Page 20 of 29
EN4.19 | Tinnitus — SDL Guide (Part 2)
Diagnosis and Differential Diagnosis
The diagnosis of tinnitus is clinical — the patient reports the symptom, and the clinical assessment characterises it. The diagnostic task is not to confirm that tinnitus is present but to identify its underlying cause, so that any treatable underlying condition is managed and serious causes are excluded. This requires a structured approach that moves from the symptom characteristics (subjective/objective, pulsatile/non-pulsatile, unilateral/bilateral) to the audiological assessment to targeted imaging when indicated.
Provided image
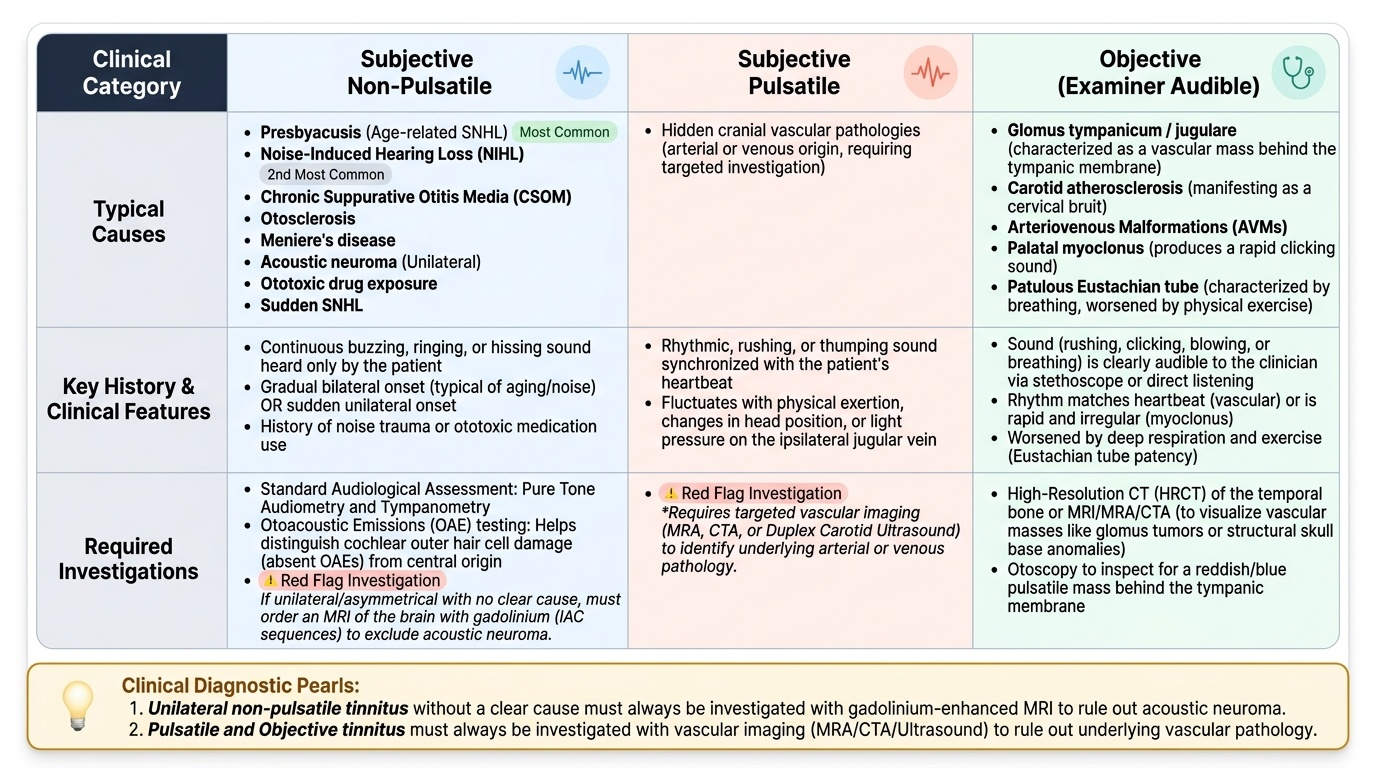
The most important clinical distinction is between the two red flag patterns — unilateral tinnitus and pulsatile tinnitus — each of which requires a specific investigation. Unilateral tinnitus in a patient without a clear ipsilateral cause must be investigated for acoustic neuroma. Pulsatile tinnitus must be investigated for vascular pathology. All other patterns (bilateral, non-pulsatile, with associated SNHL) can be managed clinically with audiological assessment and explanation before imaging is requested.
Common non-pulsatile causes by prevalence: age-related SNHL (presbyacusis, most common), NIHL (second most common), CSOM, otosclerosis, Meniere's disease, acoustic neuroma, ototoxic drug exposure, sudden SNHL.
Objective tinnitus — identifiable by the examiner: glomus tympanicum/jugulare (pulsatile, vascular mass), carotid atherosclerosis (bruit), AVM, palatal myoclonus (clicking sound), patulous Eustachian tube (sound of breathing, worsened by exercise).
Distinguishing tinnitus of cochlear origin from central tinnitus can be difficult clinically; OAE testing helps (absent OAEs suggest cochlear outer hair cell damage).
SELF-CHECK
A 35-year-old man presents with a 6-week history of new-onset unilateral right-sided tinnitus. He has no history of noise exposure and no ear disease. Otoscopy is normal. Rinne and Weber tests are normal bilaterally. The most important next step is:
A. Reassure him that unilateral tinnitus without hearing loss is always benign and does not need investigation
B. MRI brain with gadolinium (IAC sequences) to exclude acoustic neuroma
C. Start tinnitus retraining therapy immediately without imaging
D. Audiometry is sufficient — no imaging is needed if the audiogram is normal
Reveal Answer
Answer: B. MRI brain with gadolinium (IAC sequences) to exclude acoustic neuroma
Unilateral tinnitus without an obvious cause is a red flag that mandates MRI with gadolinium to exclude acoustic neuroma. Acoustic neuromas can present with unilateral tinnitus as the sole early symptom, even before measurable hearing loss develops on audiometry. A normal audiogram does NOT exclude an acoustic neuroma. Reassurance without imaging is not appropriate for new unilateral tinnitus in a young adult. TRT can be initiated later for symptom management, but investigation must come first to exclude a structural cause.
Principles of Management
The management of tinnitus follows a logical sequence: first, identify and treat any underlying reversible cause; second, counsel the patient to correct misconceptions and reduce tinnitus-related distress; third, implement evidence-based interventions to habituate the tinnitus response; and fourth, ensure hearing rehabilitation if SNHL is present. There is no universally effective pharmacological cure for tinnitus, and patients must be counselled that the goal of management is to reduce distress and functional impact — not necessarily to make the tinnitus inaudible.
Step 1 — Treat the underlying cause where possible:
Management of CSOM (surgery/antibiotics), correction of wax impaction, cessation of ototoxic drugs, treatment of Meniere's disease, stapedotomy for otosclerosis, surgery for glomus tumour. In many cases, treating the underlying cause reduces but does not eliminate the tinnitus — central plasticity changes may persist even after the peripheral cause is removed.
Step 2 — Counselling and education (essential, immediate):
Patients with tinnitus commonly fear it represents a serious disease, that it will get worse indefinitely, or that it indicates imminent deafness. Correcting these misconceptions reduces anxiety, which itself reduces tinnitus severity (anxiety amplifies tinnitus perception). Key messages: tinnitus is common, not life-threatening, and often improves or habituates over time; the loudness matched on audiometric testing is typically only 5–10 dB above threshold (much smaller than perceived).
Step 3 — Tinnitus retraining therapy (TRT):
TRT combines directive counselling (explaining the neurophysiological model of tinnitus to demystify it) with sound therapy (broadband neutral white or pink noise at a low level to reduce the contrast between tinnitus and background silence, promoting neural habituation). It is delivered over 12–24 months in a structured programme. TRT has the best quality evidence of any non-pharmacological tinnitus intervention.
Step 4 — Cognitive behavioural therapy (CBT):
CBT addresses the emotional and attentional response to tinnitus — reducing catastrophising, improving sleep, and restoring daily function. Multiple RCTs confirm reduction in tinnitus distress and improved quality of life. NICE 2020 guidelines recommend CBT for chronic, distressing tinnitus. CBT and TRT can be combined.
Step 5 — Hearing aids:
If there is significant SNHL, a hearing aid reduces the contrast between tinnitus and the amplified environmental sound, providing passive masking and improving communication. Modern hearing aids with tinnitus noise generator programmes combine amplification with active tinnitus masking.
Pharmacological agents:
No drug has consistent, clinically significant long-term evidence for tinnitus suppression. Agents tried (with limited/no sustained evidence): melatonin (for sleep), betahistine (only if Meniere's is the cause), and various anxiolytics. Antidepressants are used for comorbid depression/anxiety, not for tinnitus itself.
CLINICAL PEARL
When a patient presents with new unilateral tinnitus, the first thought should be: could this be an acoustic neuroma? Tinnitus is the second most common presenting symptom of acoustic neuroma (after hearing loss), and it can occur before any measurable hearing loss develops. An audiogram that appears normal does NOT exclude an acoustic neuroma — only MRI does. The clinical habit to develop is: any new, persistent unilateral tinnitus without an obvious cause in a patient aged 20–70 = MRI with gadolinium, IAC sequences. Missing this investigation is the commonest tinnitus-related medicolegal issue in ENT practice.
Self-Assessment: Tinnitus
Tinnitus is an examination topic that rewards classification-first thinking: the moment you can place a patient's tinnitus into the correct category (subjective/objective, pulsatile/non-pulsatile, unilateral/bilateral, with or without hearing loss), the investigation and management strategy follows logically. The questions below require you to apply this classification approach to clinical scenarios rather than recall isolated facts. Before answering each question, mentally classify the tinnitus described and identify the single most important investigation or management decision. The most important clinical habit to consolidate is the red flag reflex — unilateral tinnitus means MRI, pulsatile tinnitus means vascular imaging — and applying this consistently across varied presentations is what separates a safe, thorough, and evidence-informed ENT clinician from a dismissive one.
Key concept checks:
- What is the difference between subjective and objective tinnitus, and how is objective tinnitus identified?
- What does pulsatile tinnitus indicate, and what investigation does it require?
- Why does unilateral tinnitus in a young adult mandate MRI, even if the audiogram is normal?
- What is the neurophysiological model of non-pulsatile subjective tinnitus?
- What is tinnitus retraining therapy, and what are its two components?
- Name two evidence-based non-pharmacological treatments for chronic tinnitus.
- What audiometric pattern would suggest acoustic neuroma in a patient with unilateral tinnitus?
SELF-CHECK
A 60-year-old woman with chronic bilateral tinnitus and bilateral high-frequency SNHL from long-standing noise exposure is significantly distressed, with poor sleep and anxiety. Her tinnitus loudness matches to approximately 8 dB above her hearing threshold at 6000 Hz. The most effective evidence-based intervention for her tinnitus distress is:
A. Betahistine 24 mg three times daily for 6 months
B. Combined tinnitus retraining therapy and cognitive behavioural therapy
C. Surgical division of the cochlear nerve to eliminate the peripheral source
D. High-dose prednisolone for 2 weeks to reduce cochlear inflammation
Reveal Answer
Answer: B. Combined tinnitus retraining therapy and cognitive behavioural therapy
For chronic bilateral noise-induced tinnitus with significant distress, the evidence-based treatment is a combination of tinnitus retraining therapy (TRT — directive counselling + sound therapy) and cognitive behavioural therapy (CBT), which reduce tinnitus-related distress and improve quality of life in RCTs. Betahistine is only indicated if Meniere's disease is the cause (not bilateral NIHL). Cochlear nerve section does not reliably eliminate tinnitus in most patients — the central generator may persist. Steroids have no evidence for chronic NIHL-related tinnitus. The tinnitus loudness match of 8 dB above threshold is a useful counselling point — the tinnitus seems louder subjectively than it actually is.