Page 10 of 29
EN4.16 | Facial Nerve Palsy — SDL Guide
Learning Objectives
- Distinguish upper motor neurone from lower motor neurone facial palsy at the bedside
- Map the intratemporal course of the facial nerve and identify which functions are lost at each level of injury
- Use topognostic tests to localise the level of a facial nerve lesion
- Diagnose Bell's palsy as a diagnosis of exclusion and differentiate it from Ramsay Hunt syndrome, CSOM, and parotid causes
- Outline the principles of management including corticosteroids, antiviral therapy, and eye care
INSTRUCTIONS
Facial nerve palsy is one of the most recognisable neurological presentations in clinical medicine, and also one of the most clinically important because the immediate priority is eye protection to prevent corneal damage. This SDL covers the diagnosis and management of facial nerve palsy from the ENT perspective — particularly the distinction between Bell's palsy and secondary causes requiring investigation, and the use of topognostic testing to localise the level of the lesion.
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th ed., Ch. 17 (Facial Nerve) (textbook)
- Hazarika P — Textbook of Ear Nose Throat and Head & Neck Surgery, 3rd ed. (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Vol. 3, Ch. 241 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old woman wakes up and notices that the right side of her face is drooping. She cannot close her right eye, her mouth droops on the right, and her face feels numb. She presents to casualty. Two questions must be answered in the first 2 minutes: (1) Is this an upper motor neurone lesion (is the forehead spared — think stroke) or a lower motor neurone lesion (is the forehead also involved — think Bell's palsy)? (2) Is her cornea at risk? How do you answer both questions at the bedside, and what do you do in the next 30 minutes?
WHY THIS MATTERS
The facial nerve (VII) is the most commonly injured cranial nerve in clinical practice. Its long intratemporal course through narrow bony canals — running nearly 3 cm from the internal auditory canal to the stylomastoid foramen — makes it uniquely vulnerable to a wide range of pathologies: idiopathic inflammation, viral infection, temporal bone trauma, cholesteatoma, parotid tumour, and acoustic neuroma. Bell's palsy (idiopathic LMN facial palsy) accounts for approximately 70% of all cases and is the commonest cause of acute facial paralysis. However, 'Bell's palsy' is a diagnosis of exclusion — it is made only after secondary causes are considered and excluded. A facial palsy missed as 'just Bell's palsy' when it is actually caused by cholesteatoma eroding the facial canal, or by a parotid malignancy, leads to major harm. The immediate practical concern in any facial palsy is corneal protection: a paralysed eyelid that cannot close exposes the cornea to drying and ulceration within hours.
RECALL
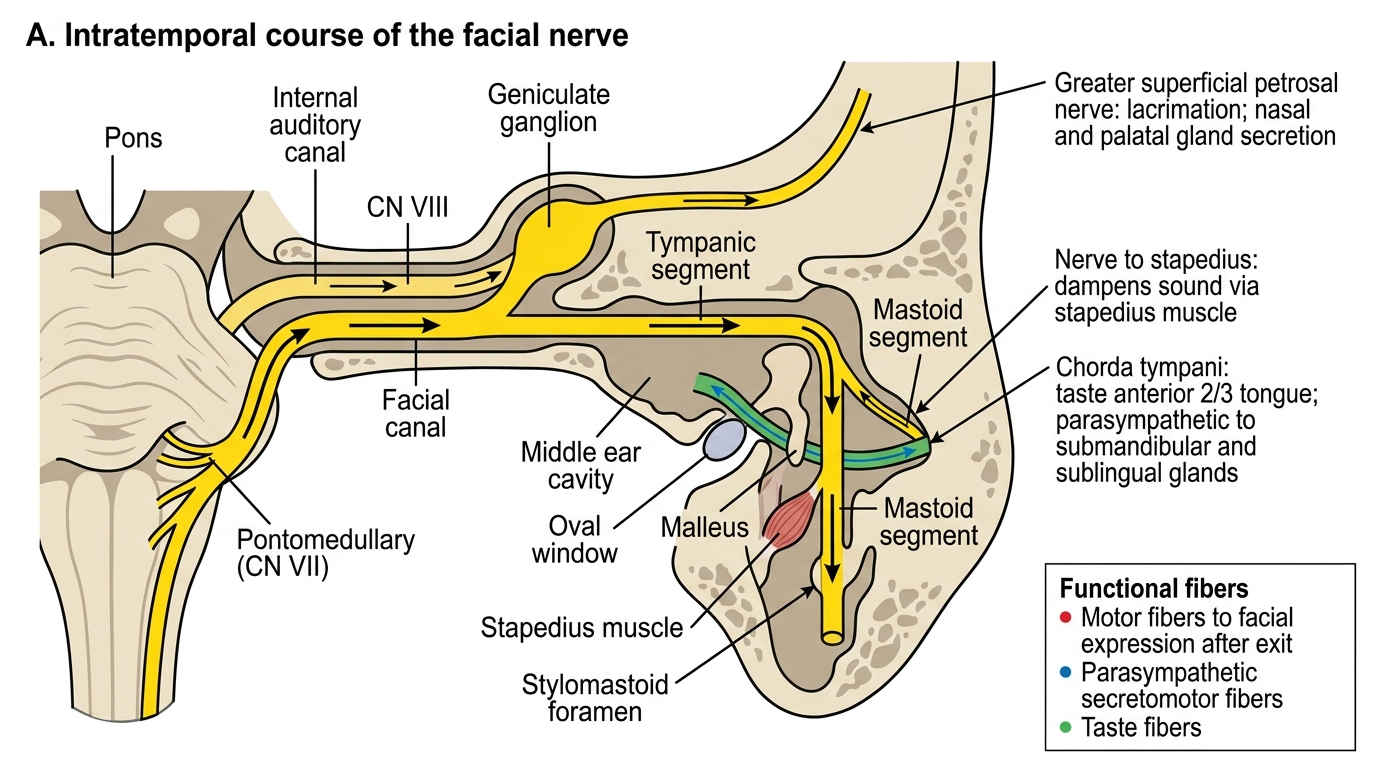
Recall the facial nerve's intracranial course: the motor nucleus is in the pons; the nerve exits the brainstem at the pontomedullary junction, enters the internal auditory canal (IAC) with the VIII nerve, and continues into the petrous temporal bone. Three important branches arise from the intratemporal segment before the nerve exits the skull at the stylomastoid foramen: (1) the greater superficial petrosal nerve (GSPN) from the geniculate ganglion — carries parasympathetic fibres to the lacrimal gland (tear secretion); (2) the nerve to stapedius from the tympanic/early mastoid segment — drives the stapedius muscle; (3) the chorda tympani from the mastoid segment — carries taste from the anterior two-thirds of the tongue and parasympathetic supply to the submandibular and sublingual glands. Also recall the UMN vs LMN rule for facial palsy: the forehead muscles (frontalis, corrugator) have BILATERAL cortical representation, so a unilateral supranuclear (UMN) lesion spares the forehead. In a peripheral (LMN) lesion, the forehead is involved on the same side — this is the bedside key test.
Clinical Presentation of Facial Nerve Palsy
Facial nerve palsy presents as ipsilateral weakness or paralysis of the muscles of facial expression. The first and most critical clinical task is to determine whether this is an upper motor neurone (UMN) or lower motor neurone (LMN) lesion, because the two have fundamentally different aetiologies and management pathways.
The forehead test is the bedside key: ask the patient to wrinkle the forehead (raise the eyebrows) or close the eyes tightly. In a UMN lesion, the forehead muscles are spared (bilaterally represented in the cortex), and only the lower face is weak contralateral to the lesion. In an LMN lesion, ALL facial muscles are involved ipsilateral to the lesion, including the frontalis — the patient cannot wrinkle the forehead on the affected side. This single observation redirects the diagnosis toward ENT/peripheral causes rather than stroke.
Additional clinical features of LMN facial palsy:
- Inability to close the eye on the affected side (orbicularis oculi weakness) — lagophthalmos
- On attempted eye closure, the eye rolls up and inward, exposing the white sclera — this is Bell's phenomenon (not Bell's palsy), a normal protective reflex
- Deviation of the mouth to the unaffected side when smiling
- Food collecting between cheek and teeth (buccinator weakness)
- Hyperacusis (stapedius paralysis — loss of stapedial reflex on affected side)
- Loss of taste in the anterior 2/3 of the tongue on the affected side (chorda tympani involvement)
- Reduced lacrimation if GSPN involved (lesion at or proximal to geniculate ganglion)
House-Brackmann grading provides standardised communication about severity:
- HB I: Normal function
- HB II: Mild dysfunction — slight weakness; complete eye closure with minimal effort
- HB III: Moderate dysfunction — obvious weakness; complete closure with effort; synkinesis possible
- HB IV: Moderately severe — incomplete eye closure; asymmetric mouth at rest
- HB V: Severe — barely perceptible movement; incomplete eye closure
- HB VI: Total paralysis — no movement
The onset is also informative. Bell's palsy typically reaches maximum severity within 48–72 hours; gradual progressive facial weakness over weeks or months is a red flag for a compressive lesion (parotid malignancy, acoustic neuroma, temporal bone metastasis).
Anatomy and Pathophysiology
The clinical usefulness of understanding facial nerve anatomy lies in its topognostic (site-of-lesion localising) implications. Because specific branches arise at specific points along the intratemporal course, the pattern of deficits — which functions are lost and which are preserved — allows the clinician to localise the lesion before any imaging is performed. This is the basis of topognostic testing.
The facial nerve is approximately 3 cm long within the temporal bone, making it the longest intratemporal course of any cranial nerve. This extended journey through a narrow bony canal (the fallopian canal) makes it uniquely vulnerable to injury. The three segments differ in their vulnerability: the labyrinthine segment is the narrowest and least vascular, making it most susceptible to compression from inflammatory oedema in Bell's palsy; the tympanic segment runs along the medial middle ear wall just above the oval window and is exposed to erosion by cholesteatoma or ASOM pus; the mastoid segment descends vertically to exit at the stylomastoid foramen and is the most accessible surgical target.
Intratemporal Course and Branches of the Facial Nerve
SELF-CHECK
A 52-year-old man presents with sudden left facial paralysis involving the forehead. He also has painful vesicles in the left ear canal. Audiometry shows mild left-sided SNHL. The most likely diagnosis is:
A. Bell's palsy (idiopathic LMN facial palsy)
B. Ramsay Hunt syndrome (herpes zoster oticus)
C. Left middle cerebral artery territory stroke
D. Parotid gland malignancy
Reveal Answer
Answer: B. Ramsay Hunt syndrome (herpes zoster oticus)
The combination of LMN facial palsy (forehead involved), painful vesicles in the ear, and SNHL is pathognomonic of Ramsay Hunt syndrome — VZV reactivation in the geniculate ganglion with spread to adjacent structures (VIII nerve, skin of the ear). Bell's palsy is idiopathic with no vesicles. A stroke produces UMN palsy (forehead spared, contralateral side, and no ear vesicles). Parotid malignancy produces a slowly progressive palsy without vesicles and without SNHL.
Investigations
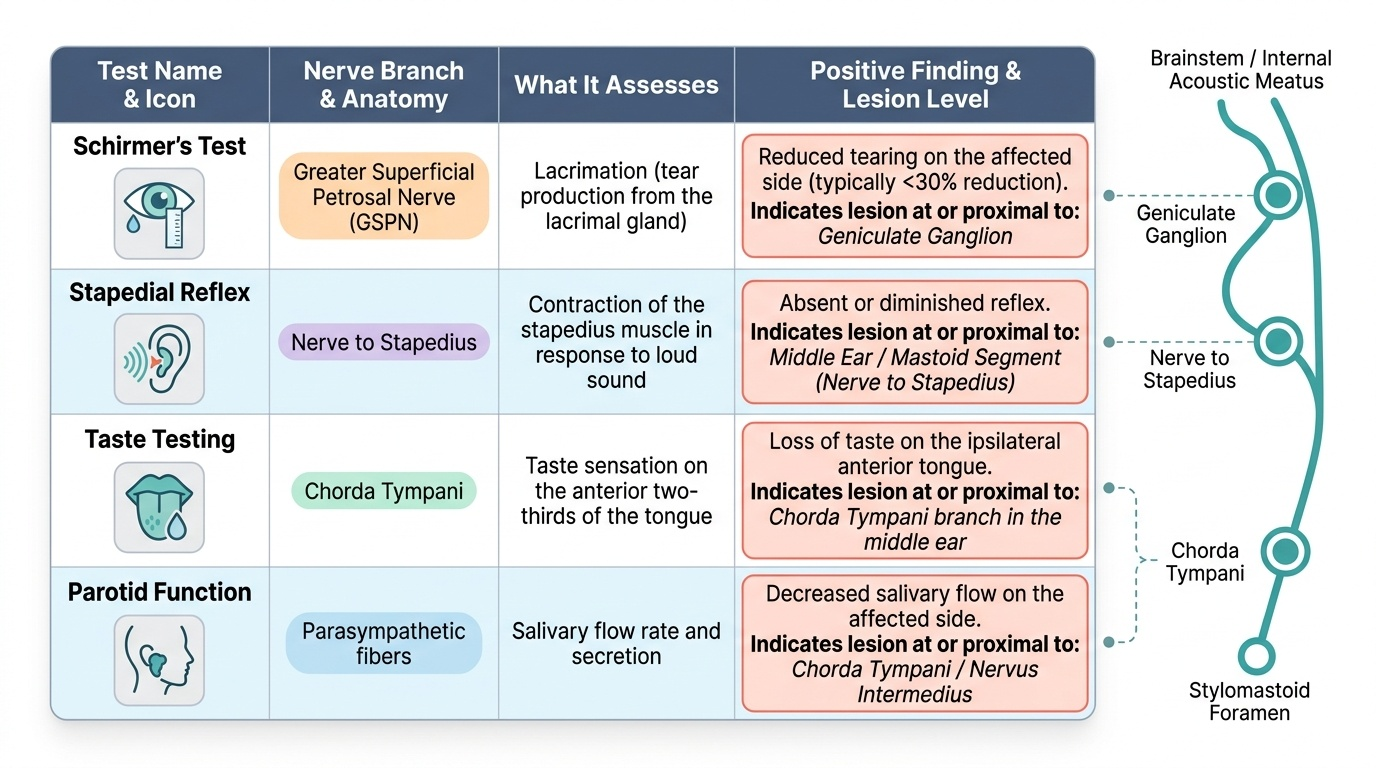
Investigations in facial nerve palsy serve two purposes: topognostic localisation (identifying the anatomical level of the lesion) and aetiological diagnosis (identifying the underlying cause). The two are related but distinct — imaging identifies mass lesions and cholesteatoma; topognostic tests use functional deficit patterns to estimate the level of injury.
Provided image
The investigation sequence is clinical-history-directed. When the history and otoscopy suggest Bell's palsy in a straightforward presentation, topognostic tests are performed in the clinic without imaging. When there are red flags (slow onset, ear discharge, parotid mass, bilateral palsy, head trauma), imaging takes priority. Audiometry is useful in all cases because sensorineural hearing loss points to VIII nerve involvement (Ramsay Hunt, acoustic neuroma) or middle ear disease (CSOM). The following tests are conducted in ascending order of complexity, from bedside to specialist electrophysiology.
Topognostic tests — these test which branches are affected and therefore where the lesion is: