Page 8 of 20
EN4.42 | Malignancy of Larynx Hypopharynx — SDL Guide (Part 2)
Investigations and Staging
The investigation of suspected laryngeal or hypopharyngeal malignancy has two goals: histological confirmation of the diagnosis and staging to guide treatment. These two goals require different investigations, and both are mandatory before any treatment decision is made.
Histological confirmation requires tissue — specifically, a biopsy of the primary lesion. In laryngeal carcinoma, this is obtained by direct laryngoscopy under general anaesthesia with microlaryngoscopy and biopsy (MLB/DL). This investigation provides: direct visualisation of the lesion's extent under magnification, assessment of cord mobility (a key staging criterion that can be difficult to assess reliably on outpatient laryngoscopy in an anxious patient), and the biopsy specimen. Indirect laryngoscopy and FFNL raise the clinical suspicion and guide the decision to proceed to MLB — they are screening tools, not definitive diagnostic investigations for malignancy.
Staging requires cross-sectional imaging:
- Contrast-enhanced CT of the larynx, neck, and chest is the primary staging modality. It assesses: cartilage invasion (thyroid/cricoid) — CT shows cartilage erosion or sclerosis (T4a); paraglottic and pre-epiglottic space invasion (upstaging); the extent and number of cervical lymph nodes (nodal staging); and pulmonary metastases or a synchronous pulmonary primary.
- MRI provides superior soft tissue detail and is particularly useful for assessing pre-epiglottic fat invasion, submucosal spread in hypopharyngeal tumours, and distinguishing tumour from oedema in irradiated patients.
- PET-CT is increasingly used for detection of occult nodal disease in the clinically N0 neck and for identification of distant metastases, particularly in hypopharyngeal carcinoma. It is especially valuable post-radiotherapy to confirm complete response.
For hypopharyngeal carcinoma, panendoscopy (triple endoscopy: laryngoscopy + rigid oesophagoscopy + bronchoscopy) is the standard investigation to: visualise and biopsy the hypopharyngeal lesion, assess its caudal extent into the oesophagus, and exclude a synchronous second primary in the oesophagus or bronchus.
Fine needle aspiration cytology (FNAC) of any palpable cervical lymph node provides cytological evidence of nodal metastases — useful for N-staging but does not replace primary site biopsy for histology.
Blood tests, nutritional assessment (albumin, prealbumin) and pulmonary function tests are performed pre-operatively in patients being considered for laryngectomy or chemoradiotherapy.
SELF-CHECK
On indirect laryngoscopy, a 58-year-old male smoker is found to have an irregular lesion on the right true vocal cord that does not cross the anterior commissure. The right cord moves normally on phonation. CT confirms the tumour is confined to the cord with no cartilage invasion and no lymphadenopathy. Biopsy confirms squamous cell carcinoma. According to TNM staging, this is T1a N0 M0. The most appropriate first-line treatment in India is:
A. Total laryngectomy with bilateral neck dissection
B. Primary radiotherapy to the larynx with curative intent
C. Concurrent chemoradiotherapy (cisplatin + RT) as organ preservation protocol
D. Partial laryngectomy (hemilaryngectomy)
Reveal Answer
Answer: B. Primary radiotherapy to the larynx with curative intent
T1a glottic carcinoma (confined to one vocal cord, normal cord mobility, no cartilage invasion, no nodes) is best treated with primary radiotherapy in India. Radiotherapy achieves disease-specific survival exceeding 90% for T1a glottic carcinoma and preserves the larynx with good voice quality. It is the standard of care (Dhingra, Hazarika). Total laryngectomy is not indicated for T1-T2 disease — it is reserved for T4 disease or failure of organ-preservation therapy. Concurrent chemoradiotherapy (the organ-preservation protocol) is used for T3 disease — it adds toxicity that is unnecessary for T1. Hemilaryngectomy (partial laryngectomy) is an alternative surgical option for T1-T2 but is not the preferred first-line approach when radiotherapy achieves equivalent results with a functioning larynx.
Diagnosis and Staging Classification
The diagnosis of laryngeal carcinoma is established by histopathological examination of a biopsy specimen — the clinical and laryngoscopic suspicion, however compelling, cannot replace tissue diagnosis before treatment. The TNM (Tumour-Node-Metastasis) staging system — developed by the Union for International Cancer Control (UICC) and the American Joint Committee on Cancer (AJCC) — stratifies patients into prognostically meaningful groups that guide treatment selection and allow comparison of outcomes across centres. For laryngeal carcinoma, the TNM system is particularly important because treatment intensity and technique differ dramatically between early and advanced stages: the same histological diagnosis (squamous cell carcinoma) is managed with curative radiotherapy alone at T1, and with total laryngectomy at T4. Staging therefore directly determines whether the patient retains a functioning larynx. The T-classification for glottic carcinoma is based on three criteria: the extent of cord involvement (one cord vs both cords), the status of cord mobility (normal vs impaired vs fixed), and the presence of cartilage invasion or extralaryngeal extension. Cord mobility — assessed on laryngoscopy by asking the patient to phonate — is the single most clinically accessible staging criterion and the one most directly tied to prognosis.
Provided image
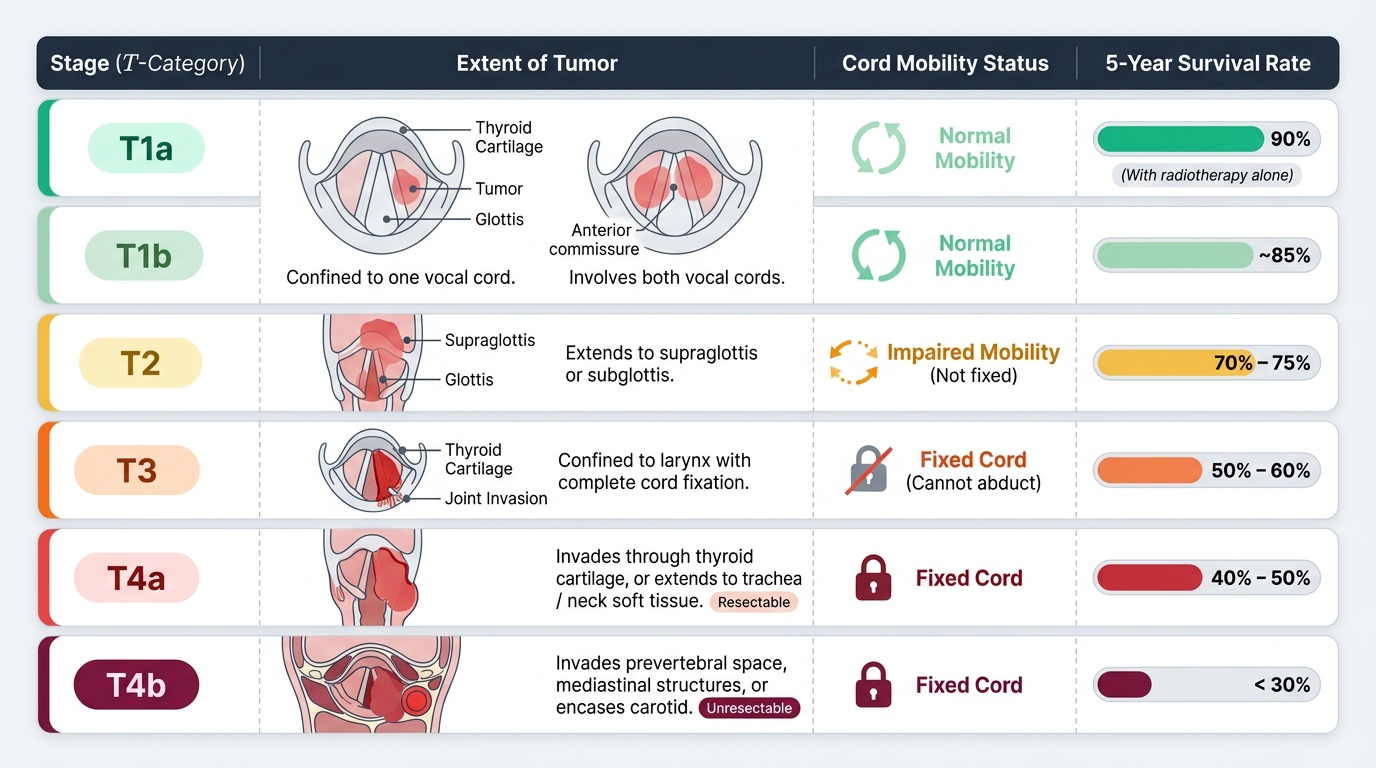
For glottic carcinoma, the staging system reflects the importance of cord mobility as a proxy for depth of invasion:
- T1a: tumour confined to one vocal cord, normal mobility; 5-year survival >90% with radiotherapy.
- T1b: tumour involves both vocal cords, normal mobility; 5-year survival ~85%.
- T2: tumour extends to supraglottis or subglottis, OR cord mobility is impaired (not fixed); 5-year survival ~70-75%.
- T3: tumour is confined to the larynx with cord fixation (inability to abduct on laryngoscopy), indicating invasion of the cricoarytenoid joint or the thyroarytenoid muscle; 5-year survival ~50-60%.
- T4a: tumour invades through the thyroid cartilage or extends beyond the larynx to trachea, soft tissues of the neck, strap muscles, thyroid gland; resectable; 5-year survival ~40-50%.
- T4b: tumour invades prevertebral space, encases carotid artery, or invades mediastinal structures; unresectable.
For supraglottic carcinoma, T-staging is based on the number of subsites involved, the presence of cord fixation (T3), and cartilage invasion (T4). The N-staging for cervical nodes is the same across all head and neck subsites: N1 = single ipsilateral node ≤3 cm; N2a = single ipsilateral node 3-6 cm; N2b = multiple ipsilateral nodes ≤6 cm; N2c = bilateral or contralateral nodes ≤6 cm; N3 = node >6 cm or extranodal extension.
Differential diagnosis of a laryngeal lesion: The clinician must distinguish laryngeal carcinoma from: benign vocal cord lesions (nodule, polyp — no ulceration, no cord fixation, no nodal disease); laryngeal papilloma (exophytic frond-like, HPV history, younger patient); laryngeal TB (rare, affects posterior larynx, associated systemic TB features, histology shows caseating granuloma, AFB positive); non-Hodgkin lymphoma of the larynx (very rare, smooth submucosal swelling, systemic lymphoma features).
Principles of Management
The management of laryngeal and hypopharyngeal carcinoma is multidisciplinary, requiring ENT surgery, radiation oncology, medical oncology, speech-language therapy, nutrition support, and palliative care. Treatment decisions are made at a multidisciplinary tumour board (MDT/MDM) and are guided by tumour stage, subsite, patient performance status and comorbidities, and — crucially — the patient's wishes regarding voice preservation.
The philosophical framework of laryngeal carcinoma management has evolved from a surgical-first approach (which prioritised disease control above all) to an organ-preservation approach (which seeks to maintain a functioning larynx without compromising survival). The evidence base for organ preservation — established through landmark randomised trials including RTOG 91-11 — demonstrates that concurrent chemoradiotherapy achieves laryngeal preservation in approximately 50% of T3 patients while producing disease control equivalent to total laryngectomy.
Stage-specific management for glottic carcinoma:
- T1a-T1b (cord confined, normal or near-normal mobility): primary radiotherapy (RT) is the standard in India — delivers 60-66 Gy in 30-33 fractions; disease-specific survival >90% for T1a; voice preservation is excellent. CO2 laser cordectomy (transoral laser microsurgery) is an alternative surgical option with comparable disease control and voice outcomes for T1a.
- T2 (impaired mobility, extension to adjacent subsite): primary radiotherapy ± concurrent chemotherapy; or partial (conservation) laryngectomy. Disease control ~70-75%.
- T3 (cord fixation, paraglottic space involvement): organ-preservation concurrent chemoradiotherapy (cisplatin 100 mg/m² every 3 weeks + RT 70 Gy in 35 fractions) — this is the RTOG protocol; salvage total laryngectomy if CRT fails. Total laryngectomy upfront if the patient is unfit for chemotherapy or if the airway is critically compromised.
- T4a (cartilage invasion): total laryngectomy + post-operative radiotherapy (PORT) with or without concurrent chemotherapy. Organ-preservation CRT is less effective for T4a; the risk of a non-functional larynx after CRT is high, making surgery the preferred primary treatment.
- T4b (unresectable): palliative concurrent CRT with cisplatin or weekly carboplatin/paclitaxel; palliative care integration.
Neck management: For early glottic carcinoma (T1-T2 N0), elective neck treatment is not required (low rate of occult nodal disease). For supraglottic carcinoma N0, elective selective neck dissection (levels II-IV) is recommended because of the 20-30% occult nodal disease rate. N+ disease requires therapeutic neck dissection or definitive chemoradiotherapy including the neck.
Total laryngectomy — when performed, involves removal of the entire larynx, creation of a permanent end-tracheostomy, and division of the pharynx. The patient permanently breathes through the neck stoma and must learn to speak using one of three methods: tracheo-oesophageal puncture (TEP) with a one-way voice prosthesis (the preferred method — the prosthesis diverts exhaled air through the oesophagus, which vibrates to produce oesophageal voice); electrolarynx (handheld vibrating device); or oesophageal speech (without a prosthesis, by learning to swallow and expel air from the oesophagus).
Hypopharyngeal carcinoma management follows similar principles but with generally worse outcomes. Piriform sinus carcinoma: organ-preservation CRT for resectable T3 with good performance status; total pharyngolaryngectomy with free flap reconstruction (jejunal or radial forearm flap) for T4 or failed CRT. Postcricoid carcinoma: pharyngolaryngo-oesophagectomy with gastric pull-up or colonic interposition for reconstruction. Palliative care for unresectable or metastatic disease.
CLINICAL PEARL
The single most important prognostic factor in laryngeal carcinoma is not the T-stage — it is the anatomical subsite. A T3 glottic carcinoma (cord fixation, but lymphatics still sparse) may still achieve 50-60% five-year survival with aggressive treatment. A T2 supraglottic carcinoma with bilateral cervical nodes carries a worse prognosis than a T3 glottic. The reason: lymphatic anatomy determines the risk of systemic spread. Reinforce this with the clinical corollary: when you see a patient with hoarseness that has been present for only three weeks, you are looking at a potentially T1 glottic carcinoma — the most curable solid tumour in ENT. When you see a patient with bilateral cervical nodes and only mild hoarseness, you are likely dealing with a supraglottic or hypopharyngeal primary — and the window of curability is much narrower.
Self-Assessment: Laryngeal and Hypopharyngeal Malignancy
Work through these consolidation vignettes and key-point questions to test your command of the material in this SDL. The three scenarios span the spectrum of laryngeal and hypopharyngeal malignancy — early glottic, advanced supraglottic, and hypopharyngeal — and require you to apply the staging system and management principles rather than recite them.
Scenario A: A 53-year-old male presents with six weeks of hoarseness. He is a 25-pack-year smoker. IDL shows an irregular thickening of the right true vocal cord that does not cross the anterior commissure; cord mobility is normal. CT shows no cartilage erosion and no cervical nodes. Biopsy = squamous cell carcinoma. Stage? First-line treatment? Expected 5-year survival?
Scenario B: A 65-year-old male smoker presents with a painless 4 cm left neck mass for three months. He has mild hoarseness. IDL shows an irregular epiglottis with extension to the left aryepiglottic fold and the left arytenoid. The left cord shows impaired mobility. CT confirms a supraglottic mass with bilateral cervical nodes, no cartilage invasion. Biopsy = SCC. What is the T-stage? What is the N-stage (bilateral nodes, all ≤4 cm)? What treatment approach is likely?
Scenario C: A 58-year-old woman presents with progressive dysphagia for solids over four months, weight loss of 7 kg, and a sore in the throat. She has a long history of iron-deficiency anaemia with koilonychia and dysphagia (for which she had never sought investigation). Barium swallow shows a postcricoid filling defect. What is the most likely diagnosis? What syndrome predisposed her to this?
Key recall questions:
- State the T-staging criteria for glottic carcinoma T1a vs T3 (the single criterion that distinguishes them).
- Why is the prognosis of glottic carcinoma better than supraglottic carcinoma at equivalent local extent?
- What is the first-line treatment for T3 glottic carcinoma in a fit patient?
- What voice rehabilitation option is preferred after total laryngectomy?
- Name the syndrome associated with postcricoid carcinoma and its three components.
Answers:
- T1a = confined to one cord, normal mobility; T3 = cord fixation (the single distinguishing criterion).
- Glottic has sparse lymphatics — late nodal spread; supraglottic has rich bilateral lymphatics — early nodal spread and worse prognosis at equivalent T-stage.
- Organ-preservation concurrent chemoradiotherapy (cisplatin + radiotherapy); salvage total laryngectomy if CRT fails.
- Tracheo-oesophageal puncture (TEP) with one-way voice prosthesis.
- Plummer-Vinson syndrome (Patterson-Kelly-Brown syndrome): iron-deficiency anaemia + dysphagia from postcricoid web + koilonychia.