Page 5 of 23
EN4.4 | Otitis Media with Effusion — SDL Guide (Part 2)
Diagnosis and Differential Diagnosis
The diagnosis of OME is made by integrating the clinical history (chronic hearing loss without acute inflammation), otoscopic findings (dull retracted amber TM, possible air-fluid level or bubbles, no erythema or bulging), and tympanometry (Type B curve). The combination of these three elements makes the diagnosis robust. A single tympanometric reading should not be acted on in isolation — OME is defined as a middle ear effusion persisting for at least 3 months, and the management decision is guided by duration and functional impact rather than a single snapshot finding.
The most important diagnostic distinction to make is between OME and ASOM — these are frequently confused by students because both involve middle ear fluid. The differences are systematic and should be committed to memory. OME is chronic, non-inflammatory, non-febrile, and painless; ASOM is acute, inflammatory, febrile, and painful. The TM in OME is retracted, dull, and amber; in ASOM it is hyperaemic, bulging (Stage 3), or perforated (Stage 4). This distinction drives completely different management: OME requires watchful waiting and eventual possible surgical drainage, not antibiotics; ASOM requires antibiotics and possibly urgent myringotomy.
Differential diagnosis table:
| Feature | OME | ASOM | Otitis Externa | Chronic CSOM |
|---|---|---|---|---|
| Duration | Weeks to months | Days to weeks | Days | Months to years |
| Otalgia | Absent or mild | Severe | Severe (tragal tenderness) | Absent or mild |
| Fever | Absent | Present | Absent | Absent |
| Discharge | Absent | Stage 4 only | Present (canal) | Present (through perforation) |
| TM appearance | Dull, amber, retracted | Hyperaemic, bulging or perforated | Normal (when visible) | Central perforation visible |
| Tympanometry | Type B | Type B (during effusion) | Type A | Type B or Tympanosclerosis |
Persistent unilateral OME in an adult: a red flag. Unlike children (where bilateral OME from adenoid hypertrophy is the norm), an adult presenting with unilateral OME — especially with associated nasal obstruction, epistaxis, neck lymphadenopathy, or cranial nerve involvement — must be urgently evaluated by flexible nasendoscopy to exclude nasopharyngeal carcinoma (NPC). NPC commonly presents in young to middle-aged adults of South-East Asian descent and frequently causes unilateral Eustachian tube obstruction as its first clinical sign. Failure to perform nasendoscopy in a unilateral adult OME is a serious clinical error.
SELF-CHECK
A 45-year-old Chinese man presents with a 6-week history of unilateral right ear fullness and reduced hearing. He has no ear pain, no fever, no discharge. Otoscopy shows a dull retracted right TM. Tympanometry is Type B on the right. The most critical next investigation is:
A. PTA with bone conduction thresholds to distinguish conductive from sensorineural loss
B. Flexible nasendoscopy to exclude a nasopharyngeal mass obstructing the Eustachian tube
C. CT temporal bone to assess middle ear anatomy
D. Watchful waiting for 3 months and tympanometry recheck
Reveal Answer
Answer: B. Flexible nasendoscopy to exclude a nasopharyngeal mass obstructing the Eustachian tube
Unilateral OME in an adult — especially of South-East Asian descent — is a red flag for nasopharyngeal carcinoma (NPC), which commonly presents as unilateral Eustachian tube obstruction causing middle ear effusion. Flexible nasendoscopy is mandatory in every adult with unilateral OME to visualise the nasopharynx and ET orifice before any other management decision. Watchful waiting for 3 months (the approach for children with bilateral OME) is inappropriate here — delaying nasendoscopy risks missing a surgically resectable NPC. PTA and CT are important secondary investigations but do not replace the primary obligation to exclude a nasopharyngeal mass.
Management of OME
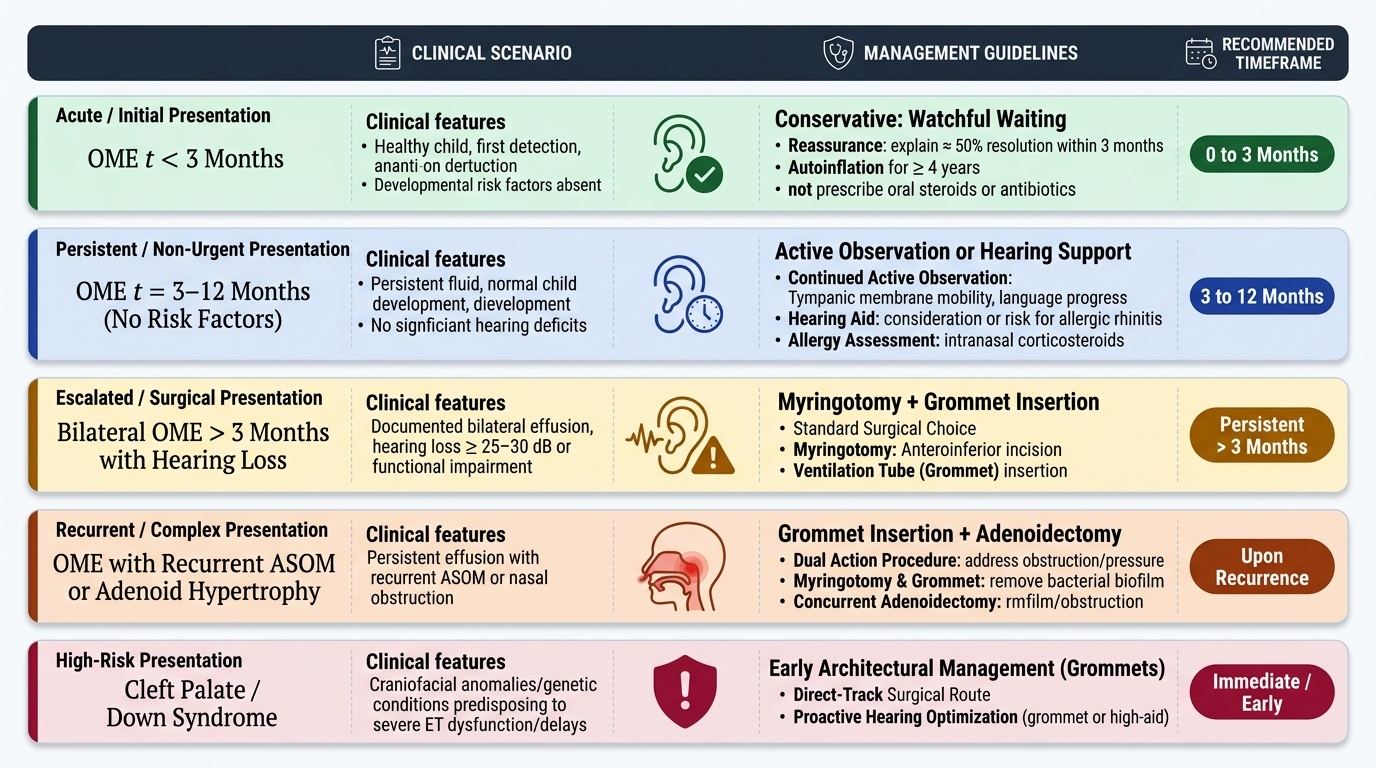
The management of OME is guided by three factors: the duration of the effusion, the degree of hearing loss and its functional impact on the child's development or daily life, and the presence of risk factors for hearing-related developmental harm. The natural history of OME is predominantly self-resolving — approximately 50% of cases resolve spontaneously within 3 months and around 90% within 12 months in otherwise healthy children. This favourable natural history is the basis for the evidence-based watchful waiting approach endorsed by NICE, AAP, and Dhingra/Hazarika: a single abnormal tympanogram at one visit is not an indication for surgery. However, the children who do not resolve spontaneously, and those who develop significant hearing loss during critical developmental windows, require timely surgical intervention to prevent lasting consequences. The challenge in clinical practice is identifying the threshold between waiting and acting — which requires integrating tympanometric evidence, hearing assessment, and functional information from parents and teachers.
Provided image
Conservative management (first-line for all children):
- Watchful waiting for 3 months from the diagnosis of OME (or from the time of first detection) — most cases resolve without intervention
- Hearing aid as an alternative to surgery in children who are unsuitable for surgery (e.g. due to anaesthetic risk) or parental preference; allows hearing correction during the waiting period
- Autoinflation (Otovent device): The child blows up a nasal balloon with one nostril, inflating the balloon by raising nasopharyngeal pressure — this forces the ET open and allows equalisation of middle ear pressure. Non-invasive; modest evidence of benefit in cooperative children ≥4 years
- Treat underlying cause: If allergic rhinitis is contributing to ET dysfunction, intranasal corticosteroids may reduce mucosal oedema and improve ET function; antihistamines have not been shown to be effective for OME
- Antibiotics and oral corticosteroids are NOT recommended for OME (no proven sustained benefit; risk of adverse effects)
Surgical management:
- Myringotomy with grommet (ventilation tube) insertion: The standard surgical intervention for persistent OME; performed under general anaesthesia as a day procedure in children. The myringotomy is made in the anteroinferior quadrant; the grommet (a small flanged tube) is inserted through the incision to bypass ET dysfunction and allow air ventilation of the middle ear. Hearing improves immediately post-insertion. The grommet typically extrudes spontaneously over 6–12 months; the TM heals behind it.
- Indications for grommet insertion: (1) Bilateral OME with hearing loss >25 dB persisting for ≥3 months AND affecting speech development or school performance; (2) Unilateral OME persisting ≥6 months; (3) OME with associated TM changes (retraction pocket, early atelectasis) indicating structural risk; (4) OME in high-risk groups (cleft palate, Down syndrome) — these patients may benefit from early grommet insertion without the 3-month wait
- Adenoidectomy: Adding adenoidectomy to grommet insertion reduces recurrence rates in children aged ≥4 years with recurrent OME or documented adenoid hypertrophy. The adenoid is a reservoir of bacteria/biofilm and mechanically obstructs the ET — removal addresses both mechanisms.
- Adenoidectomy alone (without grommets): An option for recurrent OME in older children (≥4 years) where adenoid hypertrophy is the clear aetiology, particularly when the OME is mild
Post-grommet care:
- Avoid water getting into the ear during bathing and swimming (custom ear moulds or cotton wool with Vaseline)
- Follow up at 4–6 weeks to confirm improved hearing, and at grommet extrusion to confirm TM healing
- Most short-stay grommets extrude by 12 months; persistent OME after extrusion may require re-insertion
CLINICAL PEARL
The single most important rule in adult OME is: flexible nasendoscopy first. A middle-aged adult presenting with unilateral OME is presumed to have a nasopharyngeal mass obstructing the Eustachian tube until proven otherwise. Do not watchfully wait an adult with new unilateral OME without first visualising the nasopharynx — nasopharyngeal carcinoma is a treatable disease when caught early and can present silently as a unilateral ear effusion months before any obvious nasal or cervical sign appears.
Self-Assessment: Key Concepts in OME
At this point in the module, consolidate the following essential framework before attempting the self-check questions. OME is the most common cause of acquired hearing loss in children, characterised by chronic non-suppurative middle ear effusion without acute inflammation — the hallmark is a hearing loss noticed by a parent or teacher in an otherwise well child. The mechanism is Eustachian tube dysfunction leading to negative middle ear pressure, serous transudate, and eventually mucoid metaplasia (goblet cell proliferation) producing the viscous 'glue ear' fluid. Adenoid hypertrophy is the most common surgically addressable contributing cause in children. The otoscopic findings are distinctive but subtle: dull amber or grey-blue retracted TM, no erythema, no bulging, possible air-fluid level. Tympanometry Type B (flat) curve is the most sensitive non-invasive test for effusion. Management follows a staged approach: watchful waiting for 3 months, then surgery (myringotomy + grommet insertion ± adenoidectomy) for persistent cases with significant hearing loss. In adults, unilateral OME always warrants flexible nasendoscopy to exclude nasopharyngeal carcinoma before any conservative management is undertaken.
Key facts for self-testing:
- OME duration classification: acute <3 weeks, subacute 3–12 weeks, chronic >12 weeks
- Glue ear = mucoid subtype with viscous goblet-cell secretion
- Tympanometry Type B = flat = fluid; Type C = negative pressure only; Type A = normal
- Watchful waiting: 3 months before surgical decision in most healthy children
- Surgical intervention: myringotomy + grommet in anteroinferior quadrant
- Adult unilateral OME: nasendoscopy mandatory to exclude NPC
- Cleft palate and Down syndrome: ET dysfunction chronic — early grommet intervention indicated
SELF-CHECK
Which tympanometric finding most reliably confirms middle ear effusion in a child with suspected OME?
A. Type A tympanogram (normal peaked compliance curve)
B. Type B tympanogram (flat curve across all pressures)
C. Type C tympanogram (peak shifted to negative pressure)
D. No tympanometric finding can confirm effusion — PTA is required
Reveal Answer
Answer: B. Type B tympanogram (flat curve across all pressures)
A Type B (flat) tympanogram indicates near-zero TM compliance regardless of ear canal pressure, which occurs when fluid is present in the middle ear behind the TM — this is the hallmark tympanometric finding of OME. A Type A curve (normal) makes significant effusion unlikely. A Type C curve indicates negative middle ear pressure (ET dysfunction without frank effusion — a precursor to OME but not confirmatory of it). PTA alone cannot confirm effusion — it quantifies hearing loss but does not differentiate the mechanism.