Page 2 of 20
EN4.40 | Hoarseness of Voice — SDL Guide (Part 2)
Clinical Examination and Investigation of Hoarseness
The clinical examination of a patient with hoarseness has a defined sequence: general assessment, neck examination, and most importantly, laryngoscopic visualisation of the vocal folds. No diagnosis of the cause of hoarseness can be made without visualising the cords.
General assessment begins by listening to the patient's voice before any instrument is used. A rough, gravelly voice suggests a cord lesion; a weak breathy voice suggests cord palsy or large glottic gap; a strained or pressed voice suggests spasmodic dysphonia or muscle tension. Document the patient's maximum phonation time (MPT) — ask the patient to sustain a vowel sound /aaah/ on a comfortable note for as long as possible. Normal MPT is ≥15 seconds for men and ≥12 seconds for women; a MPT below 8 seconds indicates significant glottic incompetence.
Neck examination follows a systematic inspection and palpation: thyroid gland for enlargement or nodules; the trachea for deviation; cervical lymph nodes in all levels (I–VI), with particular attention to level VI (prelaryngeal/pretracheal/paratracheal nodes) and level II–III jugulodigastric nodes for laryngeal malignancy; and the carotid sheath for masses.
Indirect laryngoscopy (IDL) using a laryngeal mirror is the primary and most widely used technique for visualising the larynx. The technique is performed with the patient seated upright, mouth open, tongue protruded and held by gauze. A warmed laryngeal mirror (to prevent fogging) is introduced into the oropharynx at 45°, pressing the uvula and soft palate upward without touching the posterior pharyngeal wall (which triggers the gag reflex). The patient is asked to breathe quietly for the respiratory phase, then to say /eee/ for the phonatory phase. Structures visualised include the epiglottis, aryepiglottic folds, arytenoids, false cords, and — most importantly — the true vocal folds. The examiner assesses cord colour, surface regularity, symmetry of movement, and glottic closure. Cord mobility is assessed during /eee/ (adduction) and quiet breathing (abduction).
Flexible fibre-optic nasolaryngoscopy (FFNL) is increasingly the preferred technique in outpatient ENT because it provides a superior and dynamic view of the larynx, is tolerated with topical anaesthesia only, and can be performed in patients with a brisk gag reflex. A flexible nasolaryngoscope is passed through the anaesthetised nasal cavity, and the larynx is viewed in real time during phonation, swallowing, coughing, and valsalva manoeuvres. FFNL is the gold standard for dynamic assessment of vocal cord movement, enabling detection of subtle mobility asymmetry missed by IDL.
Investigations are selected based on examination findings:
- All patients with hoarseness >3 weeks: laryngoscopy (IDL or FFNL) is mandatory and constitutes the primary investigation.
- Suspected vocal cord palsy: CT chest (neck to diaphragm) to image the course of the left RLN; if bilateral palsy, add CT/MRI brain and neck. Thyroid function tests and thyroid ultrasound if thyroid disease is suspected.
- Suspected malignancy: contrast CT of the larynx, neck and chest for staging (assesses cartilage invasion, cord fixation, nodal disease, pulmonary metastases). Direct laryngoscopy under general anaesthesia with biopsy (microlaryngoscopy) is required to confirm histology — the definitive diagnostic investigation for laryngeal carcinoma.
- Benign vocal cord lesions: laryngostroboscopy (stroboscopic light source during laryngoscopy) provides a slow-motion view of the mucosal wave, differentiating functionally significant lesions from incidental findings.
- Voice analysis: computerised acoustic analysis (fundamental frequency, jitter, shimmer, harmonic-to-noise ratio) and aerodynamic studies (MPT, phonatory airflow) provide objective documentation of voice quality and are used in research and for monitoring response to treatment.
SELF-CHECK
On indirect laryngoscopy in a patient with chronic hoarseness, you see bilateral small whitish thickenings at the junction of the anterior one-third and posterior two-thirds of both vocal cords. The patient is a 35-year-old female school teacher with no smoking history. The most likely diagnosis and appropriate first-line management are:
A. Bilateral vocal cord carcinoma — urgent microlaryngoscopy and biopsy
B. Vocal cord nodules — voice therapy and vocal hygiene education for 3–6 months before considering surgery
C. Reinke's oedema — cessation of smoking and corticosteroids
D. Vocal cord polyps — immediate microlaryngoscopy and polypectomy
Reveal Answer
Answer: B. Vocal cord nodules — voice therapy and vocal hygiene education for 3–6 months before considering surgery
Bilateral, symmetric, whitish fibrous thickenings at the junction of the anterior one-third and posterior two-thirds of the vocal cords in a professional voice user without risk factors for malignancy is the classic appearance of vocal cord nodules (singer's nodules / teacher's nodules). These are caused by repeated mechanical trauma at the point of maximum vibratory amplitude. The first-line treatment is voice therapy (vocal hygiene, breathing technique, resonance therapy) for 3–6 months — the majority of nodules resolve with voice therapy alone. Surgery (microlaryngoscopic excision) is reserved for nodules that fail conservative management. Reinke's oedema is bilateral but affects the entire cord and is associated with smoking. Polyps are typically unilateral. Carcinoma in a young non-smoker without risk factors is very unlikely, and the appearance described is not that of malignancy.
Diagnosis and Differential Diagnosis
The clinical diagnosis of the cause of hoarseness integrates the history (duration, character, risk factors) with laryngoscopic findings. A systematic approach prevents both under-investigation of malignancy and over-investigation of benign conditions.
Provided image
Acute laryngitis: onset over hours to days following an upper respiratory infection or vocal overuse; the voice is rough, low-pitched and effortful; mild oedema and hyperaemia of the vocal cords on laryngoscopy; usually self-limiting within 7–14 days; management = voice rest, steam inhalation, treatment of the underlying URI, avoidance of irritants. Rarely requires laryngoscopy unless the patient is a performer or the episode is unusually prolonged.
Chronic laryngitis: persistent hoarseness >3 weeks from chronic irritation (tobacco smoke, alcohol, reflux, dust, occupational irritants); laryngoscopy shows erythema, thickening and irregular mucosa; important because it represents a background of laryngeal dysplasia (leukoplakia) in smokers that can progress to carcinoma. Biopsy is required when leukoplakia is present.
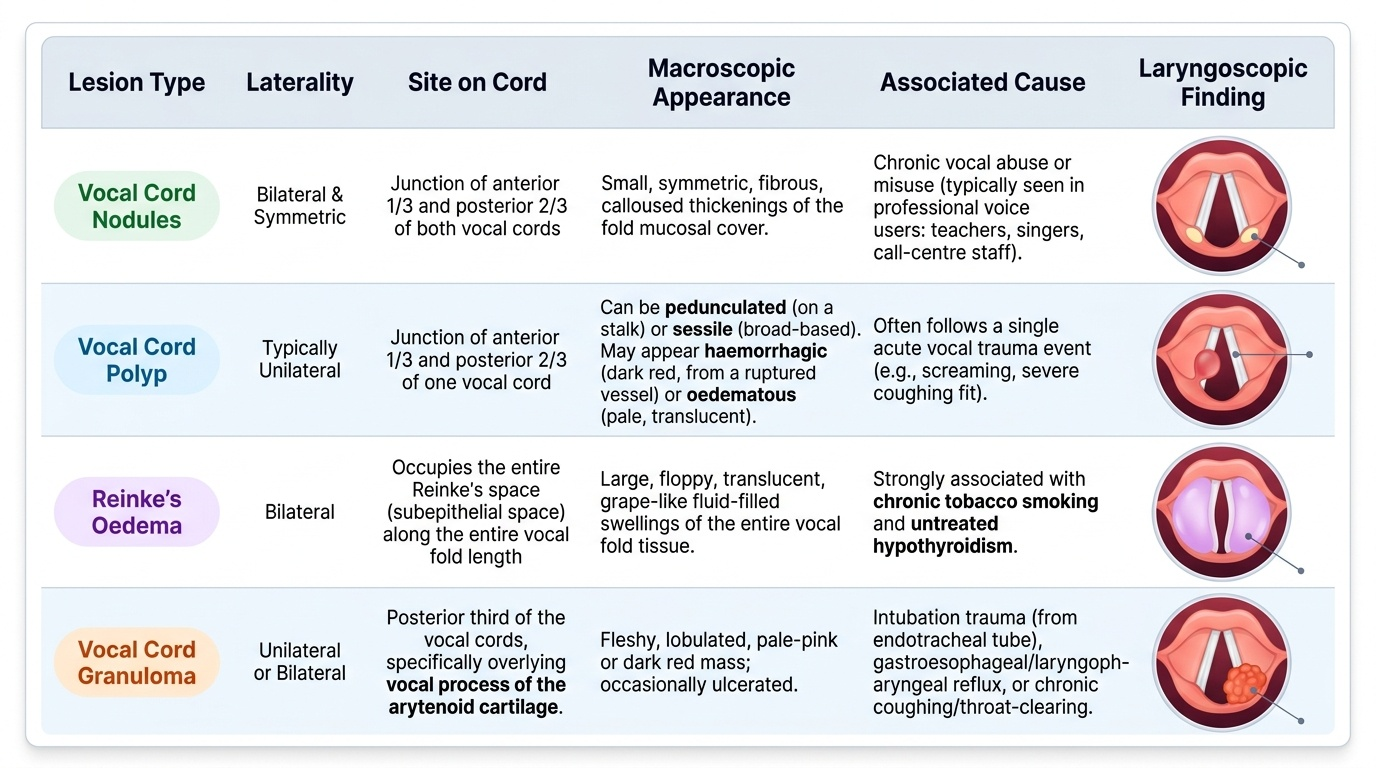
Vocal cord nodules: bilateral, symmetric, fibrous thickenings at the junction of the anterior one-third and posterior two-thirds of both vocal cords (the point of maximum vibratory amplitude); in professional voice users (teachers, singers, call-centre staff); voice is rough and fatigable; first-line = voice therapy 3–6 months.
Vocal cord polyp: typically unilateral, at the anterior one-third/posterior two-thirds junction; may be pedunculated or sessile; haemorrhagic (red, from a ruptured vocal fold vessel) or oedematous (translucent/pale); often follows a single vocal trauma event (shouting, coughing). Surgical excision by microlaryngoscopy is standard.
Reinke's oedema (polypoid degeneration): bilateral subepithelial oedema of the entire vocal fold, occupying Reinke's space; the cords appear as large, translucent, grape-like swellings; produces a markedly low-pitched 'gruff' voice (typical presentation in a middle-aged female smoker with a surprisingly deep voice); strongly associated with smoking and hypothyroidism. Management: smoking cessation and treatment of hypothyroidism; surgical drainage and trimming of the redundant mucosa (phonomicrosurgery) if voice is significantly compromised.
Vocal cord granuloma: at the posterior vocal process of the arytenoid (not the free edge); associated with laryngopharyngeal reflux (most common), post-intubation trauma, or vocal abuse. Treated with anti-reflux therapy; surgery carries a high recurrence rate.
Glottic carcinoma: persistent hoarseness is the EARLIEST symptom — this is because glottic tumours arise at the level of the vibrating vocal fold and immediately disrupt phonation. The cord may appear irregular, thickened, leukoplakic or frankly ulcerative. Impaired cord mobility (partial fixation) and eventually cord fixation indicate deeper muscle invasion. Lymph node spread is uncommon in early glottic carcinoma because the true vocal fold has a poor lymphatic supply — this is why early glottic carcinoma has an excellent prognosis. Biopsy under microlaryngoscopy confirms the diagnosis; CT staging for treatment planning.
Supraglottic carcinoma: involves the epiglottis, aryepiglottic folds or false cords; hoarseness occurs late (the true cords are not involved early); the supraglottis has a rich bilateral lymphatic supply — bilateral cervical lymphadenopathy may be the presenting feature before voice change. Prognosis is significantly worse than glottic carcinoma for the same reason.
Vocal cord palsy (discussed above): unilateral palsy = breathy weak voice; bilateral palsy = stridor with airway compromise. Distinguishing features: asymmetric cord movement on laryngoscopy; need to image the full RLN course.
Principles of Management
Management of hoarseness is cause-specific, and choosing the right treatment requires a clear diagnosis established through the history and laryngoscopy. The overarching framework has three tiers: first, conservative measures that address modifiable causes and protect the mucosa; second, medical or behavioural therapies targeting specific aetiologies; and third, surgical intervention for lesions that fail conservative treatment or require tissue diagnosis and excision. This hierarchy is not merely a matter of preference — inappropriate early surgery on vocal cord nodules without a preceding course of voice therapy carries a significant risk of recurrence, because the underlying phonatory trauma that created the nodule has not been corrected. Similarly, empirical voice rest and reflux treatment may resolve a granuloma that would otherwise recur repeatedly after surgery. Understanding why the treatment sequence matters is as important as knowing what treatment to prescribe.
Conservative measures common to most causes:
- Voice rest: complete voice rest (absolute silence, not whispering — whispering is effortful and can worsen vocal fold trauma) for 7–14 days in acute laryngitis and following vocal cord haemorrhage.
- Vocal hygiene: adequate hydration (6–8 glasses of water daily), avoidance of throat-clearing and whispering, smoking and alcohol cessation, anti-reflux measures (elevation of head end, dietary modification, proton pump inhibitors).
- Treat reversible systemic causes: thyroxine replacement restores the voice in hypothyroid hoarseness; treatment of laryngopharyngeal reflux with PPIs often resolves granuloma and posterior laryngitis.
Vocal cord nodules: voice therapy by a speech-language pathologist for 3–6 months is the established first-line treatment and resolves the majority of nodules; microlaryngoscopic excision is reserved for nodules persisting after adequate voice therapy. Technique = cold instrument excision or laser, preserving the overlying epithelium and Reinke's space to prevent scarring.
Vocal cord polyp: microlaryngoscopy and excision (cold steel or CO2 laser); specimen sent for histopathology. Concurrent anti-reflux therapy. Voice therapy post-operatively to prevent recurrence.
Reinke's oedema: smoking cessation (mandatory and often partially reverses the oedema); treat hypothyroidism; phonomicrosurgery (cordotomy and evacuation of the oedematous contents with trimming of excess mucosa) when voice is severely affected — never strip the entire cord (causes scarring and worse voice).
Unilateral vocal cord palsy: if due to an identifiable cause, treat the underlying cause first. Voice compensation may occur spontaneously in 6–12 months as the contralateral cord learns to cross the midline. For persistent palsy with severe dysphonia or aspiration risk: vocal fold medialization — Type I thyroplasty (Isshiki classification) involves inserting a silicone or Gore-Tex implant through a window in the thyroid cartilage to push the paralysed cord toward the midline; alternatively, injection laryngoplasty (injection of fat, Gelfoam or hyaluronic acid into the paralysed cord) provides temporary or permanent medialization. Speech therapy.
Bilateral vocal cord palsy: immediate airway assessment — if stridor is present, this is an airway emergency requiring urgent tracheostomy. Once the airway is secured and the underlying cause treated, surgical options for restoring abduction include posterior cordotomy (CO2 laser), arytenoidectomy, or laryngeal reinnervation procedures.
Glottic carcinoma:
- T1 (confined to one or both cords, normal mobility): primary radiotherapy (RT) is the standard in India — equal disease control to surgery and better voice preservation. Five-year disease-specific survival >90% for T1a.
- T2 (extension beyond the glottis, impaired cord mobility): radiotherapy with or without chemotherapy; or partial laryngectomy.
- T3/T4 (cord fixation, cartilage invasion, extralaryngeal spread): concurrent chemoradiotherapy (cisplatin-based organ preservation protocol) or total laryngectomy. Neck dissection for nodal disease.
| Condition | First-line | Surgical option | Prognosis |
|---|---|---|---|
| Acute laryngitis | Voice rest, treat URI | — | Excellent (self-limiting) |
| Vocal cord nodules | Voice therapy 3–6 months | Microlaryngoscopic excision | Excellent |
| Vocal cord polyp | Voice rest, anti-reflux | Microlaryngoscopic excision | Excellent |
| Reinke's oedema | Smoking cessation, treat hypothyroid | Phonomicrosurgery | Good |
| Unilateral VCP | Treat cause, voice therapy | Type I thyroplasty / injection | Variable (cause-dependent) |
| T1 glottic Ca | Radiotherapy | Partial laryngectomy | Excellent (>90% at 5yr) |
| Supraglottic Ca | CRT / surgery depending on stage | Total laryngectomy + neck dissection | Moderate (stage-dependent) |
CLINICAL PEARL
The most dangerous clinical habit in managing hoarseness is labelling persistent hoarseness as 'chronic laryngitis' without performing a laryngoscopy. Laryngitis is a diagnosis of exclusion that requires visualisation of the vocal cords to confirm benign inflammation and exclude a cord lesion. The rule is absolute: any hoarseness persisting beyond three weeks in an adult requires laryngoscopy — and a smoker with hoarseness requires it regardless of duration. A glottic carcinoma diagnosed at T1 has a five-year survival exceeding 90%. The same carcinoma at T3 (cord fixation) has a survival of approximately 50–60%. That difference lives entirely in the interval between the patient's first symptom and the clinician's first laryngoscopy.
Self-Assessment: Hoarseness
Test your understanding of the material in this SDL with the following consolidation exercise. Each scenario is drawn from common clinical presentations you are likely to encounter during your ENT posting and in final-year clinical examinations. For each scenario, apply the structured approach you have learned: first establish the duration of hoarseness and the risk-factor profile, then correlate with the laryngoscopic finding described, and finally choose the management based on the diagnosis rather than the symptom alone. Noticing that two patients may both have chronic hoarseness but require entirely different workups — one because of professional voice overuse and another because of smoking with an irregular cord — is the core clinical skill that this SDL has aimed to build. Work through each vignette independently before reading the discussion.
Scenario A: A 40-year-old male call-centre team leader has had hoarseness for three months. He speaks continuously for 10–12 hours daily. There is no smoking history. On IDL, bilateral small whitish nodular thickenings are seen at the junction of the anterior one-third and posterior two-thirds of both vocal cords. Cord movement is normal and symmetrical.
- Diagnosis? Management?
Scenario B: A 65-year-old male presents with progressive hoarseness for eight weeks, unintentional weight loss of 5 kg over two months, and referred left otalgia. He has smoked 40 cigarettes daily for 40 years and drinks alcohol regularly. IDL shows an irregular lesion on the left vocal cord with impaired mobility.
- What is your working diagnosis? What is the immediate investigation? What staging modality is required?
Scenario C: A 48-year-old female who underwent total thyroidectomy for thyroid carcinoma six months ago presents with a weak, breathy voice and aspiration of liquids. On FFNL, the left vocal cord is fixed in the paramedian position.
- Diagnosis? What would you offer if the palsy persists beyond 12 months?
Key points for self-check:
- Name the single muscle that abducts the vocal cords and its nerve supply.
- State the anatomical reason the left RLN is more susceptible to mediastinal disease than the right RLN.
- At what duration of hoarseness does laryngoscopy become mandatory, and why?
- Distinguish glottic from supraglottic carcinoma in terms of presenting symptom, lymphatic spread, and prognosis.
- What is the first-line treatment for T1 glottic carcinoma in India?
Answers for self-check:
- Posterior cricoarytenoid (PCA) muscle; recurrent laryngeal nerve.
- Left RLN loops under the aortic arch (intrathoracic course), making it vulnerable to mediastinal pathology; right RLN loops under the subclavian artery at the thoracic inlet.
- Greater than three weeks — because glottic carcinoma must be excluded, and early diagnosis markedly improves survival.
- Glottic: earliest symptom is hoarseness (good lymphatics absent), excellent prognosis; supraglottic: late hoarseness, early bilateral cervical lymphadenopathy (rich lymphatics), worse prognosis.
- Primary radiotherapy — provides equal disease control to surgery with better voice preservation.