Page 2 of 17
EN4.1 | Otalgia — SDL Guide (Part 2)
Diagnosis and Differential Diagnosis of Otalgia
The diagnostic framework for otalgia proceeds from the history and examination findings to a structured, anatomically-organised differential diagnosis. The overarching organising question is: does the examination reveal primary ear pathology that can account for the pain? If it does, the differential is confined to the ear and its immediate structures — the external canal, the middle ear, and the mastoid. If the ear examination is normal — a finding that, in adults especially, is at least as common as finding an abnormality — the clinician must shift focus entirely to the referred pathway structures: the oral cavity, the oropharynx, the hypopharynx and larynx, the TMJ, the salivary glands, and the cervical spine. Failing to make this conceptual shift is the proximate cause of missed head-and-neck malignancies presenting as otalgia. The causes within each category are arranged below in rough order of clinical importance.
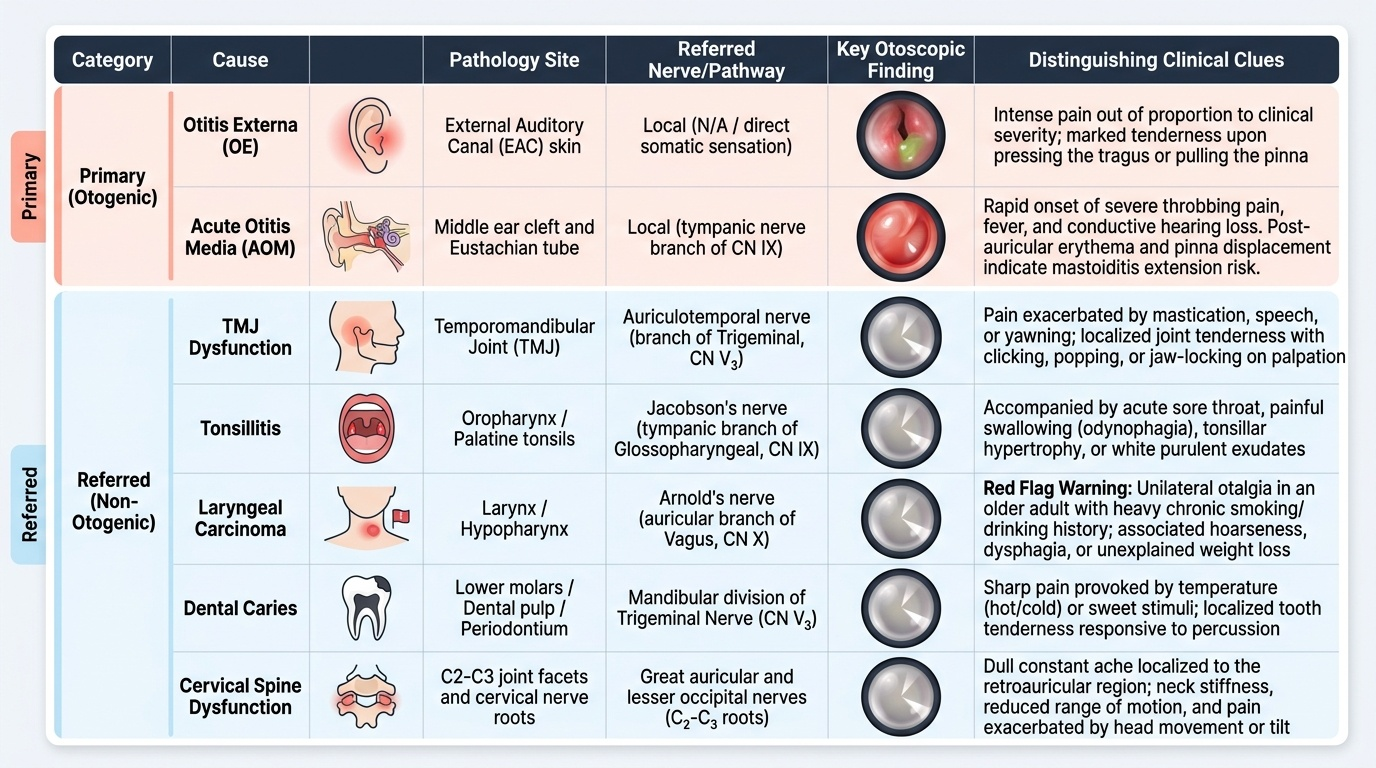
Provided image
Primary (otogenic) otalgia — causes to consider:
- Otitis externa (OE): erythema and oedema of the EAC skin, tenderness on tragal pressure and pinna movement, discharge. The pain can be severe and disproportionate to appearance. Malignant OE (skull base osteomyelitis, typically in elderly diabetics caused by Pseudomonas aeruginosa) presents with severe pain, granulation tissue at the EAC floor, cranial nerve palsies — a life-threatening condition.
- Acute otitis media (AOM): fever, ear pain, conductive hearing loss, dull or bulging TM with absent cone of light. Children commonly. AOM progressing to mastoiditis causes post-auricular swelling and tenderness, pinna displaced forwards and downwards.
- Chronic suppurative otitis media (CSOM) with exacerbation: central TM perforation with mucopurulent discharge; pain during exacerbation. The unsafe (atticoantral) type with cholesteatoma can present with foul discharge, bone erosion, and pain. Pain in CSOM can also herald a complication (lateral sinus thrombosis, extradural abscess, meningitis).
- Herpes zoster oticus (Ramsay Hunt syndrome): severe burning otalgia + vesicles in EAC/concha + facial palsy ± sensorineural hearing loss. The vesicles may be sparse and easily missed.
- Bullous myringitis: painful haemorrhagic blisters on the TM, associated with viral or Mycoplasma infection — severe acute pain.
- Myringitis (TM inflammation without perforation): erythematous, injected TM.
- Furunculosis (boil of the outer EAC): localised painful swelling in the cartilaginous EAC — very tender, may point and discharge.
Referred (non-otogenic) otalgia — causes to consider:
- Dental (CN V): lower molar caries, dental abscess, impacted wisdom teeth — pain reproduced by biting, hot/cold foods.
- TMJ dysfunction / Costen's syndrome (CN V): pre-auricular pain, jaw clicking, worsened by chewing; TMJ tender to palpation.
- Tonsillitis / peritonsillar abscess (CN IX): acute tonsillitis, peritonsillar abscess (trismus + uvular deviation + muffled voice) — referred ear pain via Jacobson's nerve.
- Post-tonsillectomy otalgia (CN IX): common in the first 7–10 post-operative days; managed with analgesics.
- Oropharyngeal carcinoma (CN IX): unilateral otalgia + throat discomfort + neck node — biopsy and staging required.
- Hypopharyngeal or laryngeal carcinoma (CN X, Arnold's nerve): the most important single diagnosis to exclude in an adult with unexplained unilateral otalgia — especially in smokers and drinkers. The primary lesion may cause minimal local symptoms until advanced; otalgia may be the first symptom.
- Pharyngitis / nasopharyngitis: common, bilateral, usually obvious from throat examination.
- Eagle's syndrome: elongated styloid process causing otalgia and throat discomfort on swallowing — diagnosed by palpation of tonsillar fossa or CT.
- Cervical spondylosis / disc prolapse C2–C3 (great auricular nerve): otalgia with neck pain, stiffness, and neurological symptoms in the arm — cervical spine imaging required.
- Parotid pathology: parotitis, Warthin's tumour, parotid carcinoma — parotid swelling + otalgia.
SELF-CHECK
A 45-year-old woman presents with severe left ear pain for 5 days. She has pain on opening her mouth. There are vesicular lesions in the left EAC and concha. She also has a left-sided lower motor neurone facial palsy. The diagnosis and the responsible virus is:
A. Otitis externa caused by Pseudomonas aeruginosa
B. Ramsay Hunt syndrome caused by varicella-zoster virus reactivation
C. Acute otitis media caused by Streptococcus pneumoniae
D. Bullous myringitis caused by Mycoplasma pneumoniae
Reveal Answer
Answer: B. Ramsay Hunt syndrome caused by varicella-zoster virus reactivation
This is Ramsay Hunt syndrome (herpes zoster oticus): the triad of severe otalgia + vesicles in the EAC/concha + ipsilateral peripheral facial nerve palsy is pathognomonic. The causative agent is reactivation of varicella-zoster virus (VZV) in the geniculate ganglion of the facial nerve (CN VII). Otitis externa (Pseudomonas) causes diffuse EAC tenderness without vesicles or facial palsy. AOM causes a bulging TM with fever; no vesicles. Bullous myringitis causes haemorrhagic blisters on the TM itself, not vesicles in the EAC skin, and does not cause facial palsy.
Principles of Management
The management of otalgia is entirely and non-negotiably driven by its underlying cause. There is no generic treatment for ear pain in the way that there is a generic treatment for a sore throat — the word "otalgia" names a symptom, not a disease, and treating the symptom with topical ear drops when the source is a tonsillar carcinoma or a laryngeal tumour is not merely ineffective; it provides false reassurance that actively delays a curative-intent diagnosis. The clinical principle, therefore, has three components: identify the cause first, treat the cause specifically, and provide appropriate analgesia as an adjunct rather than as a substitute for diagnosis. The following sections outline cause-directed management for the principal otogenic and referred categories, followed by the general analgesic approach and indications for urgent referral.
Management of primary (otogenic) causes:
- Otitis externa: meticulous aural toilet (suctioning the canal under microscope or dry mopping) followed by topical antibiotic/steroid drops (ciprofloxacin 0.3% + hydrocortisone, or gentamicin + betamethasone). Analgesics. If canal is very oedematous and drops cannot penetrate, an ear wick (glycerine and ichthammol-soaked ribbon gauze or manufactured wick) is inserted to allow the drops to reach the deeper canal. Systemic antibiotics only if cellulitis extends outside the EAC or if the patient is diabetic/immunocompromised. Malignant otitis externa: hospital admission, intravenous anti-pseudomonal antibiotics (piperacillin-tazobactam or cefepime ± tobramycin) for 4–6 weeks + aggressive glycaemic control in diabetics. Surgery (debridement) for necrotic bone.
- Acute otitis media: analgesia (paracetamol ± ibuprofen) is the first-line treatment. Antibiotics (amoxicillin 40–45 mg/kg/day for 5–7 days) are indicated in children <2 years, severe disease, or if no improvement in 48–72 hours. Decongestants are not effective. Myringotomy is indicated for severe pain or incipient complication — performed in the antero-inferior quadrant of the tympanic membrane (to avoid ossicles superiorly and jugular bulb inferiorly).
- Ramsay Hunt syndrome: early antiviral therapy (aciclovir 800 mg five times daily or valaciclovir 1 g thrice daily) started within 72 hours + oral prednisolone — reduces the severity of facial palsy and duration of otalgia. Eye protection (lubricant drops, eye pad at night) if corneal exposure from facial palsy.
- Furunculosis: analgesics + oral flucloxacillin; incision and drainage when pointing.
Management of referred otalgia:
- Dental causes: refer to dentist for appropriate dental treatment (extraction, root canal, drainage of abscess).
- TMJ dysfunction: soft diet, avoid chewing hard foods, NSAIDs, physiotherapy, dental occlusal splint. Refractory cases: intra-articular steroid injection or surgical intervention by maxillofacial team.
- Tonsillitis: analgesics, adequate hydration, antibiotics for bacterial tonsillitis (phenoxymethylpenicillin or amoxicillin — avoid ampicillin/amoxicillin if infective mononucleosis is possible due to risk of maculopapular rash). Peritonsillar abscess: needle aspiration or incision and drainage under local anaesthesia + antibiotics. Interval tonsillectomy after recurrent episodes.
- Post-tonsillectomy otalgia: reassurance + regular analgesia (paracetamol ± diclofenac). Expected to resolve as the tonsillar fossa heals by secondary intention.
- Oropharyngeal/hypopharyngeal/laryngeal malignancy: urgent referral to oncological ENT team. Management is by multimodal treatment (surgery, radiotherapy, chemotherapy depending on staging). Early referral is critical — the poor hook case illustrates what happens when this is delayed.
- Cervical spondylosis: physiotherapy, NSAIDs, cervical collar; neurosurgical referral if neurological deficit is present.
General principle — analgesic ladder:
Paracetamol and NSAIDs are appropriate as adjuncts at all stages of otalgia management. Opioids may be required briefly for severe pain (e.g., Ramsay Hunt, malignant OE). Analgesics should not replace or delay definitive treatment.
Indications for urgent referral:
- Unexplained otalgia with normal ear examination in any adult — urgent H&N examination is mandatory.
- Suspected skull base involvement (malignant OE, cholesteatoma complication).
- Suspected or confirmed head-and-neck malignancy.
- Peripheral facial palsy (Ramsay Hunt or other aetiology).
- Suspected AOM complication (mastoiditis, intracranial involvement).
SELF-CHECK
During myringotomy for acute otitis media in a child, the correct safe site for the incision is:
A. Postero-superior quadrant
B. Antero-inferior quadrant
C. Postero-inferior quadrant
D. Pars flaccida (Shrapnell's membrane)
Reveal Answer
Answer: B. Antero-inferior quadrant
The safe site for myringotomy is the antero-inferior quadrant of the pars tensa. The postero-superior quadrant overlies the ossicular chain (incudostapedial joint), risking ossicular damage. The postero-inferior quadrant risks injury to a high-riding jugular bulb (a normal variant). The pars flaccida is in the attic and is the site of attic retraction pockets and cholesteatoma — incisions there are contraindicated. The antero-inferior quadrant is away from these vulnerable structures and is the standard taught site.
CLINICAL PEARL
The most dangerous error in otalgia management is dismissing normal-otoscopy ear pain in an adult as psychosomatic or functional. Referred otalgia from an occult head-and-neck malignancy — most commonly hypopharyngeal or laryngeal carcinoma — can be the only presenting symptom for months before the tumour becomes clinically obvious. The rule is simple: any adult with unilateral otalgia and a normal ear examination must have a complete head-and-neck examination including indirect or fibreoptic laryngoscopy before the cause is attributed to a benign referred source. A missed carcinoma at this stage is a missed window for curative intent treatment.
Self-Assessment
Before moving on, take a few minutes to test your own recall and application of the key principles from this module. Self-assessment at this stage is not simply a revision exercise — it surfaces the gaps between what you believe you know and what you can actually recall under examination conditions. Research on retrieval practice (testing effect) consistently shows that attempting to answer questions without reference to notes consolidates learning more effectively than re-reading the material. If a question exposes a gap, return to the relevant section with that specific question as your reading target. The questions below cover all six arc steps and include the highest-stakes clinical facts — the ones that, if forgotten, could lead to a patient harm scenario in your practice.
- Name the five nerve pathways that can mediate referred otalgia, and give one clinical example of a cause for each pathway.
- What is the single most important examination step in an adult presenting with unilateral otalgia and a normal otoscopic examination? Why?
- A patient develops severe ear pain, vesicles in the EAC, and facial weakness on the same side. Name the syndrome, the causative agent, and the treatment.
- In which quadrant of the tympanic membrane should myringotomy be performed, and why are the other quadrants avoided?
- What features in the history of otalgia should raise immediate concern for head-and-neck malignancy?
If you are unable to identify the five referred pathways (CN V, VII, IX, X, C2–C3) and their associated causes, revise the neuroanatomy section before your examination. The malignancy question is the highest-stakes factual point in this module — an ENT doctor who does not act on an adult's unexplained unilateral otalgia has made a potentially irreversible clinical error.