Page 13 of 20
EN4.46 | HIV Manifestations in ENT — SDL Guide (Part 2)
Investigations
Investigation of ENT manifestations in HIV is best understood as two-layered: systemic investigations that quantify the degree of immunosuppression and establish or confirm the HIV diagnosis, and local investigations targeted to the specific ENT manifestation in question. These two layers are complementary and must both be pursued — neither alone is sufficient. The CD4 count tells you the immunological context and expands or narrows the differential diagnosis dramatically: a CD4 count of 450 with oral candidiasis means moderate immunosuppression and a relatively limited differential, whereas a CD4 count of 40 with a neck mass could be lymphoma, tuberculosis, atypical mycobacterial infection, or Kaposi's sarcoma — all requiring different investigations and treatments. Local investigations then provide the specific tissue-level diagnosis that the systemic picture alone cannot give. The hierarchy below runs from the most broadly informative to the most targeted.
Systemic HIV investigations:
- HIV serology (ELISA + Western blot / fourth-generation antigen-antibody combination assay): to confirm HIV diagnosis in undiagnosed patients; rapid point-of-care tests are available.
- CD4 count: provides immunological staging and guides the differential diagnosis of ENT manifestations. CD4 >500 = minimal immune compromise; CD4 200–500 = moderate; CD4 <200 = severe/AIDS-defining range.
- Plasma HIV viral load (copies/mL): monitors treatment response; undetectable viral load on ART indicates good virological control.
- Full blood count: anaemia (of chronic disease), lymphopenia (characteristic of HIV), thrombocytopenia.
Investigations for specific ENT manifestations:
- Oral candidiasis: primarily a clinical diagnosis; potassium hydroxide (KOH) mount of scrapings shows pseudohyphae/spores; culture if treatment-refractory (to detect fluconazole-resistant species, e.g. C. glabrata, C. krusei).
- Suspected Kaposi's sarcoma: biopsy of the lesion is required for definitive diagnosis — histology shows spindle cells, slit-like vascular spaces, haemosiderin deposits, and HHV-8 positivity on immunohistochemistry. Clinical appearance is sufficient to start treatment in many centres, but biopsy confirms.
- Neck lymphadenopathy: FNA cytology (FNAC) to assess for reactive vs lymphoma vs KS vs tuberculosis (common co-infection in India). Excisional biopsy if FNAC inconclusive or lymphoma suspected.
- Sinusitis: CT paranasal sinuses for extent and bone erosion; fungal culture of sinus aspirate if fungal sinusitis suspected; nasal endoscopy.
- Hearing loss: pure-tone audiometry and tympanometry; audiological assessment for type and degree of hearing loss; MRI brain if sensorineural loss + neurological symptoms (CMV, cryptococcal meningitis).
Diagnosis: Recognising HIV-Related ENT Conditions
The diagnostic challenge in HIV ENT practice is twofold: recognising the HIV-related condition itself and distinguishing it from the range of non-HIV mimics that can produce identical-appearing lesions. Both errors are clinically costly — failing to recognise Kaposi's sarcoma on the palate as HIV-related delays diagnosis; mistaking oral candidiasis in a patient with dentures for HIV-related thrush leads to unnecessary investigation and patient distress. The framework below is structured around the clinical findings rather than the diagnoses — so that when you encounter a patient with a white oral lesion, or a violaceous palatal patch, or bilateral parotid swellings, you have an organised differential to work through rather than needing to recall lists of diseases. The approach to each finding proceeds through three questions: What does it look like? Can it be wiped off? What is the CD4 context?
Provided image
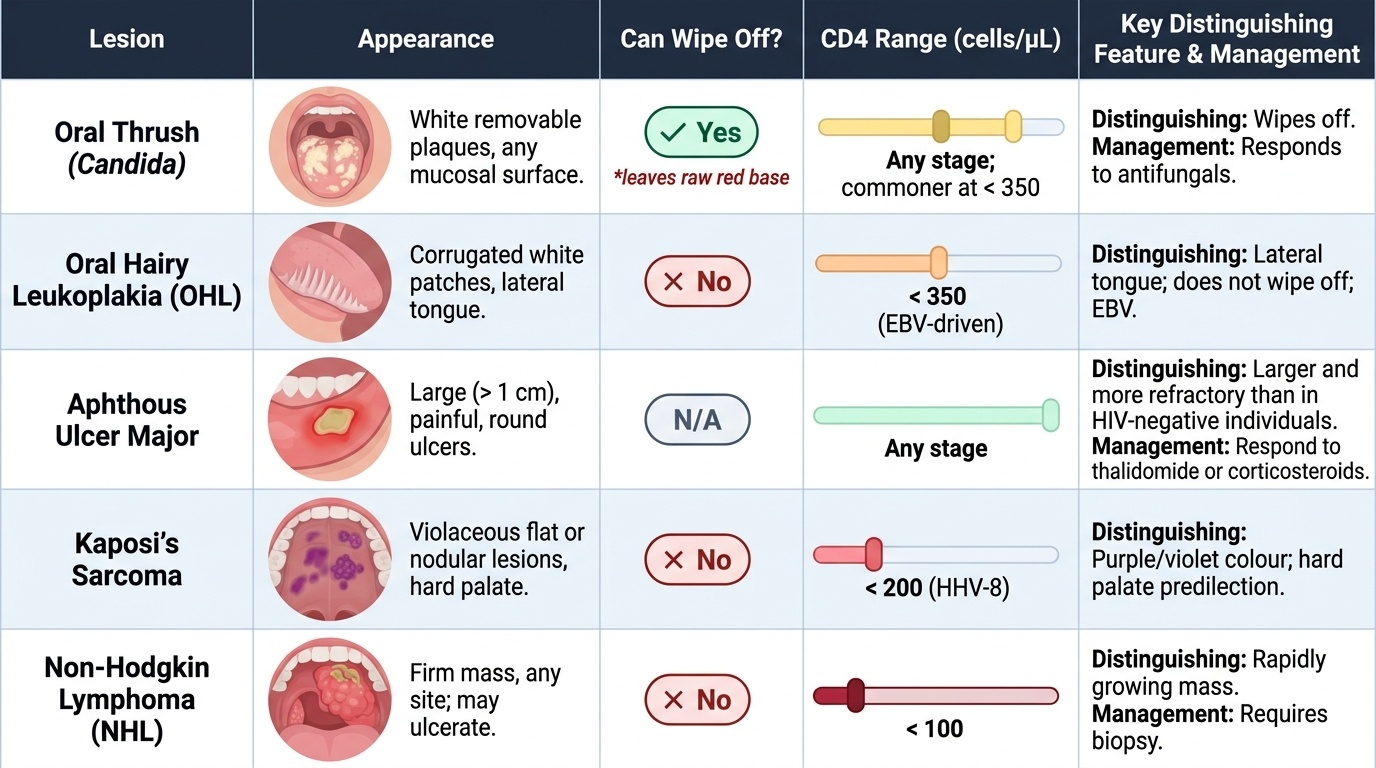
Oral lesions — the key differentials:
The four most important oral lesions to distinguish are oral candidiasis, oral hairy leukoplakia, Kaposi's sarcoma, and non-Hodgkin lymphoma. The table below summarises the distinguishing features:
| Lesion | Appearance | Can wipe off? | CD4 association | Key distinguishing feature |
|---|---|---|---|---|
| Oral thrush (candida) | White removable plaques, any mucosal surface | Yes (leaves raw red base) | Any; commoner <350 | Wipes off; responds to antifungals |
| Oral hairy leukoplakia | Corrugated white, lateral tongue | No | <350 (EBV-driven) | Lateral tongue; does not wipe off; EBV |
| Kaposi's sarcoma | Violaceous flat/nodular, hard palate | No | <200 (HHV-8) | Purple/violet colour; hard palate predilection |
| NHL (B-cell lymphoma) | Firm mass, any site; may ulcerate | No | <100 | Rapidly growing mass; requires biopsy |
| Major aphthous ulcers | Large (>1 cm), painful, round ulcers | N/A | Any stage | Larger and more refractory than in HIV-negative; respond to thalidomide or corticosteroids |
Neck masses — differential diagnosis:
Cervical lymphadenopathy in HIV-positive patients has a wide differential: persistent generalised lymphadenopathy (PGL — reactive, symmetrical, non-tender), tuberculosis lymphadenitis (commonest cause of cervical lymphadenopathy in India, regardless of HIV status — matted, tender, may collar-stud), NHL (asymmetric, rapidly growing, firm), Kaposi's sarcoma involving nodes, and Mycobacterium avium complex (MAC) lymphadenitis at very low CD4 counts. FNAC is the first investigation; excisional biopsy if needed.
Parotid swellings:
Bilateral soft fluctuant parotid swellings in an HIV-positive patient = HIV-associated lymphoepithelial cysts (HALE cysts) — benign, managed conservatively; CT or MRI shows bilateral intraparotid cystic collections.
SELF-CHECK
A 40-year-old HIV-positive man on antiretroviral therapy with a CD4 count of 85 cells/μL presents with bilateral parotid gland swellings that are soft and fluctuant. He has no pain or facial nerve weakness. CT shows bilateral intraparotid cystic collections with preserved parotid parenchyma. The most likely diagnosis and management are:
A. Bilateral pleomorphic adenoma; bilateral superficial parotidectomy
B. Bilateral Warthin's tumour; conservative observation or surgical excision
C. HIV-associated lymphoepithelial cysts; conservative management (treat the underlying HIV with ART)
D. Bilateral parotid abscesses; IV antibiotics and surgical drainage
Reveal Answer
Answer: C. HIV-associated lymphoepithelial cysts; conservative management (treat the underlying HIV with ART)
Bilateral soft fluctuant parotid swellings with intraparotid cystic collections on CT in an HIV-positive patient with low CD4 are the classic presentation of HIV-associated lymphoepithelial cysts (HALE cysts). The mechanism is intraglandular lymphoid hyperplasia with cystic change — a benign reactive process related to HIV-driven lymphoid activation within the parotid's intraglandular lymph nodes. Management is conservative: the swellings often regress with effective antiretroviral therapy as CD4 count recovers. Parotidectomy is not indicated for a benign reactive condition. Pleomorphic adenoma is usually unilateral, solid, and not associated with HIV. Warthin's tumour is bilateral in 10% but occurs in older, typically male smokers, not young HIV-positive patients with low CD4 counts.
CLINICAL PEARL
Oral hairy leukoplakia is pathognomonic of significant immunosuppression — it is not seen in immunocompetent individuals (unlike oral candidiasis, which can occur on broad-spectrum antibiotics or in diabetics). If you see it, the patient either has HIV, is on long-term immunosuppressants, or has another cause of cellular immune deficiency. The lateral tongue location and the inability to wipe it off are the two findings that clinch the diagnosis at the bedside. No biopsy is needed if the clinical picture is classic. Its presence in a patient not known to have HIV is an absolute indication to offer HIV testing.
Principles of Management of ENT Manifestations in HIV
The overarching principle of managing ENT manifestations in HIV is that antiretroviral therapy (ART) is the most important intervention for the majority of ENT manifestations — immune reconstitution through ART causes many mucosal and lymphoid manifestations to regress, reduces the susceptibility to opportunistic infections, and is the only intervention that addresses the root cause. Specific treatments are required for each manifestation, but they must be integrated with the systemic HIV management.
Oral candidiasis:
First-line treatment is topical antifungal therapy for mild/limited disease: nystatin oral suspension or miconazole oromucosal gel. For moderate or extensive oral candidiasis, or for oropharyngeal candidiasis extending into the oesophagus (odynophagia + dysphagia = oesophageal candidiasis), systemic fluconazole (oral or IV) is the first-line agent. Secondary prophylaxis (long-term fluconazole) may be required in patients with frequent recurrences and very low CD4 counts, though this risks the emergence of fluconazole-resistant Candida species.
Oral hairy leukoplakia:
OHL itself does not require specific treatment in most cases — it is a benign EBV-driven mucosal change that regresses with effective ART and immune recovery. High-dose oral acyclovir or valacyclovir can suppress EBV and temporarily reduce OHL lesions, but relapse is universal when antiviral therapy stops. The main clinical significance of OHL is as a marker of immunosuppression, prompting ART initiation or optimisation.
Kaposi's sarcoma of the head and neck:
For limited mucosal KS (small lesions in the oral cavity), local therapies are used: intralesional vinblastine injection, laser therapy, or cryotherapy. ART itself can induce KS regression in early disease. For extensive or symptomatic KS (large oral lesions causing dysphagia, laryngeal KS causing airway compromise), systemic chemotherapy (liposomal doxorubicin, paclitaxel) is required. ENT surgeon's role: biopsy for diagnosis, laser debulking for airway-threatening lesions, tracheostomy if laryngeal KS obstructs the airway.
Recurrent sinusitis:
For bacterial sinusitis, standard antibiotics (amoxicillin-clavulanate) with prolonged courses (3–4 weeks rather than standard 7–10 days). Nasal saline irrigation, intranasal corticosteroids. Functional endoscopic sinus surgery (FESS) for chronic refractory cases or when anatomical obstruction is demonstrated. For fungal sinusitis (Aspergillus, mucormycosis) — IV voriconazole or amphotericin B; aggressive surgical debridement.
Non-Hodgkin lymphoma:
Requires multidisciplinary management — haematology/oncology, ENT for biopsy and airway management. Systemic chemotherapy (R-CHOP regimen — rituximab, cyclophosphamide, doxorubicin, vincristine, prednisolone) is the backbone. ART is continued alongside chemotherapy.
Hearing loss:
Conductive hearing loss from recurrent OM: standard management (grommets, adenoidectomy). Ototoxic drug avoidance where possible; monitoring audiograms in patients receiving aminoglycosides. Sensorineural loss: hearing aids; cochlear implant assessment in selected cases.
| Manifestation | First-line treatment | Role of ART |
|---|---|---|
| Oral candidiasis | Fluconazole (systemic for mod-severe) | Immune recovery reduces frequency |
| Oral hairy leukoplakia | Observation; ART | OHL regresses with immune recovery |
| Kaposi's sarcoma (limited) | Intralesional vinblastine / laser | ART induces regression in early KS |
| Kaposi's sarcoma (extensive) | Systemic chemotherapy | Continued alongside chemotherapy |
| Recurrent sinusitis | Prolonged antibiotics; FESS if refractory | Reduces susceptibility |
| NHL | R-CHOP chemotherapy | ART continued |
| Lymphoepithelial cysts | Conservative | Often regress with ART |