Page 8 of 29
EN4.14 | Conductive and Sensorineural Hearing Loss — SDL Guide (Part 2)
Diagnosis: CHL vs SNHL and Key Causes
The audiogram is the definitive tool for classifying hearing loss, and the ability to read an audiogram is an essential competency for every doctor — not just ENT specialists. Audiograms appear in examination stations, ward rounds, and referral letters. The key skill is pattern recognition: identifying an air-bone gap (CHL), the absence of a gap with elevated thresholds (SNHL), or the 4 kHz notch signature. Once the type is established — CHL, SNHL, or mixed — the history, otoscopy, and additional investigations narrow down the cause. Two specific SNHL entities require detailed knowledge because of their clinical importance and examination yield: sudden sensorineural hearing loss and noise-induced hearing loss. Both have characteristic audiometric signatures that must be recognised on sight.
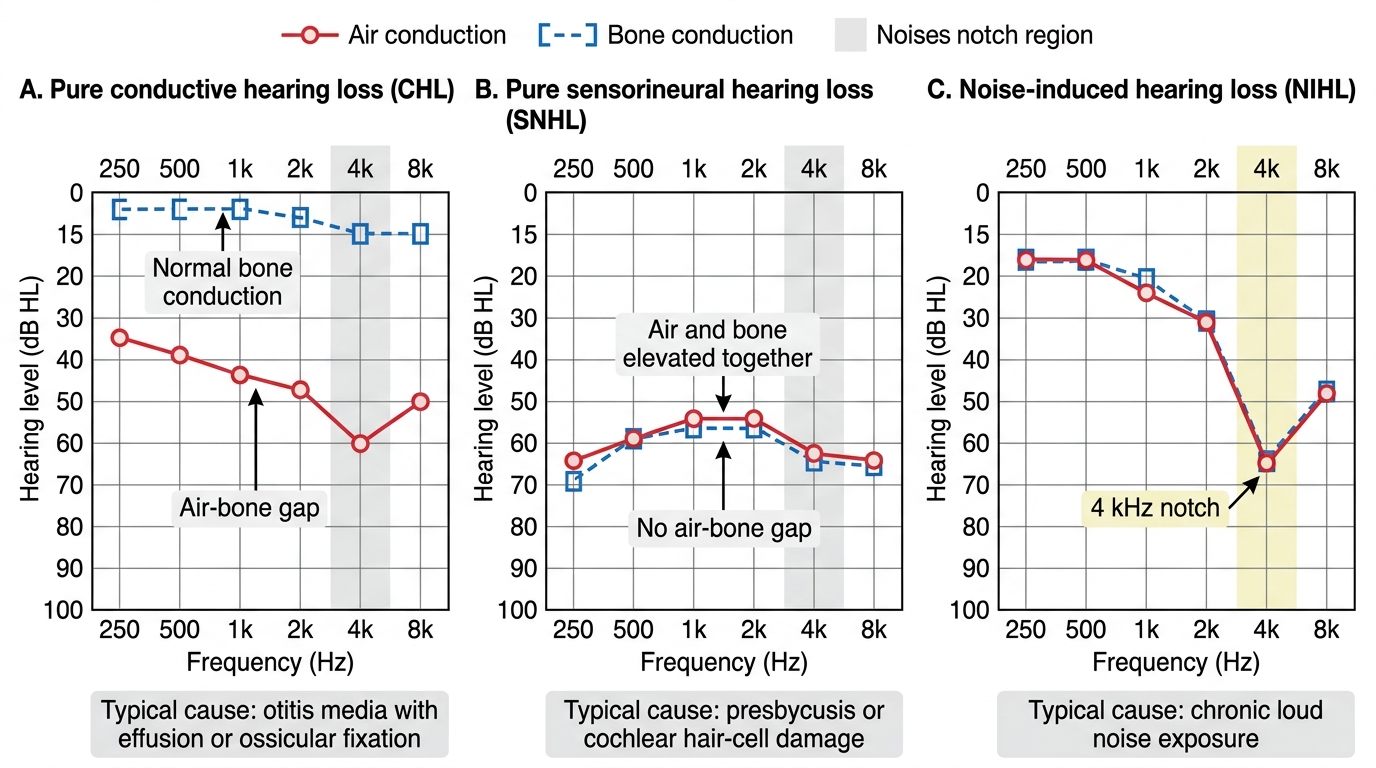
Audiogram Patterns in CHL, SNHL, and NIHL
Sudden Sensorineural Hearing Loss (SSNHL)
Definition: ≥30 dB of sensorineural hearing loss at ≥3 contiguous audiometric frequencies, developing within 72 hours. This is an otological emergency.
Aetiology: Idiopathic in the majority (~85%) — presumably viral cochleitis, vascular ischaemia of the cochlear artery, or membranous labyrinth rupture. Known causes to exclude:
- Acoustic neuroma (found on MRI in 6–15% of SSNHL cases — MRI is mandatory)
- Meniere's disease (if associated with vertigo and aural fullness)
- Autoimmune inner ear disease
- Vascular causes (vertebrobasilar insufficiency)
- Perilymph fistula (follows Valsalva, straining, head trauma)
Natural history: approximately 60% recover spontaneously within 2 weeks without any treatment. Prognostic factors for poor recovery: profound loss at onset, low-frequency loss pattern (vs high-frequency), older age, delay in treatment, presence of vertigo.
Management of SSNHL:
1. Same-day ENT assessment — do not send the patient home without investigation
2. MRI with gadolinium — to exclude acoustic neuroma
3. High-dose oral corticosteroids (prednisolone 1 mg/kg/day up to 60 mg, tapering over 10–14 days) — first-line; improves recovery rate compared to no treatment
4. Intratympanic steroid injection — as salvage treatment for non-responders to systemic steroids, or as primary treatment when systemic steroids are contraindicated (e.g. diabetic patients)
5. Hyperbaric oxygen — adjunctive therapy in some centres, limited evidence
Noise-Induced Hearing Loss (NIHL)
Definition: Permanent SNHL caused by excessive sound energy damaging cochlear outer hair cells, characteristically producing a bilateral symmetric 4 kHz notch on audiometry.
Pathophysiology: Sound above ~85 dB SPL (over 8-hour time-weighted average) generates metabolic stress — reactive oxygen species, glutamate excitotoxicity, and cochlear vasoconstriction — in the basal outer hair cells. The 4 kHz region is most vulnerable because of acoustic resonance and its end-arterial blood supply. Initially, the damage manifests as a temporary threshold shift (TTS) that recovers overnight. Repeated TTS causes cumulative permanent threshold shift (PTS).
Clinical features:
- Bilateral, symmetric SNHL
- 4 kHz notch on audiometry (C5 dip) with recovery toward normal at 8 kHz
- Tinnitus (often high-pitched, bilateral) — commonly precedes measurable hearing loss
- Poor speech discrimination in background noise
- No history of ear disease
Prevention of NIHL (most important management principle):
- Hearing conservation programmes in workplaces with noise ≥85 dB TWA
- Engineering controls (enclosures, vibration dampening)
- Personal hearing protection (earplugs, earmuffs) — mandatory in high-noise zones
- Annual audiometric surveillance for workers exposed to industrial noise
- Regulations: occupational noise ≥85 dB TWA (Occupational Safety and Health Act threshold)
Treatment of established NIHL: No proven medical treatment reverses established NIHL. Hearing aids for the functional disability. Prevention is the only definitive intervention.
SELF-CHECK
A 45-year-old man presents as an emergency with sudden onset of complete deafness in his right ear, noticed on waking. He has no history of ear disease. Otoscopy is normal. The single most important investigation to arrange within the same day is:
A. Pure-tone audiometry to grade the severity of loss
B. MRI brain with gadolinium (IAC sequences) to exclude acoustic neuroma
C. High-dose prednisolone — start treatment empirically without imaging
D. Electrocochleography to assess endolymphatic hydrops
Reveal Answer
Answer: B. MRI brain with gadolinium (IAC sequences) to exclude acoustic neuroma
SSNHL is an otological emergency. While PTA is needed to document and grade the loss (and should be done), and steroids should be started promptly, the most important investigation is MRI with gadolinium to exclude acoustic neuroma — present in 6–15% of SSNHL cases. Starting steroids without imaging misses this cause, and an acoustic neuroma found later may have grown enough to complicate surgical options. The correct approach is: PTA to confirm SNHL pattern → MRI same day or within 24 hours → high-dose steroids while awaiting/after MRI. Electrocochleography is for Meniere's disease assessment, not SSNHL workup.
Principles of Management
Management of hearing loss follows from the type and cause of the loss. Conductive losses are generally more amenable to definitive treatment because the cause (wax, fluid, perforation, ossicular fixation) can often be corrected; sensorineural losses are usually permanent and managed with rehabilitation rather than cure. The general principle is: treat reversible causes first, then consider amplification or cochlear implantation for irreversible loss. This distinction is both clinical and prognostic — telling a patient whether their hearing loss is reversible is one of the most impactful communications in ENT practice, and it rests entirely on correct classification. The following sections structure management by hearing loss type, moving from reversible causes to irreversible SNHL rehabilitation.
Management of CHL — treat the underlying cause:
- Wax impaction: syringing, microsuction, or softening drops (sodium bicarbonate/olive oil)
- Middle ear effusion (glue ear): grommets (ventilation tubes) in children with persistent bilateral effusion causing significant hearing loss (>25 dB bilateral); most resolve spontaneously within 3 months
- Tympanic membrane perforation (CSOM safe/tubotympanic): myringoplasty (TM repair) once ear is dry; closes the air-bone gap
- Ossicular chain disruption: ossiculoplasty (ossicular reconstruction using prostheses or autograft incus)
- Otosclerosis: stapedotomy (as discussed in the otosclerosis SDL)
- ASOM: antibiotic treatment; myringotomy if suppuration stage with severe pain
Management of SNHL:
SNHL is generally irreversible once established. Management aims to maximise communication:
- Hearing aids: The first-line intervention for most patients with significant SNHL. Modern digital aids amplify sound with frequency shaping to match the audiogram pattern. Types: behind-the-ear (BTE), receiver-in-canal (RIC), in-the-ear (ITE), completely-in-canal (CIC). Bone-anchored hearing aids (BAHA) when conventional aids are unsuitable (e.g. atresia, CSOM).
- Cochlear implantation: For profound bilateral SNHL (>90 dB) that does not benefit from conventional hearing aids. The device bypasses damaged hair cells and directly stimulates the cochlear nerve via an electrode array implanted in the scala tympani. Indications: post-lingually deafened adults with inadequate benefit from hearing aids; pre-lingually or peri-lingually deafened children (best outcomes if implanted before age 2–3 years, before the critical period for speech and language development closes). Contraindications: absent cochlear nerve, cochlear ossification (relative), active infection.
- SSNHL management (emergency — described in detail above): same-day assessment, MRI, high-dose systemic corticosteroids, intratympanic steroids as salvage.
- NIHL: Prevention primary (hearing protection ≥85 dB TWA); no medical treatment reverses established loss; hearing aids for functional rehabilitation.
- Ototoxicity: Avoid ototoxic drugs where alternatives exist; monitor audiology in patients requiring aminoglycosides or cisplatin; reduce dose and switch agent if early cochlear changes detected.
- Presbyacusis: Hearing aids remain the mainstay; communication training for family; social support to prevent isolation and depression.
CLINICAL PEARL
SSNHL is an otological emergency — every medical practitioner must know this. A patient who wakes up deaf in one ear should be seen the same day, not scheduled for a routine outpatient appointment in 3 weeks. The window for corticosteroid benefit narrows rapidly after onset: patients treated within the first week have significantly better outcomes than those treated after 2–4 weeks. The practical rule: any patient presenting with sudden unilateral hearing loss with a normal-appearing ear (no wax, intact TM, no infection) needs same-day ENT referral, PTA, and if confirmed SNHL, steroid treatment and MRI — in that clinical session.
Self-Assessment: Hearing Loss
This SDL has covered a broad topic — hearing loss classification, audiometric diagnosis, specific SNHL entities, and management principles. Self-assessment here works best as an integrative exercise: take the stem of a clinical scenario, diagnose the type of loss from the audiogram and history, and then reason through the management. The following questions are designed to require you to integrate multiple pieces of knowledge rather than recall isolated facts. Work through each question completely before checking the answer. Pay particular attention to the tuning-fork known-trap questions — Weber and Rinne interpretation is consistently the most examined and most frequently inverted topic in ENT examinations at finals level. If you can answer these without hesitation you are examination-ready on hearing loss.
Key concept checks:
- In unilateral SNHL, in which direction does Weber lateralise — and why?
- What is the definition of SSNHL and why does it constitute an otological emergency?
- Why does noise-induced hearing loss produce a notch specifically at 4000 Hz?
- Name two drugs that cause irreversible SNHL and explain their mechanism of cochlear toxicity.
- What tympanometry pattern would you expect in a patient with a large TM perforation?
- A child is found on neonatal screening to have absent OAEs bilaterally. What does this indicate, and what is the next step?
- What is the difference between Rinne positive and Rinne negative — which indicates CHL?
SELF-CHECK
A 70-year-old retired farmer presents with bilateral hearing difficulty. Pure-tone audiometry shows bilateral symmetric SNHL, greatest at high frequencies (4–8 kHz), with a gentle slope and no air-bone gap. Tympanometry is type A bilaterally. The most likely diagnosis is:
A. Noise-induced hearing loss — the bilateral notch at 4 kHz confirms this
B. Presbyacusis — bilateral symmetric high-frequency SNHL in an elderly patient without a discrete 4 kHz notch is typical
C. Bilateral acoustic neuromas (NF2)
D. Bilateral middle ear effusion
Reveal Answer
Answer: B. Presbyacusis — bilateral symmetric high-frequency SNHL in an elderly patient without a discrete 4 kHz notch is typical
Presbyacusis (age-related SNHL) presents as bilateral symmetric, gradually progressive high-frequency SNHL with a gently sloping audiogram — no discrete 4 kHz notch. The distinction from NIHL is important: NIHL shows a characteristic notch at 4 kHz with partial recovery at 8 kHz; presbyacusis shows a smoother downward slope continuing at 8 kHz without recovery. Type A tympanogram confirms normal middle ear (no effusion). Bilateral acoustic neuromas are extremely rare, would produce asymmetric loss and retrocochlear features, and would require MRI for NF2 screening. Middle ear effusion would produce CHL (air-bone gap) and a flat type B tympanogram.