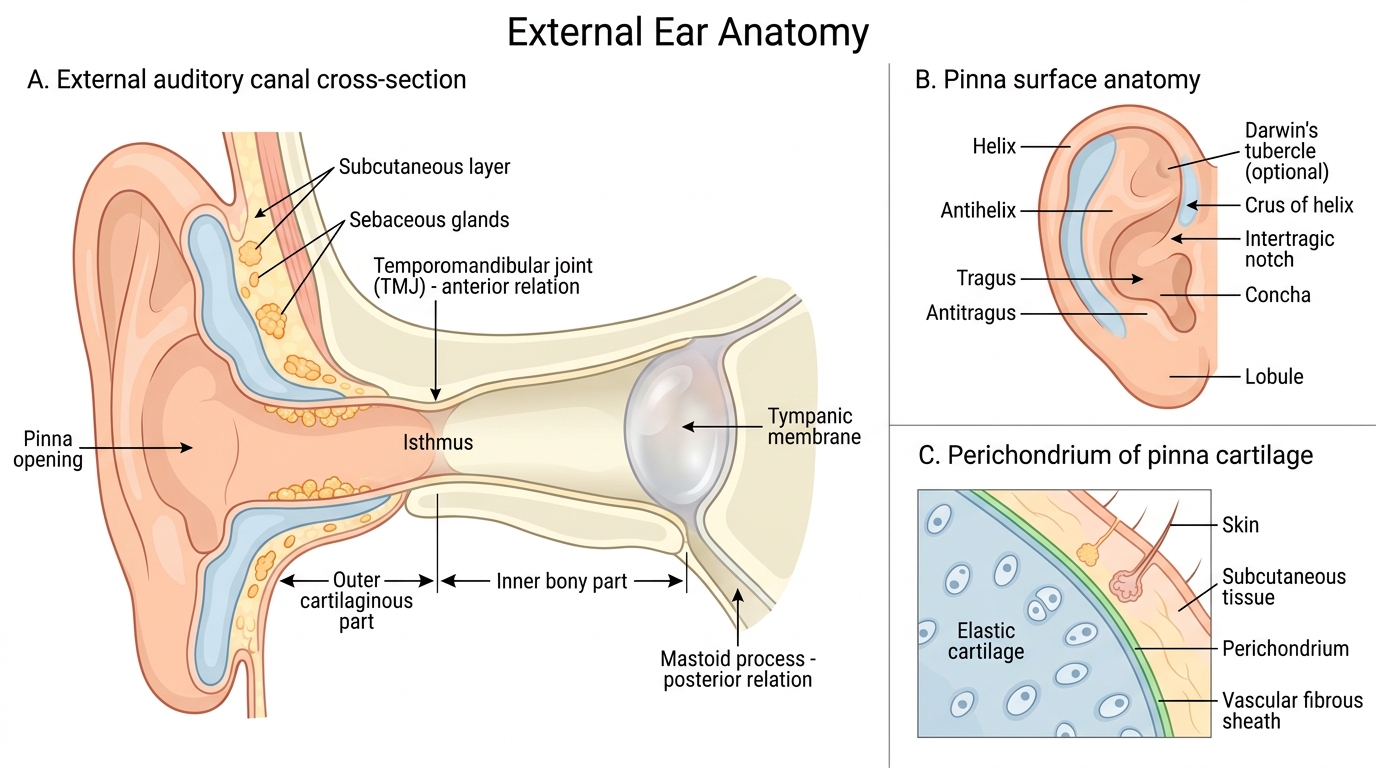
Recall from your anatomy sessions the two-part structure of the external auditory canal (EAC): the outer one-third is cartilaginous, lined with skin containing ceruminous glands (modified apocrine glands producing cerumen/wax), sebaceous glands, and hair follicles; the inner two-thirds is bony (tympanic bone), lined by thin, tightly adherent skin with no glands and no subcutaneous fat. The bony-cartilaginous junction — also called the isthmus — is the narrowest part of the EAC and a common site for wax impaction and where granulation tissue forms in malignant OE. The pinna is composed of a framework of elastic cartilage covered by skin adherent to the perichondrium on both surfaces. Because the perichondrium is the sole blood supply to the avascular cartilage, any condition that strips perichondrium from cartilage (haematoma, infection) deprives the cartilage of its nutrient supply and leads to cartilage necrosis and deformity.
Clinical Presentation of External Ear Diseases
The symptoms of external ear disease are closely determined by the anatomical region affected — pinna versus EAC — and by the nature of the underlying pathology. Taking a structured history that separates these regions and identifies the symptom character is the foundation of a focused clinical assessment.
Symptoms arising from the pinna:
The pinna presents with pain, swelling, deformity, and skin change, whose combination points to the underlying pathology. Perichondritis — infection of the pinna's perichondrium, most commonly caused by Pseudomonas aeruginosa — presents as diffuse redness, warmth, and severe tenderness of the pinna, sparing the lobule (which has no cartilage and therefore no perichondrium). The lobule-sparing pattern is a key clinical clue distinguishing perichondritis from cellulitis, which involves the lobule. Ask about recent trauma, ear piercing through cartilage (a well-recognised precipitant), burns, or ear surgery — any breach of the perichondrium is a risk factor for Pseudomonas seeding. Haematoma auris (cauliflower ear precursor) follows blunt trauma — a blow to the ear, head restraint in wrestling/rugby — and presents as a smooth, tense, fluctuant, non-tender swelling over the helical rim within hours of injury. Early drainage is the pivotal management decision. Keloid formation on the pinna (especially the lobule after ear piercing) presents as a raised, firm, non-tender scar overgrowth extending beyond the original wound margin.
Symptoms arising from the external auditory canal:
The EAC presents with a distinctive cluster: otalgia (pain), otorrhoea (discharge), pruritus (itching), and conductive hearing loss. The character and combination of these symptoms has strong diagnostic value. Understanding which symptom predominates guides the examination focus.
- Otalgia + severe tenderness on tragal pressure + pain on pinna traction = acute diffuse otitis externa (swimmer's ear). Pain is out of proportion to the otoscopic appearance.
- Pruritus >> pain + thick white or black debris = otomycosis (fungal OE). Itching rather than pain predominates; discharge has a characteristic appearance.
- Severe intractable pain in a diabetic + granulation tissue at EAC floor = malignant (necrotising) OE — a must-not-miss.
- Gradual conductive hearing loss + wax plug = wax impaction — the most common cause of adult hearing loss in primary care.
- EAC fullness + no pain + hard smooth bony enlargement bilaterally in a cold-water swimmer = exostoses — bilateral bony EAC narrowing from cold-water exposure.
Key history points to elicit: water exposure or swimming (otitis externa, otomycosis); ear instrumentation or cotton bud use (trauma, introducing infection); diabetes mellitus (malignant OE risk); trauma to pinna; ear piercing history; occupation (cold-water divers); immunosuppression (fungal infections, malignant OE).
Anatomy of the External Ear
The anatomy of the external ear is the key to understanding why specific diseases arise where they do, why certain organisms dominate, and why some conditions lead to severe complications while others are self-limiting.
The pinna:
The pinna (auricle) is a three-dimensional structure of elastic cartilage moulded into the helix, antihelix, tragus, antitragus, and concha, covered bilaterally by skin tightly adherent to the perichondrium. The lobule — the inferior soft part of the ear — contains fat and connective tissue but no cartilage, and therefore no perichondrium. This anatomical fact is clinically critical: conditions involving the perichondrium (perichondritis) do not affect the lobule, because the lobule has no cartilage to protect. The perichondrium is the sole vascular supply to the avascular cartilage. If perichondrium is stripped from cartilage — by haematoma, by infection, or by surgical trauma — the cartilage loses its blood supply and undergoes avascular necrosis, resulting in permanent deformity (the cauliflower ear of untreated haematoma auris, or the helix collapse of perichondritis).
The external auditory canal:
The EAC extends from the concha of the auricle to the tympanic membrane — approximately 2.5 cm long, slightly S-shaped when viewed from the side. The outer one-third is cartilaginous: the skin here is thick, contains sebaceous glands, hair follicles, and ceruminous glands (modified apocrine glands), and is mobile. The inner two-thirds is bony (formed by the tympanic bone): the skin is thin, avascular, tightly adherent to the periosteum, and contains no glands. The isthmus — the bony-cartilaginous junction — is the narrowest point of the canal and the most common site for impaction of wax and foreign bodies.
Cerumen (wax) is produced by the ceruminous glands and mixed with sebum. It serves a protective function — antibacterial, antifungal, and waterproofing — and normally migrates laterally by the epithelial migratory pattern of the EAC. Disruption of this migration (aggressive cotton bud use, hearing aid use, or abnormal migration in some patients) leads to wax accumulation and impaction.
The absence of subcutaneous fat in the bony EAC skin means that even mild inflammation rapidly causes severe pain — there is no cushion for oedematous pressure. This explains why acute diffuse OE of the bony EAC is exquisitely painful. In malignant OE, Pseudomonas infection tracks along the bony-cartilaginous junction through Santorini's fissures (small fissures in the cartilaginous floor of the EAC) directly into the skull base — explaining the rapid spread to the temporal bone, cranial nerve foramina, and beyond.
External Auditory Canal and Pinna Anatomy
SELF-CHECK
A 25-year-old competitive swimmer presents with a 4-day history of severe right ear pain, worsened by pulling the pinna, and a thin watery discharge. He has no fever. Otoscopy shows oedema and erythema of the EAC skin; the tympanic membrane is barely visible but appears intact. The most likely diagnosis and primary management is:
A. Acute otitis media: oral amoxicillin 500 mg thrice daily for 5 days
B. Acute diffuse otitis externa: aural toilet followed by topical antibiotic-steroid drops
C. Otomycosis: topical clotrimazole solution to the EAC after aural toilet
D. Bullous myringitis: topical ciprofloxacin drops and analgesics
Reveal Answer
Answer: B. Acute diffuse otitis externa: aural toilet followed by topical antibiotic-steroid drops
This is acute diffuse otitis externa (swimmer's ear): swimming water exposure + severe otalgia + pain on tragal pressure/pinna traction + EAC skin erythema and oedema with intact TM. Primary management is aural toilet (suctioning or dry mopping the canal) to remove debris and discharge, followed by topical antibiotic-steroid drops (ciprofloxacin-hydrocortisone or gentamicin-betamethasone). AOM presents with a bulging, opaque TM and fever; this TM appears intact. Otomycosis is characterised by pruritus and fungal debris (black/white spores), not predominant pain with thin discharge. Bullous myringitis presents with haemorrhagic vesicles on the TM itself.
ENT Examination and Investigation of the External Ear
The examination of the external ear follows a logical anatomical sequence from outside inward, and should never be limited to otoscopy alone. Many conditions affecting the pinna are diagnosed entirely on inspection; the EAC and TM require otoscopic assessment; and clinical suspicion for malignant OE or deep-seated infection must prompt imaging.
Examination sequence:
Step 1 — Inspect the pinna:
Look at both pinnae. Note any deformity (cauliflower ear from old haematoma, helix notching from perichondritis scarring), skin changes (erythema, vesicles in herpes zoster, squamous cell or basal cell carcinoma — ulcerated lesion on sun-exposed helix), swelling (haematoma — fluctuant, smooth, overlying helix; perichondritis — diffuse erythema, warmth, tender, sparing the lobule), and colour (cyanotic discoloration in severe perichondritis preceding cartilage necrosis).
Step 2 — Palpate pre-auricular and post-auricular regions:
Pre-auricular tenderness + swelling of the parotid region suggests parotitis. Post-auricular tenderness with forward displacement of the pinna indicates mastoiditis. Palpate the pinna itself — tenderness on palpation of the cartilage (excluding lobule) points to perichondritis.
Step 3 — Test tragal tenderness and pinna traction:
Gentle pressure on the tragus (tragal sign) or traction on the pinna that reproduces or worsens pain indicates EAC skin inflammation — a positive finding in acute OE. This test is negative in AOM (pain arises from middle ear, not EAC skin).
Step 4 — Otoscopic examination:
Insert the smallest appropriate speculum. In OE, canal oedema may make insertion difficult and painful — use the smallest speculum gently. Inspect systematically: EAC skin (erythema, oedema, debris colour and consistency — ceruminous wax is brown, fungal debris is black or white with characteristic hyphae, purulent discharge is yellow-green), condition of the TM (may be partly obscured by debris — do not force). In malignant OE, look specifically for granulation tissue at the floor of the EAC at the bony-cartilaginous junction — this is the pathognomonic finding.
Step 5 — Facial nerve testing:
In any suspected malignant OE or severe EAC infection, test facial nerve function (forehead wrinkling, eye closure, smile, nasolabial fold symmetry). New facial palsy in the context of OE = skull base involvement until proven otherwise.
Investigations:
- EAC swab for culture and sensitivity: essential in OE not responding to initial topical therapy, in suspected malignant OE, and in otomycosis (fungal culture, KOH wet preparation). The KOH mount is diagnostic in otomycosis — it shows Aspergillus hyphae with conidia heads (Aspergillus niger gives black spores) or Candida pseudohyphae.
- CT scan of the temporal bones: in suspected malignant OE (skull base involvement), keratosis obturans (bony expansion of EAC), or EAC tumour. High-resolution CT shows bone erosion, soft tissue extension, and involvement of the facial nerve canal.
- Technetium-99m bone scan / Gallium-67 scan: sensitive for malignant OE disease activity and monitoring treatment response (bone scan remains positive for months after infection is controlled; gallium correlates better with active disease).
- Blood glucose / HbA1c: in all cases of malignant OE — uncontrolled diabetes is the principal risk factor.
- ESR and CRP: elevated in malignant OE; useful for monitoring treatment response.
- Biopsy: if pinna lesion is suspicious for malignancy (ulcerated, indurated, rolled edges on the helix) — basal cell carcinoma most common on helix; squamous cell carcinoma also occurs.