Page 4 of 29
EN4.22 | Deviated Nasal Septum — SDL Guide
Learning Objectives
- Describe the clinical features of DNS including nasal obstruction, epistaxis, headache, and sinusitis
- Identify the anatomical components of the nasal septum and classify types of septal deviation
- Perform and interpret anterior rhinoscopy findings relevant to DNS
- Choose appropriate investigations for DNS including CT PNS and state when imaging is mandatory
- Describe the principles of septoplasty — indications, age restriction, key steps, and major complications
- Distinguish septoplasty from submucous resection (SMR) and state when turbinate reduction is added
INSTRUCTIONS
Deviated nasal septum (DNS) is the commonest structural cause of nasal obstruction in adults. EN4.22 requires you to describe clinical features, choose investigations, and discuss indications and steps of septoplasty. This module provides the clinical and anatomical foundation to understand when DNS is the genuine cause of a patient's symptoms and when surgery is the right answer.
References
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery. 8th ed. Chapter on Deviated Nasal Septum (textbook)
- Hazarika P, Nayak DR, Balakrishnan R. Textbook of Ear, Nose and Throat — Head and Neck Surgery. Chapter on DNS and Septoplasty (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery. 8th ed. Vol 2: Rhinology — Septal Surgery (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old man presents with a 4-year history of left-sided nasal block and recurrent severe headaches localised to the left side of his forehead and eye region. The headaches are not throbbing, do not worsen with activity, and are not associated with nausea. He has tried multiple antihistamines, decongestants, and even consulted a neurologist who found nothing on MRI. On anterior rhinoscopy, you see the nasal septum sharply deviated to the left with a prominent bony spur at its base on the left side that is in contact with the hypertrophied left inferior turbinate. Could a bony spur in the nose explain 4 years of headaches? What is the surgical solution, and when is a 24-year-old old enough to have it safely?
WHY THIS MATTERS
Deviated nasal septum is estimated to be present to some degree in up to 80% of the general population, but only a minority are symptomatic enough to need intervention. It is the single most common structural diagnosis in ENT outpatients and the most common indication for septal surgery globally. Understanding DNS is foundational not only for ENT but for any doctor taking a history from a patient with chronic nasal obstruction, recurrent sinusitis, or unexplained facial headache. Septoplasty is one of the most commonly performed ENT procedures — you will encounter it in every ENT posting, it appears in examinations, and it is a procedure you need to understand conceptually at the KH (knowledge for supervised practice) level per EN4.22.
RECALL
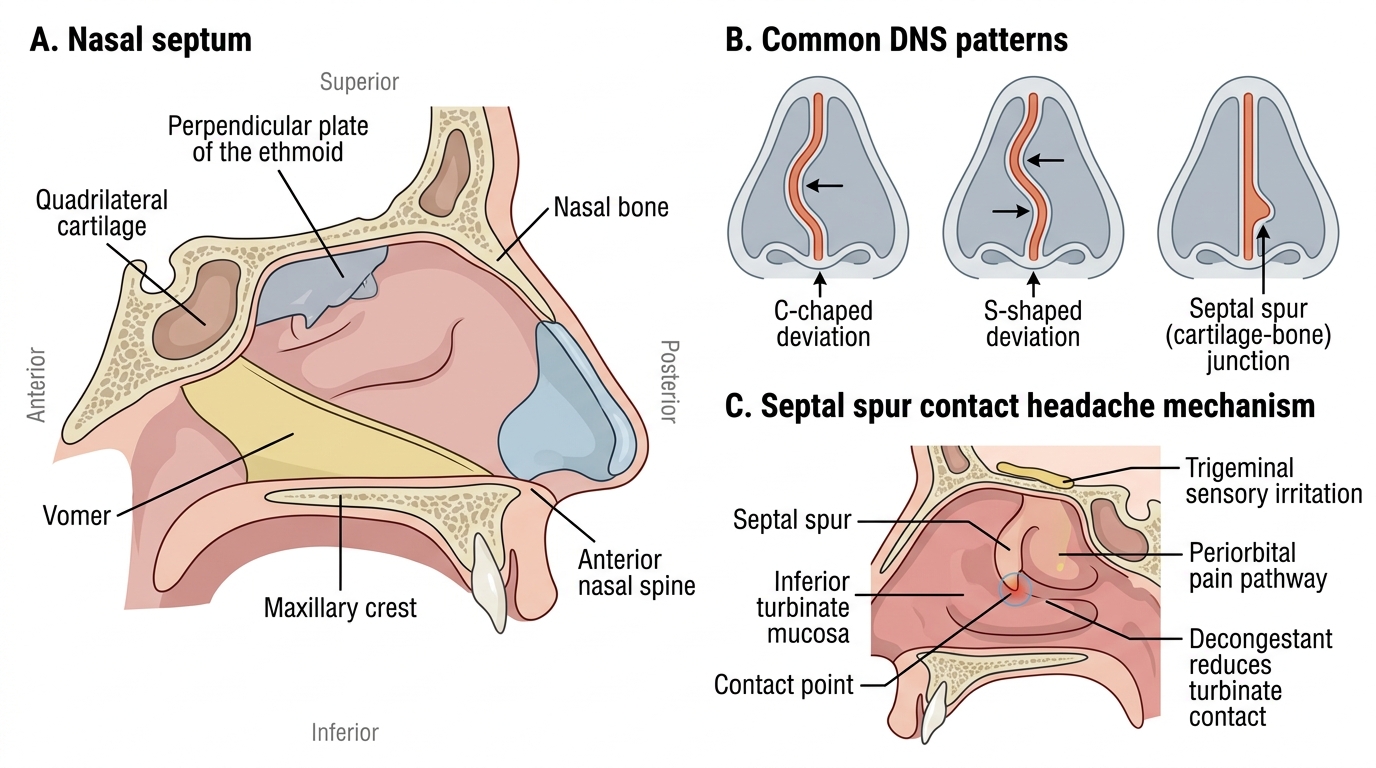
Recall from your anatomy sessions the structural components of the nasal septum. The septum is a midline partition made up of several bones and a cartilage meeting at specific junctions. The quadrilateral cartilage forms the large anterosuperior part — it is the flexible, mobile component of the septum and the part most involved in most deviations. Posterosuperiorly, the perpendicular plate of the ethmoid continues from the cribriform plate downward. Posteroinferiorly, the vomer forms the bony floor of the septum. The septum sits on the maxillary crest (a ridge on the floor of the nose formed by the maxilla and palatine bones) and articulates anteriorly with the nasal bones at the keystone area. Deviation or buckling can occur at any of these junctions, but the most clinically important site is the junction between the quadrilateral cartilage and the vomer/maxillary crest, where spurs most frequently form.
Clinical Features of Deviated Nasal Septum
The clinical presentation of DNS ranges from entirely asymptomatic — many deviations are incidental findings discovered on examination for other complaints — to severely symptomatic with multiple concurrent problems driven by a single anatomical abnormality. Understanding that one structural lesion can produce multiple seemingly unrelated symptoms (obstruction, epistaxis, headache, recurrent sinusitis) is the conceptual key to DNS history-taking.
The most common symptom is nasal obstruction, which in DNS is characteristically unilateral and constant (not intermittent or seasonal, which would suggest rhinitis). The obstruction is on the side to which the septum deviates — but paradoxically, the 'open' contralateral side may also become obstructed over time due to compensatory inferior turbinate hypertrophy, where the turbinate on the wider side enlarges to fill the expanded space. This bilateral functional obstruction from a structural unilateral lesion is a frequent source of diagnostic confusion.
Epistaxis in DNS arises from two mechanisms: (1) the deviated side has reduced airway area, so inspired air is faster-moving and drier over the nasal mucosa, causing mucosal desiccation and cracking over the deviation; (2) a septal spur — a sharp bony projection at the junction of cartilage and bone on the floor of the nasal septum — can directly traumatise the opposing inferior turbinate mucosa with breathing or minor touch.
Headache — often unrecognised as a nasal cause — occurs when a septal spur comes into contact with the lateral nasal wall (inferior or middle turbinate). This contact headache is called Sluder's neuralgia or vacuum headache, and presents as a dull, deep, periorbital or facial pain on the affected side that is relieved (temporarily) by anaesthetising the spur with topical lignocaine. It is frequently misdiagnosed as migraine or tension-type headache because it lacks the typical nasal discharge of sinusitis.
Recurrent sinusitis can result from DNS when the deviated septum narrows or obstructs the ostiomeatal complex (OMC) in the middle meatus, impairing drainage of the maxillary, frontal, and anterior ethmoid sinuses.
Snoring and sleep-disordered breathing may accompany severe DNS causing near-complete unilateral obstruction, as mouth breathing predisposes to pharyngeal turbulence during sleep.
Anatomy of the Nasal Septum and Types of Deviation
The nasal septum is a composite structure made up of four components — the quadrilateral cartilage, the perpendicular plate of the ethmoid, the vomer, and the maxillary crest — which meet at several articulations. Deviation can occur at any of these junctions, but the location and type of deviation determine both the clinical consequences and the surgical approach needed to correct it. Knowing the anatomy of the septum is essential to visualising what a surgeon is doing during septoplasty.
The quadrilateral (septal) cartilage is the largest and most anterior component. It is quadrilateral in shape and fills the anterosuperior portion of the septum. The anterior free edge of the quadrilateral cartilage forms the mobile membranous septum at the base of the nose. The cartilage is covered on each side by perichondrium, and deep to the perichondrium is the subperichondrial plane — the tissue plane that the surgeon enters during septoplasty to elevate the mucoperiosteal flap without injuring the septal mucosa.
Deviations are classified by shape and location:
- C-shaped deviation: the septum deviates as a smooth curve to one side — the entire nasal passage on that side is narrowed uniformly. The contralateral side is uniformly widened.
- S-shaped deviation: the septum deviates in opposite directions at different levels — upper part to one side, lower part to the other. This can cause bilateral obstruction at different levels — a subtle pattern that may be missed on casual rhinoscopy.
- Septal spur: a sharp angular bony or cartilaginous ridge at the junction of the cartilage and bone (usually at the cartilage-vomer junction or the maxillary crest). A spur projects laterally and may touch the inferior or middle turbinate — causing localised contact, bleeding point, and Sluder's headache.
- Caudal dislocation of the quadrilateral cartilage: the anterior free edge of the cartilage is displaced laterally out of the maxillary crest groove, visible externally as a nasal tip asymmetry or deflection and producing obstruction at the nasal vestibule.
Compensatory inferior turbinate hypertrophy develops on the contralateral (open) side of the deviation. The turbinate mucosa hypertrophies over months to years to fill the available space, reducing airflow on the nominally 'normal' side. Surgeons must address this during septoplasty — correcting only the deviation without addressing the compensatory turbinate hypertrophy may give an unsatisfactory result.
Nasal Septum Anatomy and Deviated Septum Patterns
SELF-CHECK
A patient with DNS and a prominent left-sided septal spur reports daily left-sided periorbital headache that is dull, non-pulsatile, not associated with nausea, and has not responded to sumatriptan. The headache is briefly relieved after a nasal decongestant spray. The most likely mechanism of this headache is:
A. Raised intracranial pressure from OMC obstruction causing ethmoid sinusitis
B. Contact between the septal spur and the left inferior turbinate mucosa causing Sluder's neuralgia
C. Trigeminal neuralgia triggered by mouth breathing
D. Migraine refractory to triptans requiring neurological re-evaluation
Reveal Answer
Answer: B. Contact between the septal spur and the left inferior turbinate mucosa causing Sluder's neuralgia
A dull, non-pulsatile, unilateral periorbital headache that is not associated with nausea or vomiting and is transiently relieved by nasal decongestants (which shrink the inferior turbinate, reducing contact with the spur) is characteristic of Sluder's neuralgia — a contact headache caused by a septal spur pressing against the inferior or middle turbinate mucosa. The diagnosis can be confirmed by applying topical lignocaine to the spur area, which temporarily abolishes the headache. This is frequently misdiagnosed as migraine because it is periorbital and unilateral; the key distinguishing features are its non-pulsatile quality, absence of autonomic features, and response to topical nasal anaesthetic.
Examination and Investigations
The examination of a patient with suspected DNS must be systematic and must not rely on anterior rhinoscopy alone, because posterior deviations and spurs can be missed without nasal endoscopy. A complete examination sequence generates the information needed to plan surgery safely and to determine whether CT imaging is required before operating. The examination also serves a medico-legal purpose: the extent and type of deviation documented pre-operatively forms the baseline against which post-operative outcomes are judged, and a surgeon who cannot articulate exactly what anatomical deformity they corrected is in a weak position if the patient is dissatisfied with the result. Beyond confirming DNS, the examination must actively look for co-existing pathology — polyps, turbinate hypertrophy, mucosal inflammation — that may need to be treated concurrently or that may explain symptoms that DNS alone cannot account for.
Anterior rhinoscopy (Thudichum's speculum + headlight) is the primary examination. Findings of DNS include:
- Deviated nasal septum: the septum is seen displaced from the midline, either smoothly (C-shape) or angularly, toward one side. The deviation may be cartilaginous (mobile, softer on palpation) or bony (firm, fixed).
- Septal spur: a sharp ridge at the septal floor, often touching the opposing inferior turbinate. The exact point of contact can be probed gently — this may reproduce the headache.
- Compensatory turbinate hypertrophy: the inferior turbinate on the contralateral side appears enlarged and fills the wider nasal passage.
- Mucosal changes: the mucosa over the convex aspect of the deviation may appear thin and dry; the opposing turbinate may show reactive hypertrophy or mucous pooling.
Nasal endoscopy (rigid 0° or 30°): extends the examination to the posterior nasal cavity, the middle meatus, and the nasopharynx. Essential for:
- Assessing the degree of OMC involvement by the deviation.
- Identifying a posterior spur not visible on anterior rhinoscopy.
- Ruling out co-existing polyps or masses.
CT scan of PNS (paranasal sinuses): indicated when:
- There is a history of recurrent sinusitis (to evaluate sinus involvement).
- Nasal endoscopy suggests OMC obstruction.
- Pre-operative planning for combined septoplasty + FESS.
- There is any suspicion of a co-existing mass or bony pathology.
CT is not required for straightforward DNS without sinusitis; anterior rhinoscopy alone is sufficient for an uncomplicated isolated deviation.
Rhinomanometry: objective airflow measurement; not routinely required but useful in medico-legal documentation or research settings.