Page 4 of 20
EN4.41 | Benign Inflammatory Paralytic Laryngeal Disorders — SDL Guide
Learning Objectives
- Describe the clinical features, laryngoscopic appearances and pathophysiology of the major benign structural lesions of the larynx
- Describe the clinical features, investigations and management of acute and chronic inflammatory conditions of the larynx, including recognition of airway emergencies
- Describe the clinical features, causes and principles of management of laryngeal paralysis
INSTRUCTIONS
The larynx is exposed to mechanical stress, infectious agents, chemical irritants and neurological insults — all of which can produce disease ranging from the trivially self-limiting to the immediately life-threatening. This SDL covers the three main categories of non-malignant laryngeal disease: benign structural lesions (nodules, polyps, Reinke's oedema, granuloma, papilloma), inflammatory conditions (acute laryngitis, epiglottitis, croup, chronic laryngitis, diphtheria), and laryngeal paralysis. Each category requires a distinct diagnostic approach and management strategy, and the skill of clinical differentiation is what separates safe, effective practice from dangerous mismanagement.
References
- Dhingra PL, Dhingra S — Diseases of Ear, Nose and Throat and Head and Neck Surgery, 8th ed., Ch. 64-70 (textbook)
- Hazarika P, Nayak DR — Textbook of ENT and Head and Neck Surgery, 3rd ed., Ch. 40-46 (textbook)
- Gleeson M et al — Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Vol 2, Larynx and inflammatory disease chapters (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients arrive at your ENT OPD on the same morning. The first is a 32-year-old schoolteacher with three months of worsening hoarseness; she has no risk factors for malignancy. The second is a 4-year-old boy brought in by his mother because of a barking cough and noisy breathing that worsened after midnight. Both patients have 'throat problems' — but the urgency, investigation and management could not be more different. The first requires a clinic-based laryngoscopy and a discussion of voice therapy. The second needs an immediate assessment of airway patency, a lateral neck X-ray, and potentially an anaesthetist on standby. How do you rapidly distinguish the benign from the emergency? And what single finding on the neck X-ray would change everything?
WHY THIS MATTERS
Benign laryngeal diseases — structural lesions, inflammatory conditions, and paralytic disorders — together constitute the vast majority of laryngeal pathology encountered in ENT practice. Vocal cord nodules alone account for a substantial proportion of occupational voice disorders among India's enormous population of teachers, public speakers, and call-centre workers. Laryngeal papilloma, though benign, is notorious for multiple recurrences that may require dozens of operative procedures over a patient's lifetime. At the other extreme, acute epiglottitis and diphtheria — while less common since vaccination programmes — remain life-threatening laryngeal emergencies where a delay of minutes can result in complete airway obstruction and death. The EN4.41 competency bridges this range deliberately: a graduating MBBS must be able to recognise a benign benign vocal fold lesion, counsel a patient appropriately, AND recognise an airway emergency and initiate correct immediate management — including not performing a throat examination when epiglottitis is suspected.
RECALL
This SDL builds on the laryngeal anatomy and vocal cord physiology covered in the Hoarseness of Voice SDL (EN4.40). Recall: the true vocal cords lie at the glottic level; the supraglottis includes the epiglottis, aryepiglottic folds, and false cords; and the subglottis is the region below the cords to the lower border of the cricoid. This anatomical stratification is clinically critical: supraglottic swelling (as in epiglottitis) produces a different airway threat from subglottic swelling (as in croup), because the supraglottis is a larger cavity and swelling here tends to present earlier with muffled voice and drooling before actual obstruction, whereas subglottic swelling produces the characteristic 'steeple sign' narrowing visible on X-ray and the characteristic 'barking cough' and 'inspiratory stridor' pattern of croup. Recall also the layers of the vocal fold including Reinke's space — the loose subepithelial connective tissue whose oedema leads to Reinke's oedema — and the posterior cricoarytenoid as the sole abductor, whose paralysis in bilateral cord palsy creates an airway emergency.
Clinical Presentation: A Wide Spectrum of Laryngeal Disease
The non-malignant laryngeal diseases covered in this SDL share a common symptom — voice change or airway compromise — but their clinical contexts, speeds of onset, and urgency levels span an enormous range. Recognising where on this spectrum a patient sits is the first and most important clinical judgement.
At one end of the spectrum is the patient with a chronic, slowly progressive change in voice quality — a teacher whose voice has been 'getting rougher' over years, or a smoker with a persistently low-pitched 'gravelly' voice. These patients require careful laryngoscopy, possibly a biopsy, and a measured management plan — but they are not emergencies.
At the other end is the patient — most commonly a child — presenting acutely with stridor: the harsh, musical, usually inspiratory noise produced when the airway is narrowed to the point where airflow becomes turbulent. Stridor is always a sign of partial airway obstruction and always demands immediate assessment. The clinician's job is to determine the site and severity of obstruction, establish whether the airway is deteriorating, and institute the correct emergency management — which may include not performing an oral examination at all (for suspected epiglottitis) or preparing for intubation.
Between these poles lie patients with acute laryngitis (common, self-limiting, rarely requiring intervention), chronic laryngitis (benign but requiring vigilance for dysplasia), vocal cord granuloma (recurrent and frustrating), and laryngeal papilloma (benign but surgically demanding). The presentation of each is sufficiently distinct that a careful history of onset, duration, age of patient, associated symptoms and immunisation status narrows the differential considerably before any instrument is used.
Benign Structural Lesions of the Larynx
Benign structural lesions of the larynx arise from mechanical trauma to the vocal fold mucosa, viral infection, or chronic irritation. Each has a characteristic site, macroscopic appearance, and clinical context.
Vocal cord nodules (discussed in detail in EN4.40) arise from repetitive phonatory microtrauma at the point of maximum vibratory amplitude — the junction of the anterior one-third and posterior two-thirds of the cord. The repeated shear force causes epithelial thickening and subepithelial fibrous change, producing bilateral, symmetric, white nodular thickenings. They are the hallmark injury of professional voice users and are definitively managed with voice therapy before considering surgery.
Vocal cord polyp differs from nodules in being typically unilateral and arising from a single traumatic event — a burst blood vessel in the superficial lamina propria, usually following an episode of vocal strain (shouting, singing, violent coughing). The resulting haemorrhage or oedema into Reinke's space forms a pedunculated or sessile polyp, red or translucent depending on whether it is haemorrhagic or oedematous. Because it cannot spontaneously resolve, microlaryngoscopic excision is the definitive treatment.
Reinke's oedema (polypoid degeneration) is the consequence of chronic smoking and, sometimes, hypothyroidism on the unique structure of Reinke's space. Tobacco smoke increases vascular permeability and induces chronic oedema within the superficial lamina propria; the accumulation of protein-rich fluid causes both vocal folds to become diffusely swollen, giving them a pale, translucent, grape-like appearance. Because both cords are affected along their entire length, the voice is characteristically low-pitched and gravelly — often mistaken by patients for a permanently 'smoker's voice.' Management requires smoking cessation; phonomicrosurgery (cordotomy and evacuation of the oedematous fluid with careful trimming of excess mucosa) is performed when the voice is severely compromised, with the essential caveat that the entire cord must never be stripped.
Contact ulcer and granuloma arise at the posterior vocal process of the arytenoid — NOT at the free edge of the cord. This posterior location distinguishes them from all other benign vocal cord lesions. The posterior vocal process is covered by mucosa stretched directly over cartilage with no Reinke's space; repeated mechanical trauma — from reflux (acid bathing the posterior larynx) or from forceful glottal closure (hard attack onset phonation in habitual throat-clearing) or from endotracheal intubation pressure — erodes this mucosa, creates an ulcer, and triggers a granulomatous repair response. The granuloma is characteristically a pale, smooth, pedunculated or sessile protuberance at the vocal process. Anti-reflux therapy is the primary treatment; surgery has a high recurrence rate and should be avoided unless the granuloma is causing significant airway compromise.
Laryngeal papilloma is the commonest benign laryngeal tumour and is caused by human papillomavirus (HPV) types 6 and 11 — the low-risk, non-oncogenic types (HPV 16 and 18 are the high-risk oncogenic types associated with cervical and oropharyngeal carcinoma; do not confuse them). Papillomas grow as exophytic, warty, pink or white frond-like masses on the vocal cord surface and can cause hoarseness, dyspnoea, and even complete airway obstruction in children. There are two forms: juvenile (recurrent respiratory papillomatosis) — affects young children, acquired by vertical transmission of maternal HPV at birth; tends to regrow aggressively after excision, requiring multiple operations over years; adult-onset papilloma — less aggressive, often solitary, with a higher chance of definitive cure after surgical excision. Treatment is by microlaryngoscopy with CO2 laser or microdebrider; cidofovir injection and bevacizumab have been used as adjuvant therapies for aggressive juvenile disease. Malignant transformation is rare but recognised, particularly with HPV 11 and in adults.
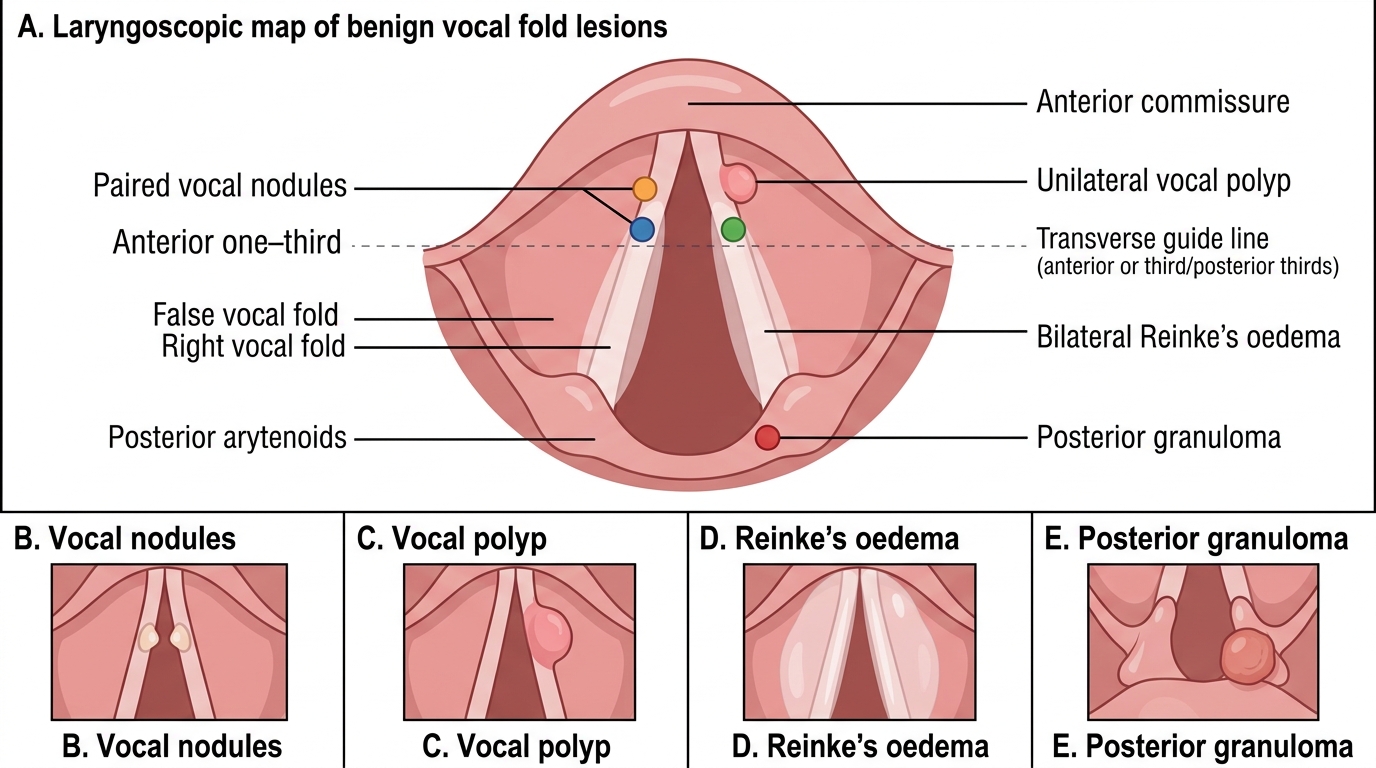
Benign Vocal Fold Lesions: Laryngoscopic Positions
SELF-CHECK
A 7-year-old boy is brought to ENT with progressively worsening hoarseness and intermittent dyspnoea over eight months. His mother had a history of genital warts during pregnancy. On indirect laryngoscopy, multiple frond-like pink masses are seen on both vocal cords. The most likely diagnosis and causative agent are:
A. Laryngeal carcinoma — HPV 16/18
B. Juvenile recurrent respiratory papillomatosis — HPV 6/11
C. Laryngeal diphtheria — Corynebacterium diphtheriae
D. Laryngeal candidiasis — Candida albicans
Reveal Answer
Answer: B. Juvenile recurrent respiratory papillomatosis — HPV 6/11
The clinical picture — a young child with progressive hoarseness and dyspnoea, a maternal history of genital warts (HPV infection), and multiple frond-like papillary masses on both vocal cords — is classic juvenile recurrent respiratory papillomatosis. The causative agents are HPV types 6 and 11 (the low-risk, non-oncogenic types), transmitted vertically from mother to child during delivery through an infected birth canal. HPV 16 and 18 are the high-risk oncogenic types associated with cervical and oropharyngeal carcinoma, not papilloma. Laryngeal carcinoma is exceedingly rare in children. Diphtheria produces a grey pseudomembrane, not papillary fronds. Candida produces white plaques, not frond-like masses.
Inflammatory Conditions of the Larynx
Inflammatory conditions of the larynx range from the extremely common and self-limiting (acute viral laryngitis) to the rare and potentially fatal (diphtheria, acute epiglottitis). The anatomical level of the inflammation within the larynx — supraglottic, glottic, or subglottic — largely determines the clinical presentation and the degree of airway threat.
Acute laryngitis is the most common laryngeal inflammatory condition. It is almost always viral in aetiology (rhinovirus, influenza, parainfluenza, adenovirus) and usually follows an upper respiratory tract infection. The vocal cords become oedematous, hyperaemic, and the mucosal wave is disrupted — producing hoarseness that may be severe ('complete voice loss' is not unusual with viral laryngitis). The condition is self-limiting in 7–14 days. Management is symptomatic: voice rest, steam inhalation, hydration, and analgesics; antibiotics are not indicated for uncomplicated viral laryngitis. Professional voice users (singers before performances) may receive a short course of systemic corticosteroids to reduce cord oedema — a well-recognised 'emergency' use in this context.
Acute epiglottitis is a supraglottic emergency. The epiglottis and surrounding supraglottic structures become cellulitic — in the pre-vaccination era this was almost always caused by Haemophilus influenzae type b (Hib); since the introduction of Hib vaccination in national immunisation programmes, adult cases (from group A streptococcus, S. pneumoniae, S. aureus) have become proportionally more important. The child presents with a high fever, odynophagia, drooling (cannot swallow secretions), a 'hot potato voice' (muffled, not hoarse — supraglottic swelling does not directly affect cord vibration early), and a tripod posture (leaning forward on arms). The lateral neck X-ray shows the pathognomonic 'thumb sign' — the swollen, thumb-shaped epiglottis silhouetted against the air column. The critical rule: do NOT examine the throat in a suspected case of acute epiglottitis in a child. Attempting to visualise the pharynx with a tongue depressor may precipitate complete laryngospasm and airway obstruction. Immediate management is admission, senior anaesthetic presence, controlled induction of anaesthesia, and orotracheal intubation or tracheostomy to secure the airway — THEN intravenous ceftriaxone.
Croup (acute laryngotracheobronchitis) is the most common cause of stridor in children, caused primarily by parainfluenza virus type 1 (occasionally types 2, 3, influenza, RSV). It affects children aged 6 months to 5 years, typically presenting in autumn/winter. The virus infects the subglottic mucosa, which becomes oedematous — and because the subglottis is a rigid ring (the cricoid is the only complete cartilaginous ring), subglottic oedema cannot expand outward; it narrows the airway inward. On the anteroposterior (AP) chest/neck X-ray, this produces the characteristic 'steeple sign' (also called 'pencilling') — a loss of the normal shouldering at the subglottis, with the air column tapering to a narrow central column. The child has a barking, 'croupy' cough, inspiratory stridor (worse at night), and low-grade fever. Unlike epiglottitis, the child is not drooling and can be examined. Management: mild croup = oral dexamethasone (0.15–0.6 mg/kg) and humidified air; moderate-severe croup = nebulised adrenaline (epinephrine) + systemic corticosteroids; intubation if airway is not maintained.
Diphtheria is caused by Corynebacterium diphtheriae, which produces an exotoxin that causes tissue necrosis and the formation of a dense, grey-white pseudomembrane — a tough membrane of fibrin, inflammatory cells and bacteria that adheres tightly to the underlying mucosa and bleeds when forcibly removed. In laryngeal diphtheria, this membrane extends from the pharynx onto the larynx and subglottis, causing progressive airway obstruction. The patient (unvaccinated or incompletely vaccinated) presents with a sore throat, low-grade fever, cervical lymphadenopathy ('bull neck'), and progressive hoarseness. Systemic complications include myocarditis and peripheral neuropathy from toxin spread. Treatment: diphtheria antitoxin (to neutralise circulating toxin), penicillin or erythromycin (to eradicate the organism), and airway management. India still sees diphtheria outbreaks in underimmunised populations.
Chronic laryngitis results from prolonged exposure to irritants — tobacco smoke, alcohol, laryngopharyngeal reflux, occupational dust, or repeated acute episodes. The laryngeal mucosa becomes thickened, erythematous, and irregular; the cords may show leukoplakia (white patches representing hyperkeratosis/dysplasia) — a pre-malignant change that mandates biopsy under microlaryngoscopy. Management requires elimination of the causative irritant (smoking cessation most important), anti-reflux measures, and regular surveillance with biopsy for leukoplakia.
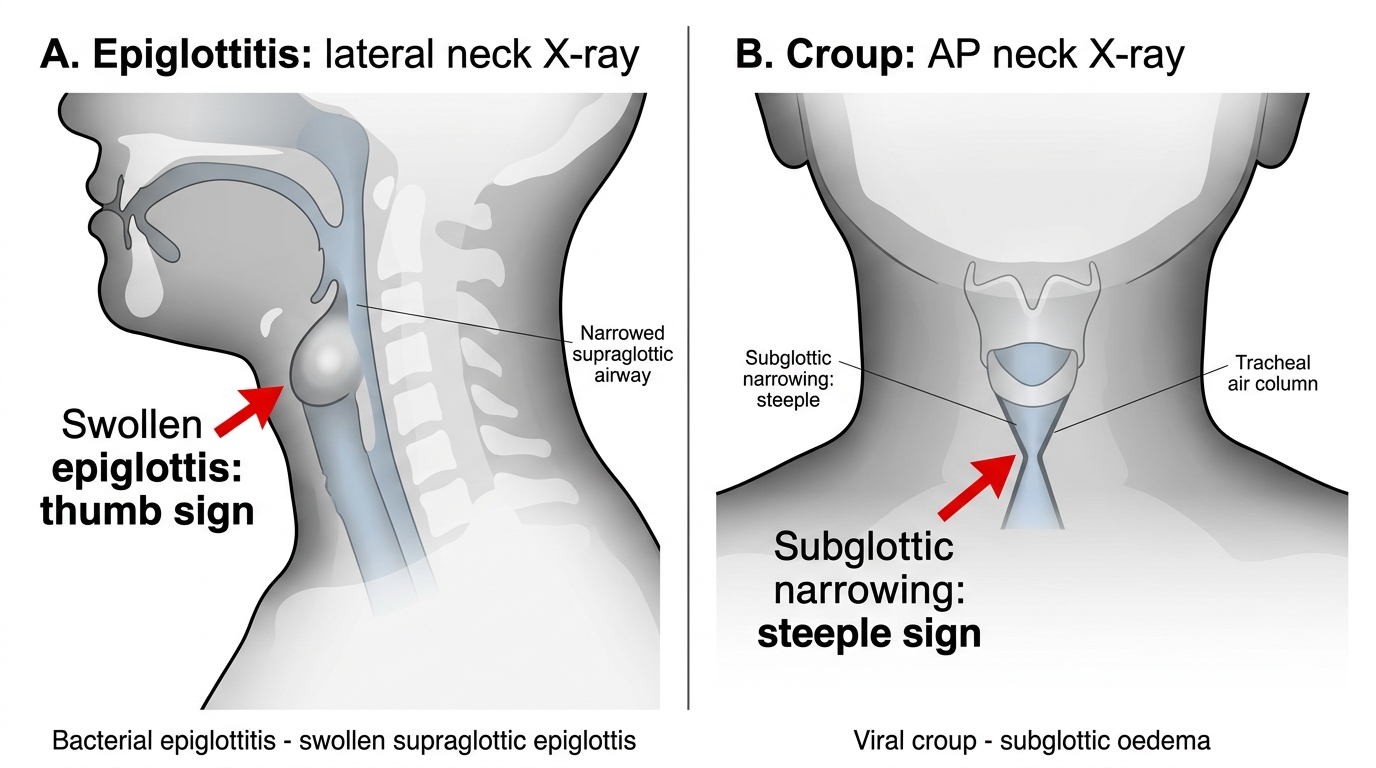
Thumb Sign vs Steeple Sign on Neck X-ray
SELF-CHECK
A 3-year-old child is brought to casualty at 2 AM with a barking cough, inspiratory stridor, and mild respiratory distress. Temperature is 38°C. The child is alert and sitting comfortably. The anteroposterior neck X-ray shows a 'steeple sign.' The most appropriate immediate management is:
A. Urgent oral examination with tongue depressor to assess the epiglottis
B. Oral dexamethasone 0.15 mg/kg and humidified oxygen; reassess in 2 hours
C. Immediate endotracheal intubation under general anaesthesia
D. Intravenous ceftriaxone and admit to HDU
Reveal Answer
Answer: B. Oral dexamethasone 0.15 mg/kg and humidified oxygen; reassess in 2 hours
The clinical picture — a young child (age 3), barking cough, inspiratory stridor worse at night, low-grade fever, alert child sitting comfortably, and 'steeple sign' on AP X-ray — is classic croup (acute laryngotracheobronchitis) due to parainfluenza virus. This is mild-moderate croup. The recommended management is oral dexamethasone (0.15–0.6 mg/kg single dose) which reduces the subglottic oedema and shortens the illness, plus humidified oxygen; nebulised adrenaline is reserved for moderate-severe croup. Oral examination with a tongue depressor is contraindicated in epiglottitis, not in croup — but the 'steeple sign' (subglottic narrowing on AP view) already points to croup, not epiglottitis (which shows the 'thumb sign' on lateral view). Immediate intubation is not required for mild-moderate croup. IV ceftriaxone is appropriate for epiglottitis, not croup.