Page 4 of 29
EN4.13 | Otosclerosis — SDL Guide
Learning Objectives
- Describe the clinical presentation of otosclerosis including the characteristic audiological profile
- Explain the pathophysiology of otosclerosis and the mechanism of the Carhart's notch
- Interpret the key investigations — pure-tone audiometry, tympanometry, and HRCT temporal bone
- Construct a differential diagnosis for progressive conductive hearing loss in a young adult
- Outline the principles of medical and surgical management, distinguishing stapedectomy from stapedotomy
INSTRUCTIONS
Otosclerosis is the paradigm case of progressive conductive hearing loss in a young adult without any history of ear disease or discharge. It is important because it is treatable — surgical correction with stapedectomy or stapedotomy offers excellent hearing restoration — but it can be missed or misattributed if the clinician does not recognise the characteristic audiological profile. This SDL builds on your knowledge of the ossicular chain and tuning-fork tests to help you understand why otosclerosis produces the specific pattern it does, and how to distinguish it from other causes of conductive hearing loss.
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th ed., Ch. 12 (Otosclerosis) (textbook)
- Hazarika P — Textbook of Ear Nose Throat and Head & Neck Surgery, 3rd ed. (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Vol. 3, Ch. 233 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman presents to your clinic with a 3-year history of gradually worsening hearing in both ears. She reports that she can hear better in noisy environments than in quiet ones — a strange observation she has noticed at parties. There is no history of ear discharge, pain, or trauma. Her mother also has hearing loss. On examination the tympanic membranes are intact and normal-appearing, and tuning-fork tests show Rinne negative bilaterally with Weber lateralising to the right. What is the most likely diagnosis, and what single clinical-audiological finding would most strongly support it?
WHY THIS MATTERS
Otosclerosis is one of the most common causes of progressive hearing loss in young adults in the Indian subcontinent, with a prevalence of approximately 1–2% in the general population and a higher familial incidence. Unlike most ear diseases, otosclerosis affects an intact, normal-looking ear — there is no discharge, no perforation, and no history of infection. This makes it a diagnosis that requires active clinical thinking rather than passive observation. The condition is important for three reasons: first, it is highly treatable — surgery restores serviceable hearing in over 90% of patients; second, it worsens with pregnancy (oestrogen accelerates disease), making early diagnosis important in young women; and third, misattributing it to noise damage or psychological factors leads to unnecessary delays in a curative intervention.
RECALL
Recall the ossicular chain: the malleus is attached to the tympanic membrane; it articulates with the incus, which articulates with the stapes. The stapes consists of a head, two crura, and a footplate that sits in the oval window — a membrane-covered opening into the vestibule of the inner ear. Sound energy is transmitted as mechanical vibration from the TM through the chain to the stapes footplate, which pushes fluid in the inner ear. Any fixation of the stapes footplate interrupts this mechanical transmission and produces conductive hearing loss. Recall also from your tuning-fork training: Rinne negative (BC > AC) indicates CHL; Weber lateralises to the MORE affected (worse) ear in CHL — the opposite direction from SNHL. This is a critical known-trap: do not reverse CHL and SNHL for Weber.
Clinical Presentation of Otosclerosis
Otosclerosis presents with a characteristic clinical profile that distinguishes it from other causes of hearing loss. The typical patient is a young adult — most commonly a woman in her second or third decade — presenting with bilateral, slowly progressive, predominantly conductive hearing loss. The onset is insidious and is usually noticed first as difficulty understanding speech in quiet environments. A distinctive and diagnostically useful symptom is paracusis Willisii — the paradoxical phenomenon of hearing better in noisy environments than in quiet ones. This occurs because background noise stimulates speakers to raise their voices or to project more forcefully, while the patient's conductive loss effectively filters out the background noise and the louder signal reaches the cochlea more easily than in a quiet room.
Key features of the history:
- Bilateral hearing loss in 70–80% of cases (though one ear is usually affected before the other)
- No history of ear disease — no discharge, no pain, no perforation, no trauma or noise exposure
- Positive family history in approximately 25–40% of cases (autosomal dominant with variable penetrance)
- Worsening with pregnancy — oestrogen accelerates the pathological bone remodelling; deterioration often noticed or reported during pregnancy
- Tinnitus — low-pitched, bilateral, often described as a 'hum' rather than a high-pitched ring
On examination, the most important finding is the normal-appearing tympanic membrane in a patient with significant conductive hearing loss — this combination immediately points to a middle-ear or ossicular problem rather than a perforated eardrum. In active disease, a faint pinkish blush may be seen through the intact TM in the region of the oval window — this is the Schwartze sign (also called 'flamingo pink sign'), reflecting the hypervascular active otosclerotic focus shining through the thin tympanic membrane. It is present in only a minority of cases but is pathognomonic when present.
Tuning-fork findings:
- Rinne negative (BC > AC): characteristic of CHL; in otosclerosis, bone conduction is intact while air conduction is blocked by stapes fixation
- Weber lateralises to the more affected ear (worse hearing side): a key distinction from SNHL where Weber lateralises away from the affected side
- Absolute bone conduction (ABC test): normal in pure conductive otosclerosis; reduced in cochlear involvement
Anatomy and Pathophysiology of Otosclerosis
Otosclerosis is fundamentally a disease of abnormal bone remodelling confined to the otic capsule — the bony housing of the inner ear. The otic capsule is unique in human anatomy: it is the only bone that normally undergoes no remodelling after birth. Its bone is the densest and most mineralised in the body, maintained in a static state by suppression of osteoclast and osteoblast activity. In otosclerosis, this suppression fails locally, and focal areas of the otic capsule undergo aberrant resorption (appearing as 'spongy' vascular bone — hence the older term otospongiosis) followed by re-deposition of immature, poorly mineralised, vascular lamellar bone. The resulting abnormal bone progressively expands and can anchor adjacent mobile structures. The earliest and most clinically important target is the stapes footplate at the oval window.
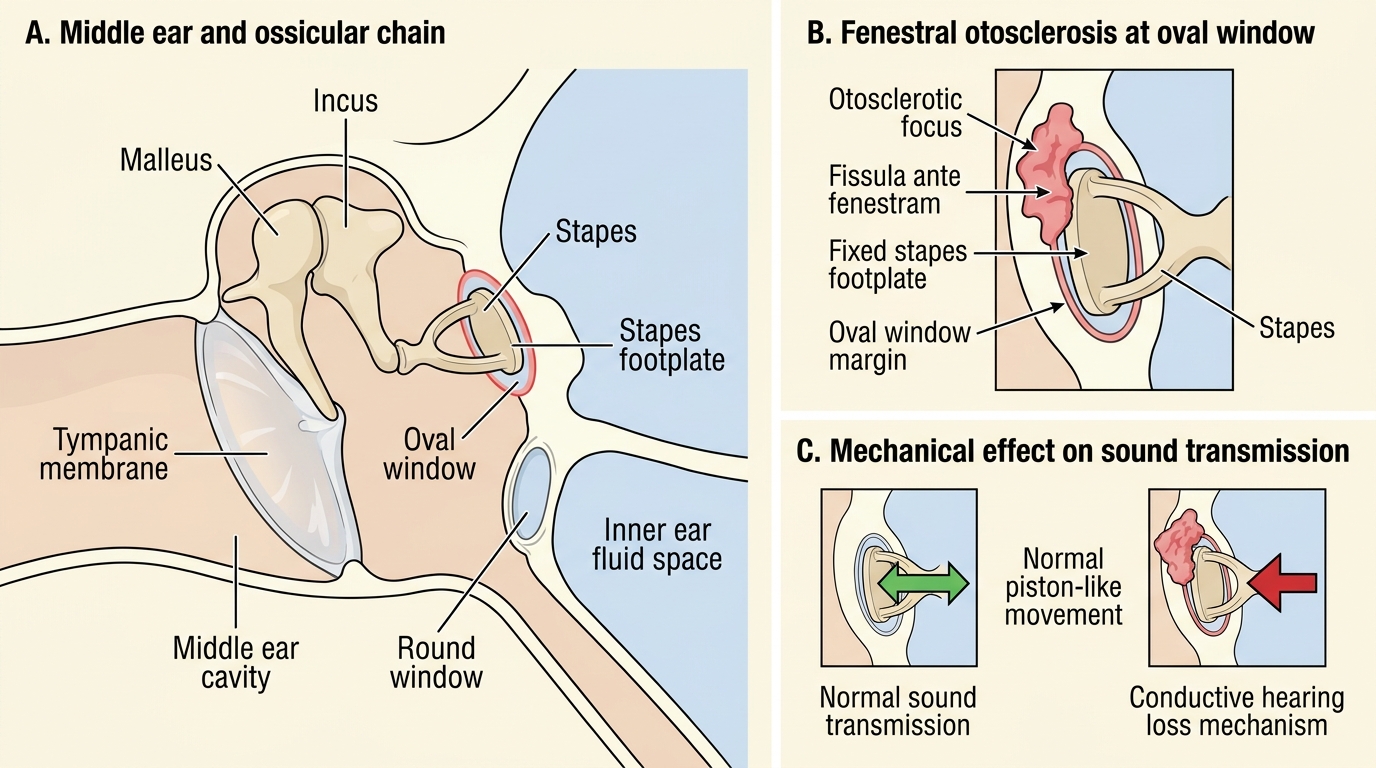
Fenestral Otosclerosis Fixing the Stapes Footplate
The most common site of abnormal remodelling is the fishbone area (fissula ante fenestram) — a small cleft in the otic capsule immediately anterior to the oval window. As the otosclerotic focus expands, it encroaches on the oval window and anchors the stapes footplate, progressively restricting its normal piston-like movement. This is fenestral otosclerosis, the commonest form, and it produces a pure or predominantly conductive hearing loss by impeding the mechanical transmission of sound to the inner ear fluid.
In a minority of cases (approximately 10–15%), the otosclerotic focus extends to involve the cochlear endosteum — the inner bone layer surrounding the cochlear duct. This cochlear (retrofenestral) otosclerosis disrupts the ionic environment of the endolymph and may damage the sensory hair cells, producing a sensorineural or mixed hearing loss component in addition to the conductive element.
Two key pathophysiological concepts explain specific audiological findings:
1. Schwartze sign: In active disease the otosclerotic focus is highly vascular (osteoclast-rich spongiotic phase). The overlying tympanic membrane is thin, and the pink-red blush of the vascular bone is sometimes visible through it — this is the Schwartze sign. Its presence indicates active, progressive disease.
2. Carhart's notch: On pure-tone audiometry, patients with stapes fixation show a characteristic dip in bone conduction at 2000 Hz (sometimes also at 500 Hz and 4000 Hz). This 'notch' does NOT represent cochlear hair cell damage; it is a mechanical artefact caused by the reduced inertial bone-conduction contribution of the stapes when it is fixed. The notch disappears after successful stapedectomy, confirming its mechanical rather than sensory origin. This is important: the bone conduction threshold at 2000 Hz underestimates true cochlear reserve and should not be used at face value when counselling patients about surgical outcomes.
SELF-CHECK
A 30-year-old woman with bilateral progressive hearing loss has a pure-tone audiogram showing an air-bone gap of 40 dB bilaterally. The bone conduction curve shows a dip at 2000 Hz that is otherwise within normal limits. The most accurate interpretation of the 2000 Hz bone conduction dip is:
A. Evidence of early cochlear sensorineural hearing loss requiring urgent investigation
B. Carhart's notch — a mechanical artefact of stapes fixation that resolves after stapedectomy, not true cochlear loss
C. Noise-induced hearing loss superimposed on the conductive component
D. Cochlear otosclerosis indicating the disease has spread to the inner ear
Reveal Answer
Answer: B. Carhart's notch — a mechanical artefact of stapes fixation that resolves after stapedectomy, not true cochlear loss
The 2000 Hz dip on bone conduction in stapes fixation is Carhart's notch — a mechanical artefact, not true sensorineural cochlear loss. It results from reduced inertial bone conduction at the resonant frequency of the ossicular chain when the stapes is fixed. The diagnostic importance is that it must not be mistaken for cochlear damage when planning surgery; it resolves after successful stapedectomy. The air-bone gap of 40 dB combined with an otherwise normal bone conduction curve in a young woman is classic otosclerosis.
Investigations in Otosclerosis
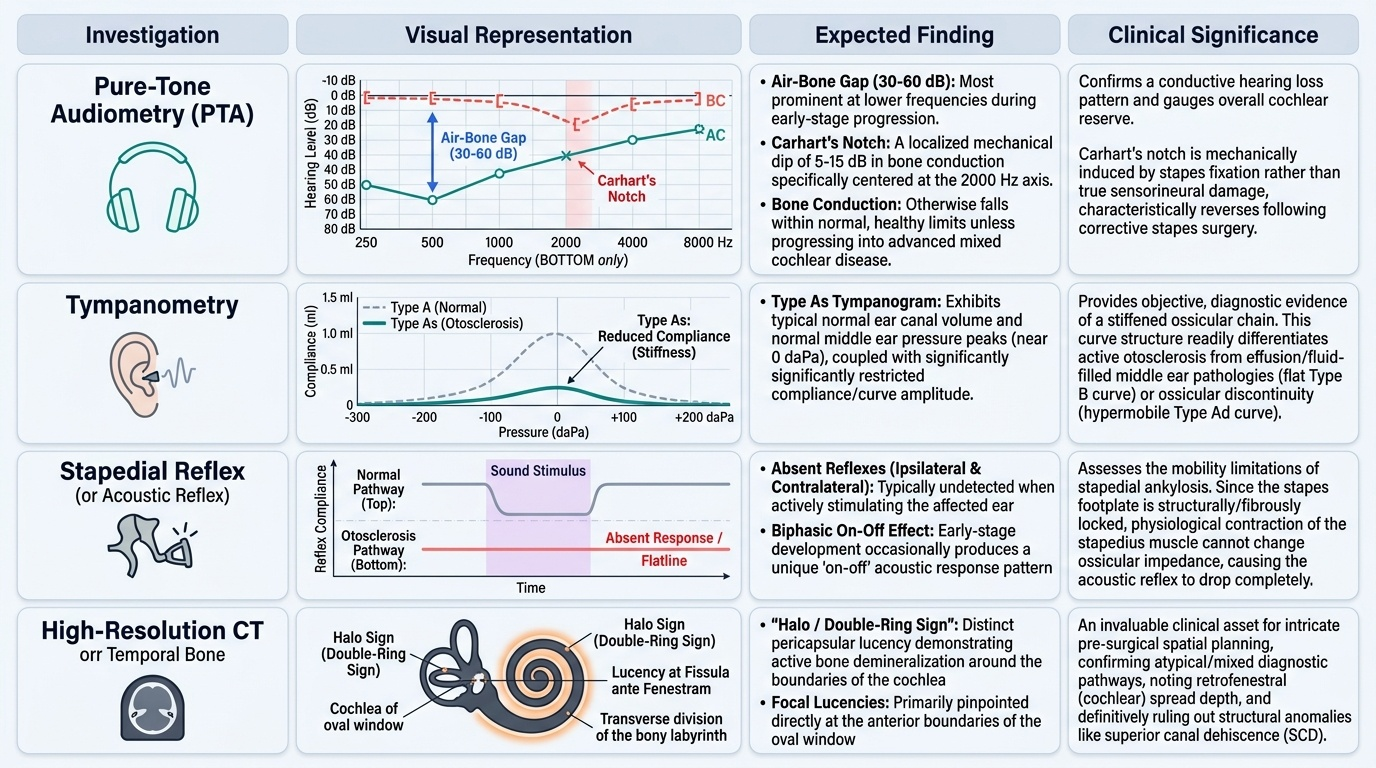
Investigations in otosclerosis aim to confirm the pattern of conductive hearing loss, assess the degree of cochlear reserve, exclude other causes of CHL, and guide surgical planning. The workup is primarily audiological, with imaging reserved for atypical cases or pre-surgical assessment. A structured approach moves from basic hearing tests (pure-tone audiometry) through acoustic immittance assessment (tympanometry and reflexes) to electrophysiology (ABR) and finally imaging. Each investigation answers a specific question: how much hearing is lost and of which type? Is the middle ear stiff or mobile? Is the eighth nerve affected? Is the disease confined to the oval window or has it spread to the cochlea? Understanding what each test asks — and what answer to expect in otosclerosis — is essential for both diagnosis and pre-surgical counselling.
Provided image
1. Pure-tone audiometry (PTA): The key findings are:
- Air-bone gap of 30–60 dB, greatest at low frequencies in early disease
- Carhart's notch — a dip of approximately 5–15 dB in bone conduction at 2000 Hz (mechanical artefact of stapes fixation, NOT cochlear loss)
- Bone conduction otherwise within normal limits in purely fenestral disease
- Mixed pattern (air-bone gap plus elevated bone conduction) in cochlear otosclerosis
2. Tympanometry: The tympanogram is typically a type As curve — a shallow (reduced amplitude/compliance) tympanogram with a normal peak pressure. The reduced compliance reflects the stiffened ossicular chain from stapes fixation. This is in contrast to a flat (B) tympanogram seen in middle ear effusion or a large-peak (Ad) tympanogram seen in ossicular discontinuity.
3. Stapedial reflex (acoustic reflex): The stapedial reflex is absent in otosclerosis because the stapes cannot contract against a fixed footplate. This is an important finding: an absent ipsilateral reflex with an intact TM and clear middle ear strongly suggests stapes fixation.
4. Auditory brainstem response (ABR): In pure fenestral otosclerosis, ABR shows prolonged absolute latencies at all waves (reflecting the conductive component) but normal inter-peak latencies (the neural pathway is intact). This distinguishes it from retrocochlear pathology.
5. High-resolution CT (HRCT) temporal bone: Not always required for diagnosis but useful for:
- Pre-surgical assessment of footplate thickness, oval window patency
- Detection of the 'halo sign' — a hypodense ring around the cochlea on CT indicating active cochlear otosclerosis
- Ruling out superior semicircular canal dehiscence (SSCD) — another cause of CHL with an intact TM that can mimic otosclerosis on audiometry