Page 7 of 15
EN1.2 | Pathophysiology of Common ENT Disorders — SDL Guide (Part 2)
Otosclerosis: Pathophysiology and Hearing Impact
Otosclerosis is a disease of the otic capsule — the bony shell of the inner ear derived from enchondral bone — in which localised patches of abnormal spongy vascular bone replace the normal dense enchondral bone. This process, sometimes called otospongiosis (a more anatomically accurate term, referring to the spongy new bone before it re-scleroses), occurs in the temporal bone of the otic capsule and creates clinical disease primarily through its effect on the stapes footplate.
Pathophysiology
The most clinically significant site is immediately anterior to the oval window, at the fissula ante fenestram — a small gap in the otic capsule at the anterior margin of the oval window. When abnormal vascular spongy bone replaces the dense enchondral bone here, it encroaches on and ultimately fixes the stapes footplate to the oval window margins, preventing the footplate from vibrating freely. This is stapedial otosclerosis, and its mechanical consequence is clear: the entire ossicular chain — malleus, incus, and stapes — is now a rigid connected system, with the stapes footplate fixed in the oval window. Sound energy that would normally be transmitted as a pressure wave into the perilymph via stapes footplate movement is instead reflected back — producing a conductive hearing loss that is progressive over years to decades.
A characteristic audiometric finding in otosclerosis is the Carhart notch — a dip in bone conduction thresholds at 2000 Hz on the audiogram. Importantly, the Carhart notch is a mechanical artefact of stapes fixation on bone conduction testing (the stapes normally contributes to bone conduction via its inertial mass vibration), not a true sensorineural loss — it typically reverses after successful stapedectomy. It should not be misinterpreted as cochlear damage.
In a less common variant, cochlear otosclerosis, the abnormal bone remodelling affects the cochlear endosteum and disrupts the blood supply to the spiral ligament and stria vascularis, producing a sensorineural hearing loss (SNHL) component. Cochlear otosclerosis may occur independently or superimposed on stapedial disease.
Demographics and predisposing factors:
Otosclerosis has a distinctive epidemiological profile that reflects its genetic and hormonal basis:
- Autosomal dominant inheritance with 50% penetrance (meaning many carriers are asymptomatic); positive family history in approximately 25% of cases.
- Caucasians predominantly affected; rare in Blacks and Asians.
- Female predominance (F:M approximately 2:1) — oestrogen is thought to stimulate abnormal bone remodelling; pregnancy frequently accelerates hearing loss, and hormonal contraceptives have historically been cautioned.
- Bilateral in approximately 70–80% of cases, though the two ears are often asymmetrically affected.
- Onset typically in the second to fourth decades of life — a young adult with bilateral progressive conductive hearing loss and a normal-looking tympanic membrane (no perforation, no otoscopy abnormality) is otosclerosis until proven otherwise.
- Tympanometry: typically shows a Type As (reduced compliance/'shallow') pattern on tympanogram — the stapes fixation reduces the compliance of the TM/ossicular system, producing a low-amplitude flat peak. Stapedius reflex is absent (the fixed stapes cannot move to tighten the chain).
Adenotonsillitis: Acute, Recurrent, and Complications
The palatine tonsils are part of Waldeyer's ring — the first immunological checkpoint against inhaled and ingested pathogens. Their position at the oropharyngeal junction exposes them to an enormous antigen load, and tonsillar inflammation is the clinical expression of this exposure when the immune response produces tissue damage rather than protection. Understanding the difference between normal tonsillar immunological activity and pathological tonsillar hypertrophy/infection is the key to appropriate management.
Aetiology of Acute Tonsillitis
Approximately 70% of acute tonsillitis episodes in adults and older children are viral — the commonest agents being rhinovirus, coronavirus, adenovirus, and, importantly, Epstein-Barr virus (EBV/infectious mononucleosis), which produces severe exudative tonsillitis with marked cervical lymphadenopathy, splenomegaly, and atypical lymphocytes on the blood film. EBV tonsillitis is a critical differential from bacterial tonsillitis — prescribing amoxicillin in EBV mononucleosis causes a drug-induced maculopapular rash in approximately 90% of patients, a dangerous misdiagnosis trap.
Approximately 30% are bacterial, with Group A beta-haemolytic Streptococcus (Streptococcus pyogenes, GABHS) as the dominant pathogen. GABHS tonsillitis has distinctive features: fever >38.5°C, tonsillar exudate, absence of cough, anterior cervical lymphadenopathy (Centor criteria — higher score = higher probability of GABHS). The clinical importance of GABHS identification is twofold: (1) it responds to penicillin and will not clear spontaneously as reliably as viral tonsillitis; (2) inadequately treated GABHS tonsillitis risks the immunological complications of acute rheumatic fever (ARF) and post-streptococcal glomerulonephritis (PSGN). ARF follows a molecular mimicry mechanism: streptococcal M-protein epitopes cross-react with cardiac valve proteins (particularly mitral and aortic valves), myocardium, and joint synovium — the basis of rheumatic carditis and rheumatic valvular disease. This complication is still clinically relevant in lower-income settings in India.
Pathological progression of tonsillitis:
Acute follicular/lacunar tonsillitis (pus in the tonsillar crypts → white/yellow follicles on the tonsillar surface) → peritonsillar cellulitis (spread beyond the tonsillar capsule into the peritonsillar space) → peritonsillar abscess (quinsy) (pus accumulates between the tonsillar capsule and the superior constrictor muscle, pushing the tonsil medially and downward, and displacing the uvula to the contralateral side). Quinsy produces: severe unilateral throat pain, trismus (jaw stiffness from medial pterygoid muscle irritation), 'hot potato' muffled voice, drooling, inability to swallow, and the contralateral uvular deviation sign. Management: immediate incision and drainage (or aspiration) of the abscess, IV hydration and antibiotics, followed by interval tonsillectomy 6 weeks later.
Deep space spread of tonsillar infection:
If peritonsillar abscess ruptures or is inadequately drained, pus can track into adjacent deep neck spaces:
- → Parapharyngeal space: neck swelling, CN IX/X/XI/XII involvement, carotid artery involvement (rare — internal carotid pseudoaneurysm from erosion by Lemierre's syndrome, septic thrombophlebitis of the internal jugular vein).
- → Retropharyngeal space → Danger space → Mediastinum: descending necrotising mediastinitis — a life-threatening emergency with mortality of 20–50% even with treatment.
Indications for tonsillectomy (recurrent tonsillitis):
The Paradise criteria (widely referenced): ≥7 documented episodes in 1 year, or ≥5 per year for 2 years, or ≥3 per year for 3 years, each meeting one of: temperature >38.3°C, cervical lymphadenopathy, tonsillar exudate, or positive GABHS culture. In Indian practice, these thresholds are used as a guide; compliance documentation and shared decision-making are also factored in.
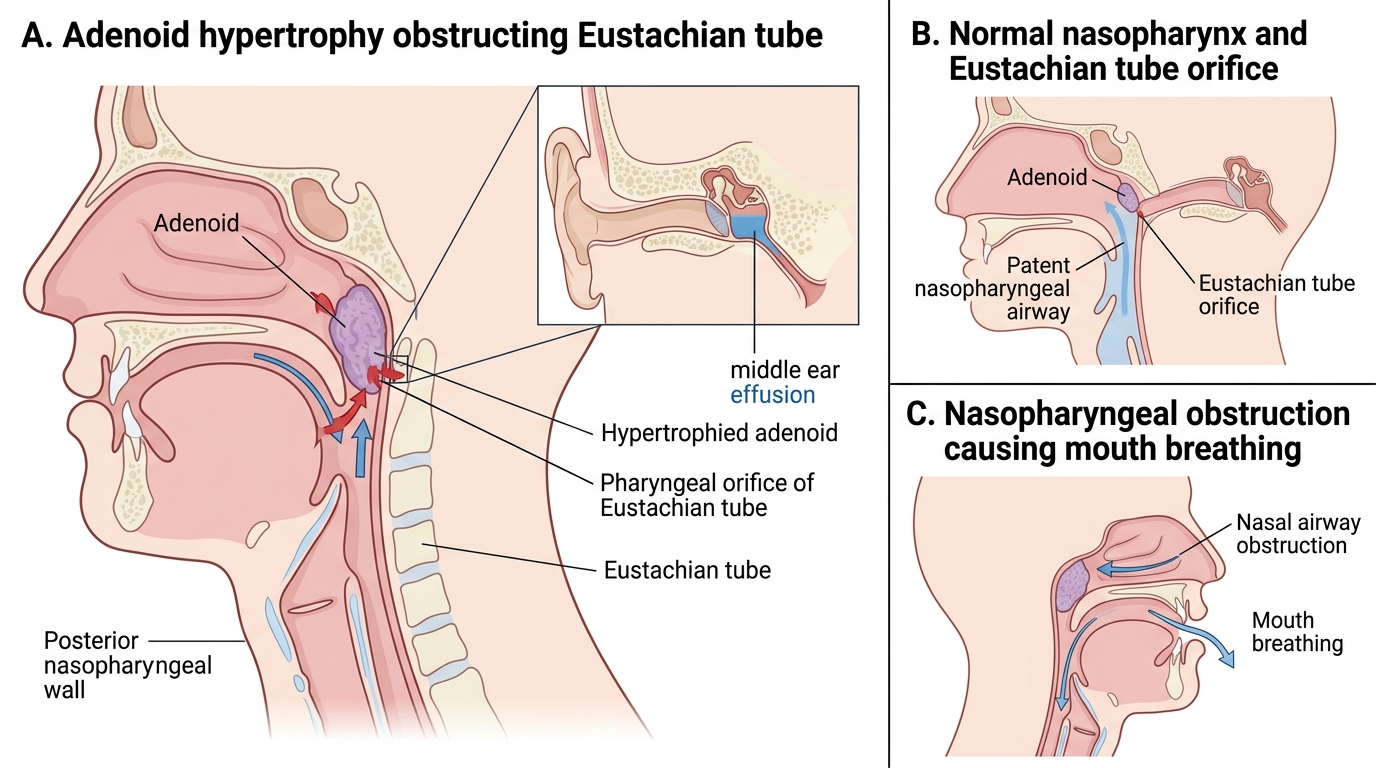
Adenoid Hypertrophy: Pathophysiology and Sequelae
The adenoid (pharyngeal tonsil) is the third and often overlooked component of Waldeyer's ring. It sits on the roof and posterior wall of the nasopharynx, where it directly flanks the Eustachian tube orifices. This anatomical proximity is what makes adenoid hypertrophy so consequential in children — it is not just an obstructing mass in the nasopharynx, but a potential cause of both airway obstruction and middle ear disease through Eustachian tube obstruction.
Adenoid lymphoid tissue is physiologically prominent from birth, grows with antigenic stimulation throughout childhood, peaks at approximately 3–7 years of age, and then progressively involutes during adolescence. Pathological adenoid hypertrophy — hypertrophy that persists or continues growing beyond the physiological involution phase — is driven by chronic infection (adenoiditis) and, in some children, allergic inflammation. When the adenoid mass is large enough to obstruct the Eustachian tube orifices, the Eustachian tube cannot perform its pressure-equalising function. Negative middle ear pressure develops, the TM retracts, and a viscous mucinous fluid (driven by chronic mucosal transudate + goblet cell secretion) accumulates in the middle ear — producing otitis media with effusion (OME, glue ear). OME causes a conductive hearing loss typically in the 15–30 dB range, which in children during the critical period for language acquisition (under 5 years) can impair speech and language development.
Consequences of adenoid hypertrophy — a cascade from a single anatomical site:
1. Nasopharyngeal airway obstruction: mouth breathing (constant, not only when the nose is blocked), snoring, hyponasal voice (loss of nasal resonance → 'blocked nose' quality of voice), and in severe cases, obstructive sleep apnoea (OSA) — with arousal-fragmented sleep, daytime somnolence, behavioural problems, and in very severe/chronic cases, pulmonary hypertension from repeated hypoxaemia.
2. Eustachian tube obstruction → OME → conductive hearing loss.
3. Descending infections: chronic adenoiditis serves as a bacterial reservoir (Haemophilus influenzae, Streptococcus pneumoniae, Moraxella) that seeds descending episodes of sinusitis and AOM.
4. Adenoidal facies: the characteristic facial appearance of a child with chronic mouth breathing — open mouth, elongated face, narrow maxillary arch, dental crowding, and hypoplastic nasal bones — from the loss of nasal airflow pressure on facial bone development.
Management: adenoidectomy is indicated for OME with hearing loss (often with simultaneous grommet insertion), symptomatic OSA, or recurrent adenoiditis. Adenoidectomy alone or with grommets is the definitive treatment; recurrence of adenoid tissue is uncommon in adolescents.
Adenoid Hypertrophy: Ear and Airway Effects