Page 16 of 29
EN4.26 | Acute and Chronic Rhinitis — SDL Guide
Learning Objectives
- Elicit a structured history distinguishing acute from chronic rhinitis and identifying the aetiology
- Describe the clinical features and stages of acute viral rhinitis and acute bacterial rhinosinusitis
- Describe the clinical features of chronic rhinitis and its subtypes — hypertrophic and atrophic
- Choose appropriate investigations and describe the principles of management for each type
- Describe the clinical presentation of atrophic rhinitis including ozaena — a condition with a characteristic fetid nasal odour
INSTRUCTIONS
Acute rhinitis (the common cold) is the most common infectious disease in humans, experienced 2–4 times per year by most adults. Chronic rhinitis represents prolonged or recurrent mucosal inflammation with structural changes. EN4.26 requires you to take a correct history, describe clinical features, choose investigations, and describe management of both acute and chronic forms. This module also covers atrophic rhinitis — a distinct and important chronic nasal condition characterised by mucosal atrophy and paradoxically wide, dry, crusted nasal passages.
References
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery. 8th ed. Chapter on Rhinitis (textbook)
- Hazarika P, Nayak DR, Balakrishnan R. Textbook of Ear, Nose and Throat — Head and Neck Surgery. Chapter on Acute and Chronic Rhinitis (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery. 8th ed. Vol 2: Rhinology — Inflammatory Disease (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 55-year-old woman is referred from the medical OPD because other patients in the waiting room have complained of a foul odour coming from her. She is embarrassed and distressed. She has had nasal crusting and a dry nose for 20 years. She herself cannot smell the odour — she has complete anosmia. On anterior rhinoscopy, both nasal passages are paradoxically wide, filled with thick greenish-yellow crusts that are adherent to the mucosa. When you remove a crust with forceps, the underlying mucosa bleeds slightly. There is no polyp, no septal perforation, no foreign body. What is this condition? Why is the nasal passage paradoxically wide? And why has she lost her sense of smell entirely?
WHY THIS MATTERS
Acute rhinitis (common cold) is the most frequently occurring infectious disease in humans, responsible for more lost working days and school days than any other illness. Understanding its natural history — and crucially when bacterial superinfection has occurred requiring antibiotics — prevents the most common antibiotic prescribing error in primary care: treating viral rhinitis with antibiotics. Chronic rhinitis and its subtypes — hypertrophic, atrophic, ozaena — represent end-stage mucosal consequences of uncontrolled chronic inflammation, recurrent infection, or specific infections (syphilis, leprosy, rhinoscleroma) that are more prevalent in the Indian subcontinent than elsewhere. Atrophic rhinitis with ozaena is a classically described and examination-favourite ENT condition that causes immense social disability and is frequently seen in ENT outpatients in India.
RECALL
Recall from your microbiology and immunology sessions the structure and function of the nasal mucosa. The nasal cavity is lined by pseudostratified ciliated columnar epithelium (respiratory epithelium) with interspersed goblet cells producing mucus. The mucociliary escalator — the coordinated beating of cilia moving the overlying mucus blanket toward the nasopharynx — is the primary innate defence mechanism of the upper respiratory tract, clearing inhaled particles, bacteria, and viruses. From your microbiology sessions, the most common viral causes of acute rhinitis (common cold) are rhinoviruses (the most common, >100 serotypes), coronaviruses, respiratory syncytial virus (RSV), influenza and parainfluenza viruses, and adenoviruses. Bacterial causes of acute rhinitis and rhinosinusitis include Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis — the same pathogens that cause acute otitis media. This shared microbiology reflects the continuity of the upper respiratory mucosal surface.
Acute Rhinitis: Clinical Features and Management
Acute rhinitis is an acute inflammatory condition of the nasal mucosa, almost always caused by viral infection in its initial phase. The clinical presentation follows a well-defined sequence that reflects the virus-host interaction in the nasal mucosa, and understanding this sequence allows the clinician to distinguish a straightforward viral upper respiratory tract infection from one that has developed a bacterial complication.
The clinical stages of acute viral rhinitis (Dhingra's description):
Stage 1 — Dry/irritation stage (day 1–2): nasal dryness, burning, and sensation of stuffiness. The patient is irritable and may feel unwell. Temperature may be slightly elevated. The mucosa appears red and congested on rhinoscopy. No nasal discharge yet.
Stage 2 — Catarrhal/secretion stage (day 2–4): profuse watery nasal discharge (rhinorrhoea), sneezing, and bilateral nasal obstruction. Lacrimation (watery eyes from nasolacrimal duct congestion) and nasal itch. This is the peak symptomatic stage. The nasal discharge is watery and profuse — not mucopurulent.
Stage 3 — Resolution or bacterial superinfection: in most cases, symptoms resolve over 5–10 days. The watery discharge becomes mucoid and then disappears. However, in some patients — particularly those with concurrent allergic rhinitis, DNS, or immunocompromise — bacterial superinfection occurs. The discharge becomes thick, mucopurulent, and yellowish-green; facial pain and pressure over the affected sinuses develop (sinusitis); symptoms worsen after initial improvement (the 'double-sickening' sign). Bacterial superinfection is the indication for antibiotic therapy.
Management of acute viral rhinitis:
- Symptomatic relief: paracetamol or ibuprofen for fever and myalgia; oral decongestants (pseudoephedrine) or short-term topical decongestants (oxymetazoline, 3–5 days maximum) for nasal obstruction; saline nasal irrigation.
- Antibiotics are NOT indicated for uncomplicated acute viral rhinitis. The yellow-green colour of nasal discharge in the later stages of a viral cold reflects neutrophilic breakdown products and does NOT indicate bacterial infection requiring antibiotics.
- Antibiotics ARE indicated if bacterial superinfection (acute rhinosinusitis) is suspected: persistent symptoms >10 days without improvement, symptoms worsening after initial improvement, or severe symptoms (high fever >38.5°C, severe unilateral facial pain) — treat with amoxicillin (or amoxicillin-clavulanate if severe/failure of first-line).
Chronic Rhinitis: Hypertrophic and Atrophic Types
Chronic rhinitis refers to persistent or recurrent nasal mucosal inflammation lasting more than 12 weeks. Unlike acute rhinitis, chronic rhinitis reflects structural changes in the nasal mucosa — either mucosal hypertrophy (thickening and engorgement) or mucosal atrophy (thinning and scarring). These two ends of the pathological spectrum present very differently and require entirely different management approaches.
Chronic Hypertrophic Rhinitis:
Long-standing mucosal inflammation — from recurrent infections, chronic allergic rhinitis, vasomotor rhinitis, or recurrent viral colds — leads to progressive hypertrophy of the nasal mucosal lining, particularly of the inferior turbinate. The mucosal epithelium undergoes metaplasia from ciliated pseudostratified columnar to squamous or transitional epithelium; submucosal fibrosis develops; and the turbinate becomes firm, non-compressible, and permanently enlarged. This is distinct from the soft, engorged, reversible inferior turbinate of acute allergic or vasomotor rhinitis — in hypertrophic rhinitis, the turbinate does not shrink with topical decongestants.
Clinical features of hypertrophic rhinitis:
- Persistent bilateral nasal obstruction — the turbinates are permanently enlarged.
- Thick, mucoid or mucopurulent nasal discharge.
- Post-nasal drip, throat clearing.
- Key examination finding: the inferior turbinate is enlarged and firm — does NOT blanch or shrink with topical decongestant spray (e.g. oxymetazoline). This non-response to decongestant (in contrast to the soft, reversible turbinate of allergic rhinitis) is the cardinal distinguishing feature of hypertrophic turbinate.
- The turbinate surface may be lobulated and pale, superficially resembling a nasal polyp — distinguished by probing (turbinate is sessile, attached to lateral wall; polyp is pedunculated, mobile).
Management of hypertrophic rhinitis: once established, medical therapy (INCS, decongestants) has limited effect on the fixed fibrous hypertrophy. Surgical reduction of the inferior turbinate is required — inferior turbinate reduction by submucosal diathermy, radiofrequency ablation, cryotherapy, or partial turbinectomy.
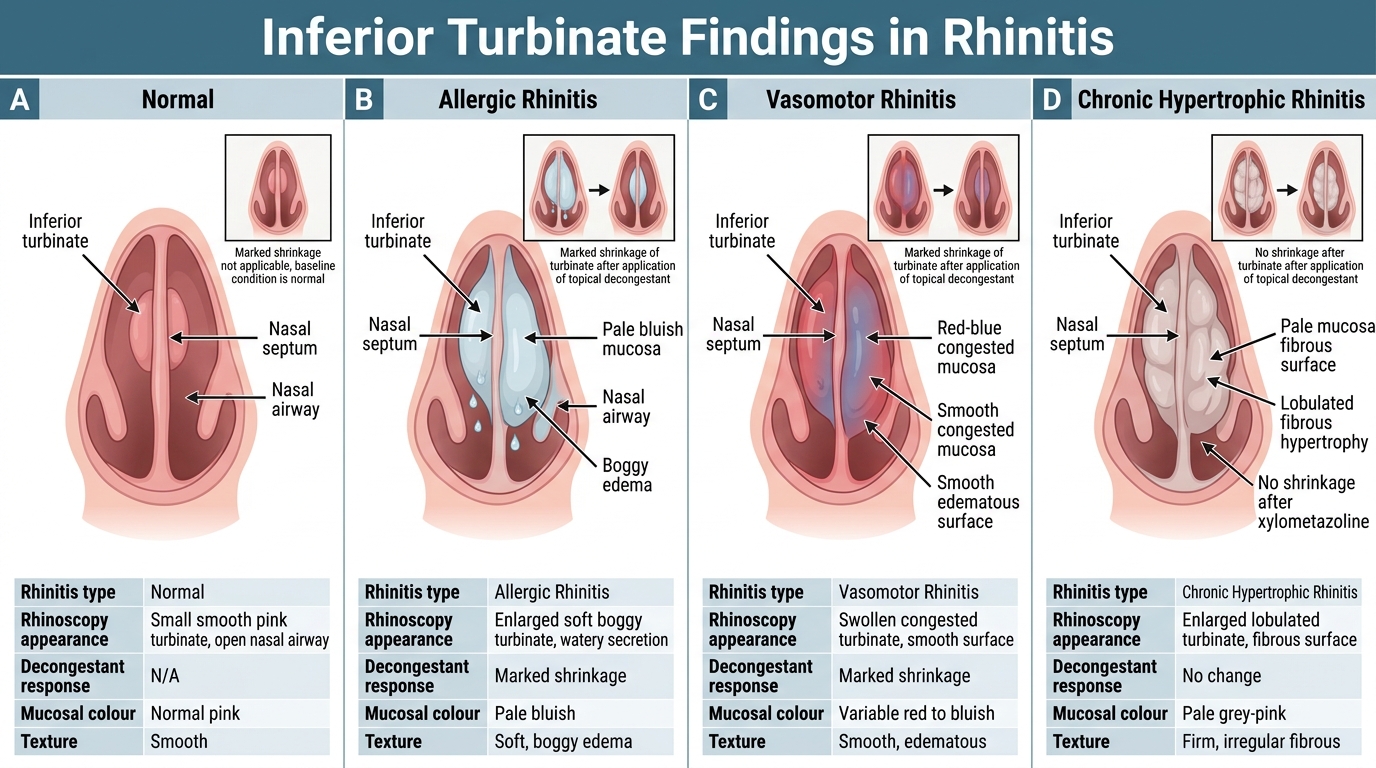
Inferior Turbinate Findings in Rhinitis
SELF-CHECK
On anterior rhinoscopy of a 50-year-old man with a 15-year history of bilateral nasal obstruction, you see bilaterally enlarged inferior turbinates with a lobulated surface and pale mucosa. You spray 1% xylometazoline into both nostrils and re-examine 10 minutes later — the turbinates are unchanged in size. The most likely diagnosis is:
A. Bilateral nasal polyps — they do not shrink with topical decongestants
B. Chronic hypertrophic rhinitis with fixed fibrous turbinate hypertrophy
C. Allergic rhinitis with temporary decongestant failure
D. Bilateral antrochoanal polyps
Reveal Answer
Answer: B. Chronic hypertrophic rhinitis with fixed fibrous turbinate hypertrophy
Non-response to topical decongestant is the cardinal finding of chronic hypertrophic rhinitis — the inferior turbinate has undergone irreversible fibrous hypertrophy (submucosal fibrosis replaces the normally erectile vascular tissue), so it no longer responds to vasoconstriction. In allergic or vasomotor rhinitis, the turbinate is soft and vascular — it shrinks markedly with a decongestant. The lobulated pale turbinate in this patient superficially resembles nasal polyps, but polyps are pedunculated and arise from the middle meatus; turbinates are attached to the lateral nasal wall. Bilateral antrochoanal polyps do not exist — by definition, the antrochoanal (Killian's) polyp is always unilateral and single.
Atrophic Rhinitis and Ozaena
Atrophic rhinitis is a distinct and important chronic nasal condition characterised by progressive atrophy of the nasal mucosa and underlying turbinate bones, resulting in wide, spacious, dry nasal passages filled with thick, dried, foul-smelling crusts. It represents the diametrically opposite pathological end to hypertrophic rhinitis — instead of too much tissue, there is too little. Atrophic rhinitis is more prevalent in tropical and developing countries, including India, and is more common in young women — a demographic pattern that has led to speculation about hormonal and nutritional factors in its pathogenesis. Understanding atrophic rhinitis is clinically important because it causes severe social disability (the foul odour is detected by everyone except the patient), it is readily diagnosed on clinical grounds, and it is frequently seen in ENT outpatient departments in India where appropriate management can dramatically improve quality of life.
Types of atrophic rhinitis:
1. Primary atrophic rhinitis (ozaena): the classical form, more prevalent in tropical and subtropical countries including India. The aetiology is uncertain but involves endocrine, nutritional, and infective components. Klebsiella ozaenae (formerly Bacillus foetidus ozaenae) is the organism most frequently isolated from the nasal crusts — though whether it is a primary cause or a secondary coloniser is debated.
2. Secondary atrophic rhinitis: follows known causes — excessive turbinate surgery (over-aggressive partial turbinectomy), specific granulomatous infections (syphilis, tuberculosis, leprosy, rhinoscleroma), radiotherapy to the nasal region, trauma.
Pathology: The mucosal epithelium changes from ciliated pseudostratified columnar to squamous metaplasia. Submucosal glands and vessels undergo progressive fibrosis. Turbinate bones are resorbed. The nasal passages become paradoxically wide — yet the patient feels obstructed, because the absence of normal air turbulence over the turbinates eliminates the sensation of airflow (this is called paradoxical nasal obstruction).
Clinical features of atrophic rhinitis/ozaena:
- Foul-smelling nasal discharge (ozaena): the most socially disabling feature; the crusts harbour anaerobes and Klebsiella that produce the characteristic fetid odour. Crucially, the patient often cannot smell the odour because they have complete anosmia — a paradox that leads to social isolation.
- Anosmia: destruction of the olfactory mucosa and obstruction of the olfactory cleft by crusts; may be complete.
- Nasal crusting: thick, greenish-grey, adherent crusts covering wide nasal passages; when removed, the underlying mucosa is thin, atrophic, and bleeds slightly.
- Paradoxical nasal obstruction: despite wide nasal passages, the patient feels blocked (absence of normal airflow sensation).
- Wide nasal passages on rhinoscopy — in contrast to most nasal diseases that cause narrowing.
- Occurs more commonly in young women and in dry, hot climates.
Management of atrophic rhinitis:
- Nasal irrigation: regular irrigation with warm isotonic or hypertonic saline to remove crusts and hydrate the mucosa; the mainstay of conservative management.
- Local application: glucose-glycerine drops (antibacterial, hygroscopic); oestrogen nasal drops (historically used to stimulate mucosal regeneration — controversial efficacy).
- Antibiotics: systemic treatment targeting Klebsiella ozaenae for acute exacerbations — ciprofloxacin or co-trimoxazole.
- Surgical: Young's operation — surgical closure of the anterior nares (partial obliteration) to reduce airflow through the nasal cavity, allowing the mucosa to rest and partially regenerate; the closure is maintained for 6 months and then reopened. A definitive procedure for severe ozaena.
SELF-CHECK
A 25-year-old woman presents with anosmia, nasal crusting, and complaints from her family of a persistent foul smell from her nose. She herself is unaware of the odour. On rhinoscopy, both nasal passages are paradoxically wide with thick greenish-grey crusts. The most likely diagnosis and its characteristic organism are:
A. Nasal foreign body — a small retained object; organism = Staphylococcus aureus
B. Primary atrophic rhinitis (ozaena) — organism most commonly isolated = Klebsiella ozaenae
C. Chronic rhinosinusitis with polyposis — organism = Aspergillus species
D. Septal perforation with crusting — associated with intranasal cocaine use
Reveal Answer
Answer: B. Primary atrophic rhinitis (ozaena) — organism most commonly isolated = Klebsiella ozaenae
The classic presentation of primary atrophic rhinitis (ozaena) is: young woman, paradoxically wide nasal passages, thick adherent crusts, foul odour (undetected by the patient due to anosmia), and anosmia. Klebsiella ozaenae is the organism most commonly isolated from the crusts of ozaena. The paradox of a 'wide' nose with a sensation of blockage (paradoxical nasal obstruction) results from loss of normal mucosal turbulence sensation. This clinical picture is highly characteristic and should be recognised immediately. Nasal foreign bodies cause unilateral, not bilateral disease. Sinusitis with polyposis would show narrowed passages with polyps, not widened passages with crusts.