Page 3 of 15
EN1.1 | Anatomy and Physiology of Ear, Nose, Throat, Head and Neck — SDL Guide (Part 3)
Physiology of Voice, Speech, and Swallowing
The larynx and pharynx collaborate in two of the most complex neuromuscular processes in the human body — phonation/speech and swallowing — using the same structures in sequence and with exquisite timing.
Phonation and Voice Production
Phonation is the production of sound at the laryngeal level. During quiet breathing, the vocal cords are abducted (separated) by the posterior cricoarytenoid muscles, allowing free airflow. When voicing, the vocal cords are adducted (brought together) by the lateral cricoarytenoid and interarytenoid muscles, and subglottic air pressure builds until it overcomes the closing force of the adducted cords. The cords then blow apart, the pressure falls, the Bernoulli effect (acceleration of the airstream through the narrowed glottis creates a pressure drop) and the elastic recoil of the cord tissue snap the cords shut again — and the cycle repeats. This is the myoelastic-aerodynamic theory of phonation, and the rate of repetition is the fundamental frequency (~125 Hz for adult male voice, ~200 Hz for female, higher in children). Pitch is increased by tensing the vocal cords (cricothyroid muscle elongates and thins the cords, raising vibration frequency).
Speech requires three components beyond the laryngeal sound source:
- Phonation (larynx): generates the fundamental buzzing sound.
- Resonance (pharynx, oral cavity, nasal cavity, paranasal sinuses): amplifies and shapes the sound quality (voice timber, nasal quality).
- Articulation (tongue, lips, teeth, palate): shapes the resonating sound into consonants and vowels.
Disease at any level produces characteristic speech change: cord palsy → breathy dysphonia; supraglottic oedema → muffled 'hot potato voice'; adenoid hypertrophy → hyponasal voice; velopharyngeal insufficiency → hypernasal voice.
Swallowing (Deglutition)
Swallowing is a semi-voluntary neuromuscular process divided into three phases:
- Oral phase (voluntary): The tongue shapes food into a bolus and propels it posteriorly toward the oropharynx. The soft palate elevates to close off the nasopharynx (preventing nasal regurgitation). This phase can be initiated voluntarily.
2. Pharyngeal phase (reflex, approximately 1 second): Once the bolus touches the anterior faucial pillars and posterior pharyngeal wall, the swallowing reflex is triggered (coordinated by the swallowing centre in the medulla via CN IX and X afferents and efferents). A precisely coordinated sequence occurs:
- Soft palate elevates and contacts the posterior pharyngeal wall (Passavant's ridge), sealing the nasopharynx.
- Larynx elevates (thyrohyoid muscle shortens) and moves anteriorly.
- Epiglottis retroflexes over the laryngeal inlet, deflecting the bolus laterally into the pyriform sinuses.
- Vocal cords adduct tightly (laryngeal closure).
- The upper oesophageal sphincter (cricopharyngeus muscle) relaxes to allow bolus entry into the oesophagus.
This sequence takes approximately 0.5–1.0 seconds and is so tightly coordinated that respiration is involuntarily suspended during it.
- Oesophageal phase: Primary peristaltic wave propels the bolus down the oesophagus in approximately 8–10 seconds to the lower oesophageal sphincter.
Impaired pharyngeal phase swallowing (from stroke, motor neurone disease, post-radiotherapy, or skull base disease affecting CN IX/X) carries the risk of aspiration — entry of food/liquid into the larynx and trachea. Silent aspiration (aspiration without coughing/choking) is particularly dangerous because the patient may be unaware. Clinical signs: wet/gurgly voice after swallowing, recurrent aspiration pneumonia, unexplained weight loss.
SELF-CHECK
A patient undergoes total thyroidectomy. Postoperatively, she has hoarseness and difficulty swallowing solid food. She can still change her pitch on command. Which nerve is most likely injured?
A. Both recurrent laryngeal nerves (bilateral RLN palsy)
B. Right recurrent laryngeal nerve unilaterally (cord palsy, cricothyroid intact)
C. External branch of the superior laryngeal nerve only
D. Internal branch of the superior laryngeal nerve
Reveal Answer
Answer: B. Right recurrent laryngeal nerve unilaterally (cord palsy, cricothyroid intact)
Hoarseness with dysphagia and a unilateral cord palsy after thyroidectomy points to unilateral RLN injury. The RLN supplies all intrinsic laryngeal muscles except the cricothyroid, which is supplied by the external branch of the SLN. Since she can still change pitch (cricothyroid intact), the external SLN is not injured. Bilateral RLN injury would cause severe respiratory distress (both cords paralyse in the paramedian position, nearly occluding the airway) — a surgical emergency. Internal SLN injury would cause supraglottic sensory loss and aspiration, not hoarseness. This is the single most important variant: right RLN is identified and at risk in the right lobe dissection; both RLNs are at risk in total thyroidectomy.
Head and Neck Anatomy: Spaces, Glands, Lymphatics, and Thyroid
The neck contains the major neurovascular highways of the body (carotid arteries, jugular veins, CN IX–XII) compressed into a relatively small space, surrounded by fascia-bounded compartments that determine how infection, tumour, and trauma spread. Mastery of this anatomy is essential for understanding deep space neck infections, cervical lymphadenopathy, salivary gland disease, and thyroid/parathyroid disorders.
Deep Cervical Fascial Spaces
The deep cervical fascia divides the neck into compartments, the most clinically important being: The deep cervical fascia creates the anatomical scaffolding that determines how disease spreads — infection following the path of least resistance between fascial layers, tumours invading along nerve sheaths or crossing compartment boundaries, and lymphatic drainage following predictable routes that make the nodal level of a metastasis a clinical indicator pointing to the primary site. Three fascial spaces demand particular clinical attention: the parapharyngeal space (the hub through which peritonsillar, parotid, and dental infections can spread toward the skull base), the retropharyngeal space (childhood retropharyngeal abscess), and the danger space (which connects the neck to the posterior mediastinum and explains why deep neck infections carry a mortality rate when untreated).
- Parapharyngeal space (prestyloid and retrostyloid compartments): lateral to the pharynx, medial to the parotid gland; contains the internal carotid artery, internal jugular vein, and CNs IX–XII (in the retrostyloid compartment). Peritonsillar abscess can extend into the parapharyngeal space.
- Retropharyngeal space: between the posterior pharyngeal wall and the prevertebral fascia; contains loose areolar tissue and lymph nodes (prominent in children — retropharyngeal abscess). Importantly, this space is continuous with the danger space (between the alar and prevertebral fascia), which communicates with the posterior mediastinum — explaining how neck infections can descend to cause descending necrotising mediastinitis, a life-threatening complication.
- Submandibular space and the sublingual space: important in Ludwig's angina (bilateral submandibular and sublingual space infection, usually from mandibular molar roots, potentially causing airway compromise by displacing the tongue superiorly).
Salivary Glands
- Parotid gland: the largest salivary gland; lies anterior and inferior to the ear, in the retromandibular fossa. Produces primarily serous saliva. The facial nerve (CN VII) divides into its five terminal branches (temporal, zygomatic, buccal, marginal mandibular, cervical) within the parotid substance — making parotid surgery a delicate exercise in facial nerve preservation. Stensen's duct (parotid duct) opens into the oral mucosa opposite the upper second molar.
- Submandibular gland: lies in the submandibular triangle deep to the mandible. Produces mixed serous/mucous saliva. Wharton's duct (submandibular duct) opens at the sublingual papilla on the floor of the mouth. The lingual nerve (CN V3) curves around Wharton's duct in an important surgical relation. The hypoglossal nerve (CN XII) passes deep to the gland. Submandibular gland calculi (sialolithiasis) are the commonest salivary calculi because saliva is more viscous and the duct has an uphill course.
- Sublingual glands: multiple small glands on the floor of the mouth; drain via multiple small ducts (ducts of Rivinus) directly into the floor of the mouth.
Cervical Lymph Node Levels (I–VII)
The cervical lymph nodes are grouped into levels I–VII (Memorial Sloan Kettering/UICC classification), which is essential for staging head and neck malignancies and planning neck dissection:
- Level I: submental (Ia) and submandibular (Ib) nodes — drain lips, floor of mouth, anterior oral tongue.
- Level II: upper deep cervical nodes (upper jugular chain), from skull base to hyoid — drain oropharynx, oral cavity, nasopharynx, parotid.
- Level III: middle deep cervical nodes (middle jugular chain), from hyoid to the omohyoid muscle — drain oropharynx, larynx, hypopharynx.
- Level IV: lower deep cervical nodes (lower jugular chain), from omohyoid to clavicle — drain larynx, hypopharynx, oesophagus.
- Level V: posterior triangle nodes (spinal accessory chain) — drain nasopharynx, oropharynx, skin of posterior scalp/neck.
- Level VI: central compartment nodes (pretracheal, paratracheal, prelaryngeal/Delphian node) — drain thyroid, larynx, trachea, oesophagus.
- Level VII: superior mediastinal nodes — drain thyroid, oesophagus.
Thyroid Gland and Parathyroids
The thyroid gland consists of right and left lobes connected by an isthmus at the 2nd–3rd tracheal ring level. A pyramidal lobe (remnant of the thyroglossal duct) is present in approximately 50% of individuals. The recurrent laryngeal nerve ascends in the tracheoesophageal groove, passing in close relation to the posterior surface of each thyroid lobe before entering the larynx at the inferior cornu of the thyroid cartilage — the critical nerve at risk in thyroidectomy. The superior thyroid artery (first branch of the external carotid artery) descends to the upper pole of each lobe; the external branch of the SLN runs closely alongside this artery — vulnerable to ligation with the superior thyroid artery during thyroidectomy (producing pitch problems). Four parathyroid glands (superior and inferior pairs) lie on the posterior surface of the thyroid, supplied by the inferior thyroid artery; inadvertent removal or devascularisation causes postoperative hypocalcaemia.
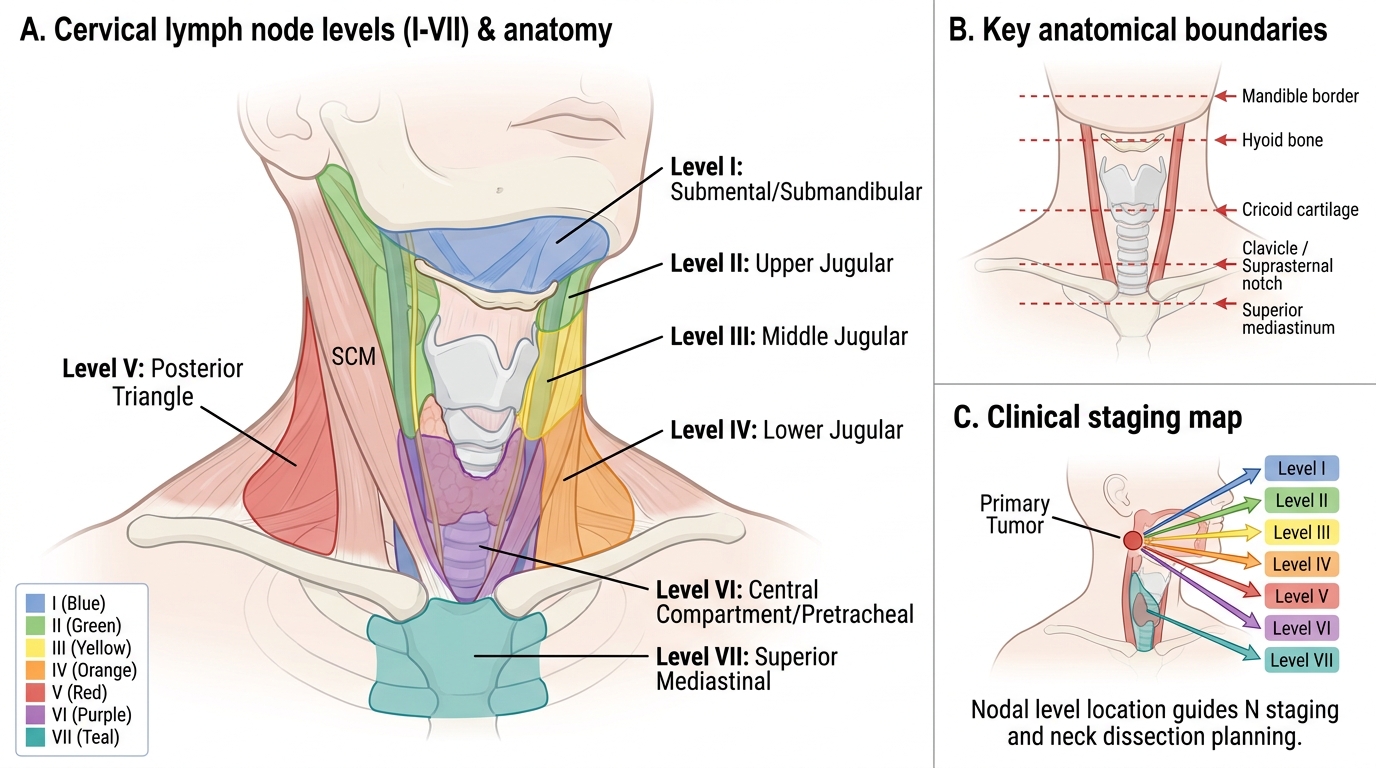
Cervical Lymph Node Levels I-VII
Clinical Correlations: Putting Anatomy to Work
ENT examination is the systematic clinical application of the anatomical knowledge outlined above. Each ENT examination technique is designed to assess a specific compartment, and findings are only interpretable if the examiner knows the underlying anatomy. This section maps the anatomy to clinical examination and the investigation methods that extend it.
Ear Examination
Otoscopy uses the anatomical landmarks of the tympanic membrane to characterise what is normal (grey, translucent, intact, with visible handle of malleus and light reflex) and what is abnormal. A dull, amber-coloured TM that moves poorly with Siegel's speculum pneumatic attachment suggests a middle ear effusion. A central perforation of the pars tensa in an ear with mucopurulent discharge = tubotympanic (safe/mucosal) CSOM — the mucosal disease type. A perforation or retraction pocket in the pars flaccida (Shrapnell's membrane) or at the posterior-superior margin with a keratin-filled retraction pocket = atticoantral (unsafe/squamosal) CSOM with cholesteatoma — the dangerous type requiring surgery.
Nasal Examination
Anterior rhinoscopy (using a Thudichum speculum and head-mirror or headlight) visualises the anterior one-third of the nasal cavity: the septum, the inferior turbinate, the floor, and the anterior part of the middle turbinate. Posterior rhinoscopy (using a mirror or rigid Hopkins rod endoscope) visualises the posterior choanae, the nasopharynx, and the Eustachian tube orifices.
Referred Otalgia — Anatomical Basis for Clinical Reasoning
Earalgia without a primary ear lesion is explained by the multiple nerves supplying the external ear and EAC (CN V3, VII, IX, X, C2/C3). Common causes:
- Dental caries/abscess → CN V3 (auriculotemporal nerve)
- Tonsillitis, peritonsillar abscess → CN IX (Jacobson's nerve in middle ear shares CN IX origin)
- Carcinoma of tongue base, tonsil, or larynx → CN IX, X (serious — referred otalgia without primary ear disease in an adult smoker is carcinoma until proven otherwise)
- Oesophageal disease → CN X
- Cervical spondylosis → C2/C3
Eustachian Tube Dysfunction — Anatomical Basis
The Eustachian tube's shorter, more horizontal anatomy in children explains why otitis media with effusion (OME, 'glue ear') is predominantly a childhood disease. Nasopharyngeal adenoid hypertrophy blocks the Eustachian tube orifices, exacerbating middle ear ventilation failure. Adults who develop new unilateral OME must be examined for a nasopharyngeal mass at the Eustachian tube orifice — nasopharyngeal carcinoma classically presents this way.
Investigations
- Pure-tone audiometry (PTA): tests air conduction and bone conduction at 250–8000 Hz; distinguishes conductive (air-bone gap) from sensorineural (no gap, both elevated) hearing loss.
- Tympanometry: measures TM compliance at different air pressures; Type A (normal) vs Type B (flat — middle ear effusion or perforation) vs Type C (negative pressure — Eustachian dysfunction).
- CT scan of temporal bone: high-resolution CT delineates bony erosion (cholesteatoma), semicircular canal dehiscence, and middle ear anatomy before surgery.
- MRI of head/neck: soft tissue characterisation of pharyngeal/laryngeal masses, parapharyngeal space lesions, perineural spread.
- Indirect laryngoscopy / flexible nasendoscopy: direct visualisation of the nasopharynx, laryngopharynx, and vocal cords — the cornerstone of ENT examination of the upper airway.
SELF-CHECK
A 45-year-old male smoker presents with a 3-month history of right-sided earache with no visible abnormality in either ear on otoscopy, and no hearing loss. He is a heavy tobacco user. What is the most important next investigation?
A. Pure-tone audiometry to test for SNHL
B. CT scan of the temporal bone
C. Thorough examination of the oral cavity, oropharynx, and laryngopharynx, plus nasendoscopy
D. Tympanometry to check Eustachian tube function
Reveal Answer
Answer: C. Thorough examination of the oral cavity, oropharynx, and laryngopharynx, plus nasendoscopy
Referred otalgia without primary ear pathology in an adult smoker is head and neck malignancy until proven otherwise. The most important causes of referred otalgia are tongue base carcinoma, tonsil carcinoma, and hypopharyngeal/laryngeal carcinoma — all in the distribution of CN IX and CN X. The immediate priority is a full examination of the mouth, oropharynx, and laryngopharynx (including nasendoscopy) to look for the primary malignancy. Delay in diagnosis of head and neck cancer significantly worsens prognosis. Audiometry/tympanometry and CT temporal bone may follow but do not take priority over identifying the primary lesion.
CLINICAL PEARL
The clinical pearl for ENT anatomy is: every neck lump needs a level, and every level tells you where to look for the primary. Level II cervical lymphadenopathy → examine the oropharynx (tonsil, tongue base, posterior pharyngeal wall) and nasopharynx. Level IV → look at the larynx, hypopharynx, and thyroid. Level VI (pretracheal) → examine the thyroid. This anatomical-level-to-primary mapping is not just academic — it is the algorithm for working up a neck lump in a final-year student's OSCE and in your surgical career. Equally: a student who knows only that 'Kiesselbach's plexus is on the anterior nasal septum' but cannot draw the five contributing arteries is unprepared for a vascular epistaxis. Know the anatomy in functional terms, not as isolated facts.