Page 7 of 29
EN4.23 | Adenoids — SDL Guide
Learning Objectives
- Elicit a structured history from a child presenting with adenoid hypertrophy, identifying nasal obstruction, mouth breathing, snoring, hearing loss, and recurrent ear infections
- Describe the anatomy and physiology of the adenoids and explain how hypertrophy causes nasal obstruction and Eustachian tube dysfunction
- Describe the examination findings and investigations used to diagnose adenoid hypertrophy, including lateral X-ray and nasal endoscopy
- Identify the consequences of untreated adenoid hypertrophy — adenoid facies, obstructive sleep apnea, conductive hearing loss from OME
- Describe the indications for adenoidectomy, the procedure overview, and its major complications
INSTRUCTIONS
Adenoid hypertrophy is the commonest cause of nasal obstruction in children aged 3–10 years and a major cause of childhood conductive hearing loss via Eustachian tube dysfunction. EN4.23 requires you to take a correct history, describe clinical features, choose investigations, and describe management. This module builds the skills to recognise adenoid disease early — before it causes irreversible hearing loss, facial growth disruption, or obstructive sleep apnea.
References
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery. 8th ed. Chapter on Adenoids (textbook)
- Hazarika P, Nayak DR, Balakrishnan R. Textbook of Ear, Nose and Throat — Head and Neck Surgery. Chapter on Adenoid Hypertrophy (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery. 8th ed. Vol 2: Paediatric ENT — Adenoids and Tonsils (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 6-year-old boy is brought by his mother to the ENT OPD. She says he has been breathing through his mouth since the age of 3, snores loudly every night, and his teachers report that he is inattentive in class and struggles to hear instructions. His mother also mentions that he has had four ear infections in the past year requiring antibiotics each time. His school audiogram flagged bilateral hearing loss of 30–40 dB. On examination, his mouth is hanging open, his face appears elongated with a narrow upper jaw, and his nasal passages appear clear on anterior rhinoscopy. You cannot see any obvious nasal pathology — yet this child has significant disease. Where is the lesion, and why can't you see it from the front?
WHY THIS MATTERS
Adenoid hypertrophy is the single most common cause of nasal obstruction in children and one of the leading causes of childhood conductive hearing loss in India. The adenoids are an obligate part of the child's immune apparatus and undergo normal growth in early childhood, but when they enlarge enough to obstruct the choanae or the Eustachian tube ostia, the consequences range from chronic mouth breathing and sleep disruption to progressive conductive deafness and characteristic facial deformity. These are not trivial outcomes: unrecognised hearing loss in a 5-year-old during the critical period of language acquisition can set back speech and reading development by years. Adenoidectomy is one of the most commonly performed operations in paediatric ENT globally — you will advise on it in general practice, paediatric OPD, and ENT postings, and parents will ask you to explain it clearly.
RECALL
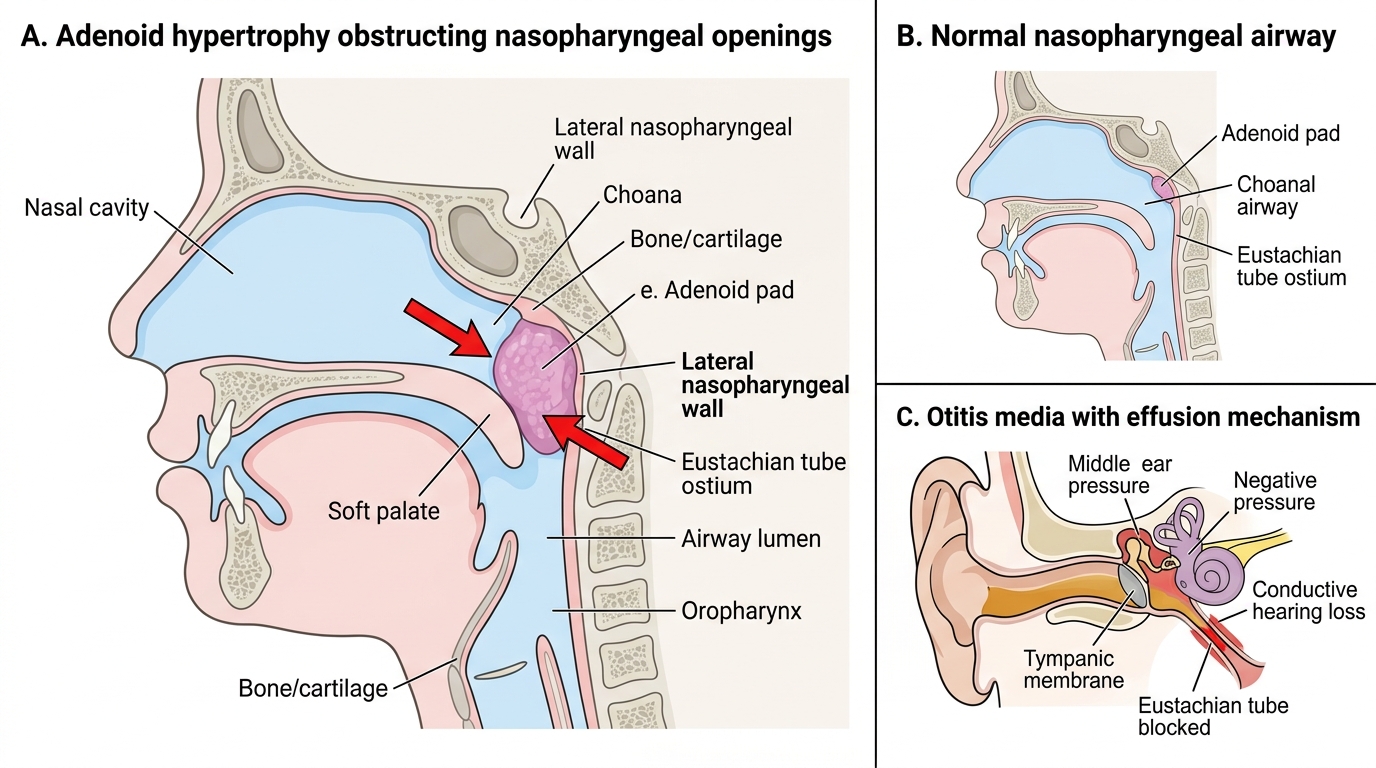
Recall from your anatomy sessions the structure of Waldeyer's ring — the lymphoid tissue that forms a protective ring at the entry to the aerodigestive tract. Waldeyer's ring includes the palatine tonsils (lateral, the most visible, what most people call 'the tonsils'), the pharyngeal tonsil (adenoids) on the posterior nasopharyngeal wall, the lingual tonsil at the base of tongue, and the tubal tonsils (Gerlach's tonsils) around the Eustachian tube openings. The adenoids and palatine tonsils are largest in early childhood and involute at puberty. From physiology (PY), recall the Eustachian tube: it runs from the anterior wall of the middle ear cleft to open on the lateral wall of the nasopharynx. Its function is to equalise pressure in the middle ear and drain middle ear secretions. Obstruction of the Eustachian tube by enlarged adenoids impairs this drainage and aeration, leading to otitis media with effusion (OME), a key complication of adenoid hypertrophy.
Clinical Presentation of Adenoid Hypertrophy
Adenoid hypertrophy most commonly presents in children between the ages of 3 and 10 years — the period when adenoid tissue is naturally at its largest. The presenting symptoms are a consequence of two anatomical effects: obstruction of the posterior choanae (the posterior opening of the nasal cavity into the nasopharynx), and obstruction of the Eustachian tube ostia on the lateral nasopharyngeal walls. Understanding these two mechanisms allows you to predict the full symptom cluster from first principles, rather than memorising a list.
Nasal obstruction and mouth breathing are the cardinal presenting features. Because the choanae are blocked posteriorly, even though the anterior nasal cavity is patent (and looks normal on anterior rhinoscopy), air cannot pass through to the nasopharynx. The child compensates by breathing through the mouth. Chronic mouth breathing has multiple consequences: the oral mucosa dries out, increasing upper respiratory infections; the palate is not moulded by the tongue resting against it during nasal breathing, resulting in a high-arched palate; and the maxilla narrows.
Hyponasal voice results from loss of the nasopharyngeal resonating space. The child sounds as though they have a permanent blocked nose (speaking through the nose is absent — the 'N' sounds become 'D' sounds: 'Mummy' becomes 'Buddy'). This is the opposite of hypernasal speech (too much nasal resonance, as in a cleft palate).
Snoring and sleep-disordered breathing are common and important. Upper airway resistance during sleep increases, causing noisy breathing; severe cases progress to obstructive sleep apnea (OSA) with observable apnoeic episodes, restless sleep, nocturnal enuresis, and daytime behavioural consequences (hyperactivity, inattention, poor school performance — features that lead to referral to a paediatrician or child psychiatrist rather than an ENT surgeon if adenoids are not considered).
Recurrent otitis media — both acute suppurative (ASOM) and secretory (OME, 'glue ear') — results from Eustachian tube dysfunction. The adenoids physically obstruct or compress the tube ostia, and also serve as a bacterial reservoir seeding the middle ear. The child presents with recurrent ear infections requiring repeated antibiotic courses, bilateral conductive hearing loss, speech delay, and school inattention.
Adenoid facies is the characteristic facial appearance that develops after years of chronic mouth breathing. Features include: open mouth at rest, elongated lower face, narrow and high-arched palate, prognathic mandible, dental crowding, and a vacant or dull facial expression. These changes develop gradually over months to years and are potentially reversible if adenoidectomy is performed before bony maturation.
The history from parents should specifically include: duration of mouth breathing and snoring, number of ear infections per year, hearing concerns, speech delay, school performance, restless sleep with observed apnoeas, and the age of onset.
Anatomy and Physiology of the Adenoids
The adenoids (pharyngeal tonsil, Luschka's tonsil) are a single midline pad of lymphoid tissue situated on the posterior and superior wall of the nasopharynx, at the junction of the roof and the posterior wall. Unlike the palatine tonsils, the adenoids have no capsule — this has implications for surgery (adenoidectomy cannot be done by dissection in a capsular plane; it is done by curettage or suction diathermy). The adenoids are covered by pseudostratified ciliated respiratory epithelium, with crypts similar to but shallower than palatine tonsillar crypts.
Position and relationships: The adenoids lie directly posterior to the choanae. When enlarged, they project forward into and may completely fill the nasopharyngeal space, obstructing the posterior choanal apertures. On the lateral walls of the nasopharynx, the Eustachian tube ostia open as oval slits approximately 1–2 cm lateral to the posterior choana. Adenoid tissue extends toward and around these ostia. Hypertrophied adenoids obstruct the tube ostia by direct pressure and by serving as a reservoir of organisms causing repeated episodes of acute and chronic Eustachian tube inflammation.
Normal growth pattern: Adenoids begin growing in early infancy, reach peak size between ages 3 and 7 years (relative to the size of the nasopharynx), and then involute progressively from puberty onward under the influence of sex hormones. By the mid-teens, adenoid tissue is usually minimal. This physiological regression explains why many children with moderate adenoid hypertrophy at age 5–6 become asymptomatic by their early teens without surgery — a point relevant to counselling parents who prefer to wait.
Eustachian tube dysfunction: The Eustachian tube normally opens with swallowing and yawning, equalising pressure between the nasopharynx and the middle ear. When adenoid obstruction prevents this opening, a negative pressure develops in the middle ear. This negative pressure draws a transudate into the middle ear cavity — initially thin and watery (serous otitis media, SOM), later becoming thick and viscous (otitis media with effusion, OME, or glue ear). OME causes conductive hearing loss, typically 20–40 dB bilaterally, which may be the first sign of significant adenoid disease.
Adenoid Hypertrophy: Airway and Eustachian Tube Obstruction
SELF-CHECK
A 5-year-old child with adenoid hypertrophy develops bilateral conductive hearing loss of 30 dB. Tympanometry shows flat (type B) curves bilaterally. The most likely mechanism is:
A. Sensorineural damage from recurrent ear infections reaching the cochlea
B. Eustachian tube obstruction by the adenoids causing otitis media with effusion (glue ear)
C. Bilateral external ear canal blockage from enlarged pinna lymph nodes
D. Adenoid tissue growing through the Eustachian tube into the middle ear
Reveal Answer
Answer: B. Eustachian tube obstruction by the adenoids causing otitis media with effusion (glue ear)
Adenoid hypertrophy causes Eustachian tube dysfunction by obstructing the tube ostia in the nasopharynx. This prevents normal pressure equalization and drainage, leading to accumulation of fluid in the middle ear cavity — otitis media with effusion (OME or 'glue ear'). The fluid damps ossicular movement, causing conductive hearing loss (typically 20–40 dB). Tympanometry type B (flat curve, no peak) confirms fluid behind the intact tympanic membrane — the hallmark finding. This is NOT sensorineural (cochlear) damage. Adenoid tissue does not grow through the Eustachian tube into the middle ear.
Examination and Investigations
The examination of a child with suspected adenoid hypertrophy must begin with the recognition that the pathology is in the nasopharynx, not the anterior nasal cavity — and anterior rhinoscopy will be entirely normal or show only clear mucus. This mismatch between an impressive symptom burden (mouth breathing, snoring, hearing loss) and a normal anterior rhinoscopy is the key diagnostic pointer: if the anterior nose looks normal and the child has nasal obstruction, look behind the nasal passages at the nasopharynx.
General examination: Note the child's posture — mouth hanging open at rest, elongated face, narrow maxillary arch, hyponasal voice. These features of adenoid facies are clinical evidence of chronicity.
Anterior rhinoscopy: The anterior nasal passages appear clear — no deviation, no polyps, no foreign body. This is the crucial negative finding that shifts attention posteriorly.
Posterior rhinoscopy (indirect, using a post-nasal mirror): the traditional method to visualise the nasopharynx. Requires patient cooperation — often difficult in young children. Shows the adenoid mass as a lobulated, pink, lymphoid pad filling the nasopharyngeal vault.
Nasal endoscopy (flexible nasopharyngoscope): the modern standard, well tolerated in children with topical anaesthetic; provides direct visualisation of the adenoid size, the degree of choanal obstruction, and the state of the Eustachian tube ostia.
Investigations:
- Lateral soft tissue neck X-ray: a traditional investigation showing the adenoid shadow on the posterior nasopharyngeal wall and the degree of airway narrowing. The adenoid-nasopharyngeal (AN) ratio is measured on this film: ratio >0.7 is considered significant hypertrophy. This investigation is widely available even in resource-limited settings and is still used where endoscopy is unavailable.
- Pure tone audiometry (PTA): essential to quantify hearing loss in children with suspected OME. Children aged ≥4 years can cooperate with standard PTA.
- Tympanometry: measures middle ear compliance and detects OME. A flat (type B) tympanogram indicates fluid in the middle ear without a tympanic membrane perforation.
- Sleep study (polysomnography): for children with suspected obstructive sleep apnea — assesses frequency and severity of apnoeas, oxygen desaturation. Not available everywhere; clinical assessment and parent-reported symptoms usually guide the decision in most settings.
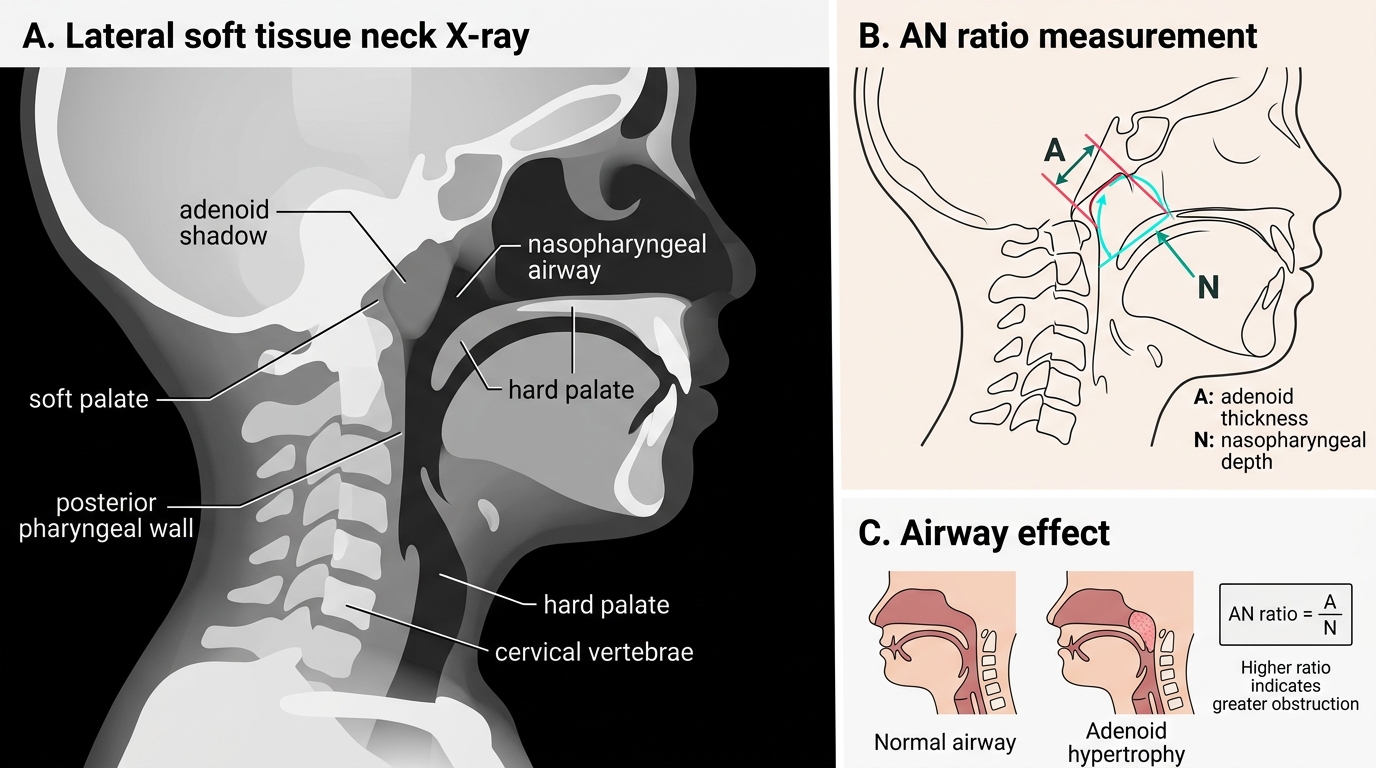
Adenoid Hypertrophy and AN Ratio on Lateral Neck X-ray