Page 14 of 29
EN4.17 | Vertigo with Vestibular Function Assessment — SDL Guide (Part 2)
Diagnosis and Differential Diagnosis
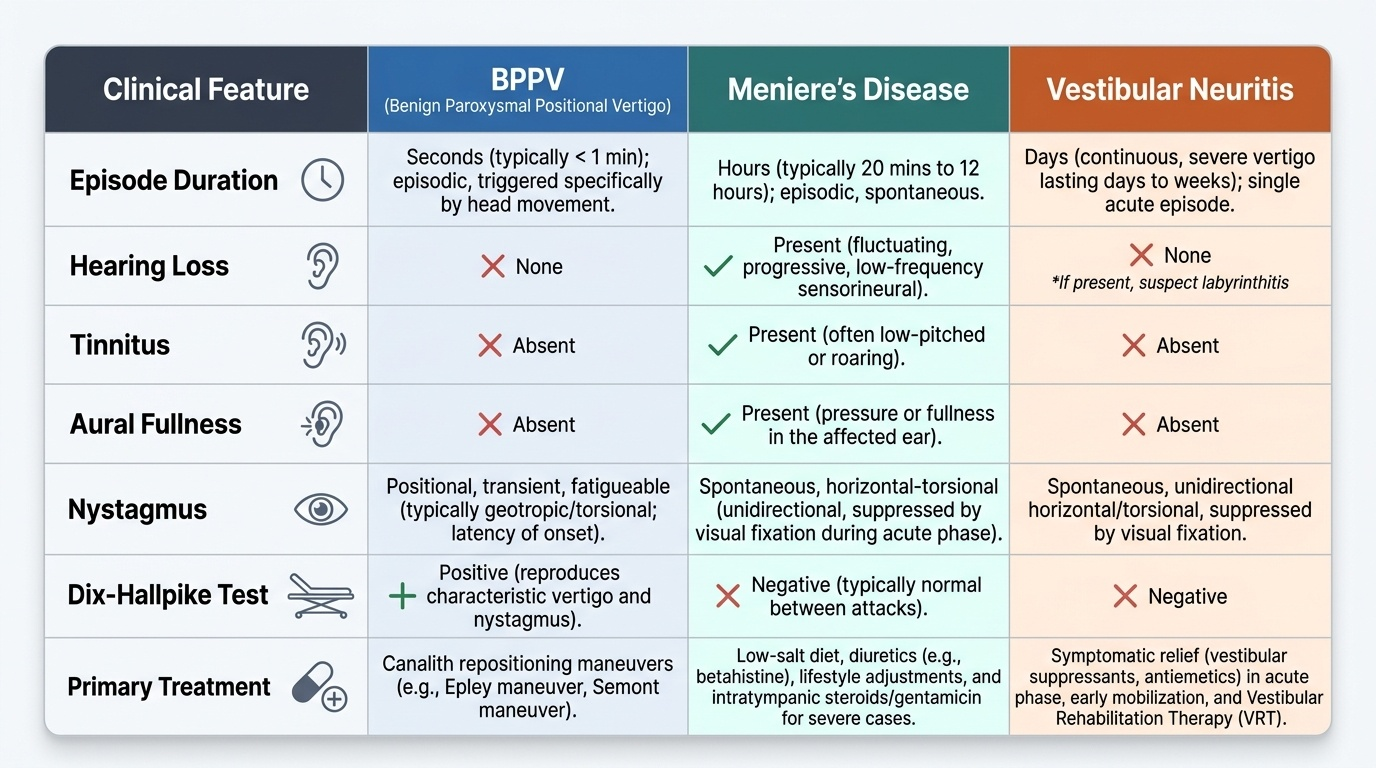
The diagnostic approach to vertigo is primarily history-driven. The duration and pattern of episodes, presence or absence of hearing loss, relationship to head position, and any associated neurological symptoms direct the clinician toward the correct diagnosis in most cases. Formal vestibular testing confirms the clinical impression and quantifies the deficit. The most important differential to make in any acute spontaneous vertigo is peripheral versus central — the HINTS examination was developed specifically for this purpose. The three common peripheral causes can be diagnosed at the bedside in the outpatient setting without any specialist equipment, using the history and the Dix-Hallpike test as primary tools. The table below summarises the distinguishing features of BPPV, Meniere's disease, and vestibular neuritis in a side-by-side comparison that is useful for examination preparation.
Provided image
HINTS examination for acute spontaneous vertigo (distinguishing peripheral from central):
The HINTS battery (Head Impulse test, Nystagmus type, Test of Skew) is a validated bedside tool for distinguishing acute peripheral from central vestibular syndrome in patients presenting with acute continuous vertigo:
- H — Head Impulse test: positive (corrective saccade) = peripheral vestibular loss (vestibular neuritis); negative (no corrective saccade) = central (brainstem/cerebellar) lesion
- I — Nystagmus: unidirectional horizontal/torsional, suppressed by fixation = peripheral; direction-changing or purely vertical = central
- N — skew deviation (Test of Skew): no vertical skew = peripheral; vertical skew (misalignment of eyes) = central
A pattern of: positive HIT + unidirectional nystagmus + no skew = peripheral (HINTS for PERIPHERAL).
A pattern of: negative HIT OR direction-changing nystagmus OR skew = central (any one of these is enough to be concerned).
The HINTS examination in trained hands has higher sensitivity for cerebellar stroke than early CT brain (which misses 20–40% of posterior fossa strokes in the first 24–48 hours).
Specific diagnosis summary:
- BPPV: episodic (seconds), positional, no hearing symptoms, positive Dix-Hallpike with fatigable upbeat-torsional nystagmus → treat with Epley manoeuvre in the same visit
- Meniere's disease: episodic (20 min – hours), with the triad (SNHL + tinnitus + aural fullness + vertigo), audiogram showing low-frequency SNHL → betahistine, dietary sodium restriction
- Vestibular neuritis: acute continuous vertigo (days), no hearing loss, positive HIT toward the affected side, canal paresis on caloric testing → prochlorperazine acutely, then vestibular rehabilitation
- Labyrinthitis: same as vestibular neuritis + hearing loss → oral steroids considered, VRT
- Central (posterior fossa stroke): acute onset, may be minimal nausea/vomiting compared to peripheral, negative HIT, direction-changing nystagmus, cerebellar ataxia → emergency MRI
SELF-CHECK
In the HINTS examination for acute spontaneous vertigo, which finding would indicate a CENTRAL cause (requiring urgent imaging) rather than a peripheral cause?
A. Positive head impulse test with corrective saccade toward the left
B. Unidirectional horizontal nystagmus suppressed by visual fixation
C. Direction-changing nystagmus (rightbeat gaze right, leftbeat gaze left)
D. Unilateral canal paresis on caloric testing
Reveal Answer
Answer: C. Direction-changing nystagmus (rightbeat gaze right, leftbeat gaze left)
Direction-changing nystagmus (gaze-evoked nystagmus) is a central sign in the HINTS battery — it indicates a brainstem or cerebellar pathology rather than a peripheral vestibular lesion. A positive HIT (corrective saccade) indicates peripheral vestibular loss. Unidirectional nystagmus suppressed by fixation is a peripheral sign. Canal paresis on caloric testing is a peripheral vestibular finding. In the HINTS battery, any ONE of the three central signs (negative HIT, direction-changing/vertical nystagmus, vertical skew) should trigger urgent MRI brain — CT misses 20–40% of early posterior fossa strokes.
Principles of Management
Management of vertigo is condition-specific: BPPV is treated with canalith repositioning manoeuvres in the clinic; Meniere's disease is managed medically to reduce frequency of attacks; vestibular neuritis is treated symptomatically in the acute phase followed by vestibular rehabilitation to promote central compensation. Central vertigo requires specialist referral and condition-specific management (thrombolytics, surgery, or disease-modifying therapy for MS). The guiding principle is that peripheral vestibular disorders are usually self-limiting or manoeuvre-treatable, and the goal of management is to hasten central compensation and prevent recurrence.
1. BPPV — Canalith Repositioning (Epley Manoeuvre)
The Epley manoeuvre is the evidence-based first-line treatment for posterior canal BPPV. It moves the displaced otoconia out of the posterior canal back into the utricle by guiding the patient through a sequence of five head positions, allowing gravity to reposition the canalith. Meta-analyses show resolution in approximately 80% of patients after one session, with additional sessions bringing the total success rate to >90%. The manoeuvre is performed in the clinic, requires no equipment, and takes 5 minutes. For horizontal canal BPPV, the Barbeque (barrel) roll (Lempert) manoeuvre is used instead.
2. Meniere's Disease — Reducing Attacks
Medical management aims to reduce the frequency and severity of vertigo attacks and slow the progression of hearing loss:
- Dietary sodium restriction (low-salt diet, <1.5–2 g/day) and adequate fluid intake — to reduce endolymph volume
- Betahistine (8–24 mg three times daily): an H3 antagonist and H1 agonist that improves cochlear microcirculation and reduces endolymphatic pressure; widely used in India per Dhingra; evidence supportive but not from large RCTs
- Diuretics (e.g. acetazolamide, hydrochlorothiazide): reduce endolymph production; used as adjunct
- Vestibular suppressants (prochlorperazine, betahistine) during acute attacks for symptom relief
- Intratympanic gentamicin (chemical labyrinthectomy): for intractable vertigo not responding to medical therapy; sacrifices remaining hearing on the affected side in exchange for vertigo control
- Endolymphatic sac decompression surgery: controversial; some benefit in select cases
3. Vestibular Neuritis — Recovery and Rehabilitation
Acute phase (first few days): vestibular suppressants (prochlorperazine 10 mg IM or oral; promethazine) for acute nausea and vertigo. Oral prednisolone (50 mg/day tapered over 3 weeks) improves recovery of vestibular function if started within the first 3 days (Strupp et al. RCT). Antivirals (acyclovir) are not recommended routinely — evidence does not support adding them.
Recovery phase: vestibular rehabilitation therapy (VRT) — a structured programme of gaze stabilisation exercises and balance training that promotes central compensation of the unilateral vestibular deficit. VRT is the most important intervention for persistent dizziness after the acute phase. Long-term vestibular suppressants should be avoided beyond the first few days — they impede central compensation.
4. Central vertigo: Urgent specialist referral; cerebellar stroke may require thrombolytics or neurosurgical intervention; MS managed by neurology.
CLINICAL PEARL
The most common diagnostic error in vertigo is to miss BPPV by failing to perform the Dix-Hallpike test. A patient presenting with brief positional vertigo who is given vestibular suppressants and sent home, when what they actually need is an Epley manoeuvre performed in the clinic, is a missed opportunity: ~80% of BPPV resolves in one session. Every clinician seeing patients with dizziness should be competent in performing the Dix-Hallpike and Epley manoeuvres. Conversely, the most dangerous error is to reassure a patient with an acute vestibular syndrome as 'just vestibular neuritis' without performing the HINTS examination — a posterior fossa stroke can be missed for days by this assumption.
Self-Assessment: Vertigo
Vertigo is a high-yield ENT and medicine examination topic because it requires integrating vestibular anatomy, the pathophysiology of three distinct disorders, clinical examination skills (Dix-Hallpike, HINTS), audiometric interpretation, and condition-specific management. The questions below require both factual recall and clinical reasoning — try to construct a full clinical reasoning chain for each question rather than simply selecting an answer. This reflective approach to self-assessment is more effective for developing the pattern-recognition skills needed in OSCEs and viva examinations. In particular, be prepared to justify why a negative head impulse test is more concerning than a positive one — this is counter-intuitive and frequently tested in clinical viva rounds at finals. Practise generating the answer aloud, and then check against the SDL content above.
Key concept checks:
- What is the duration of a typical BPPV episode, and how does this differ from Meniere's disease?
- What does the Dix-Hallpike test detect, and what are the four characteristics of a positive result?
- A patient with acute vertigo has a NEGATIVE head impulse test. Is this peripheral or central — and why does it matter?
- Name the three components of the Meniere's disease triad and the underlying pathophysiology.
- How does the Epley manoeuvre work mechanistically?
- What is vestibular rehabilitation therapy and what does it achieve?
- What audiogram pattern would you expect in vestibular neuritis?
SELF-CHECK
A 30-year-old woman has had three episodes in the past 6 months of severe vertigo lasting 2–3 hours, accompanied by a low-pitched roaring noise in the left ear and a sensation of fullness in that ear. After each episode, her hearing partially improves but does not return to normal. The most likely diagnosis is:
A. Benign paroxysmal positional vertigo (BPPV)
B. Vestibular neuritis
C. Meniere's disease
D. Acoustic neuroma
Reveal Answer
Answer: C. Meniere's disease
This is classic Meniere's disease: episodic vertigo lasting hours (2–3 hours fits the 20-minute to several-hour range), accompanied by low-frequency fluctuating SNHL (roaring tinnitus + aural fullness + partially recovering hearing). The hearing loss that does not fully recover after each episode indicates progressive cochlear damage from repeated endolymphatic ruptures. BPPV produces seconds-duration positional vertigo without hearing symptoms. Vestibular neuritis produces a single prolonged episode of vertigo (days) without hearing loss. Acoustic neuroma produces slowly progressive unilateral SNHL without episodic vertigo.