Page 19 of 29
EN4.28 | Epistaxis — SDL Guide
Learning Objectives
- Elicit a structured history from a patient with epistaxis, identifying the site (anterior vs posterior), severity, and underlying cause
- Describe the vascular anatomy of the nasal septum and identify Little's area (Kiesselbach's plexus) as the commonest site of anterior epistaxis
- Identify the causes of epistaxis classified as local and systemic
- Demonstrate and describe the immediate first-aid management of anterior epistaxis
- Describe the principles of management for anterior and posterior epistaxis including cauterisation, anterior and posterior nasal packing, and surgical/interventional options
INSTRUCTIONS
Epistaxis (nosebleed) is a common ENT emergency encountered in every clinical setting — general practice, emergency departments, and ENT clinics. EN4.28 requires you to take a correct history, describe clinical features and investigations, and describe management principles. This module covers the critical anatomical distinction between anterior and posterior bleed sites, the emergency management sequence, and the red-flag causes that must not be missed.
References
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery. 8th ed. Chapter on Epistaxis (textbook)
- Hazarika P, Nayak DR, Balakrishnan R. Textbook of Ear, Nose and Throat — Head and Neck Surgery. Chapter on Epistaxis (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery. 8th ed. Vol 2: Rhinology — Epistaxis (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 72-year-old hypertensive man is brought to your emergency department at 2 AM with profuse bilateral nosebleeding that has not stopped despite 40 minutes of self-applied pressure. He is on aspirin and amlodipine. His blood pressure on arrival is 185/110 mmHg. The blood is running down his throat, not just out of the front of his nose, and he is spitting blood and feels faint. Anterior rhinoscopy shows no obvious anterior bleeding point — the bleeding appears to arise posteriorly. He is pale and anxious. What do you do immediately? And how does this presentation differ from the 8-year-old with a simple nosebleed who pinched her nose for 5 minutes and it stopped?
WHY THIS MATTERS
Epistaxis is the commonest ENT emergency, occurring at some point in approximately 60% of the general population, with 10% requiring medical attention. Most nosebleeds are anterior, self-limiting, and managed easily with simple first aid — but a minority are posterior, arterial, and life-threatening, requiring urgent specialist intervention. The ability to quickly classify a bleed as anterior or posterior, identify the anatomical site, and institute correct first-aid and escalation measures is a core clinical skill that every doctor needs, regardless of specialty. Missing a posterior bleed or applying incorrect first-aid (such as tilting the head back — which causes blood to run down the throat and risk aspiration) can have serious consequences. EN4.28 at the SH level requires you to demonstrate and describe this management.
RECALL
Recall the vascular supply to the nasal septum from your anatomy sessions. The nasal septum receives a rich anastomotic blood supply from multiple vessels of both the internal carotid and external carotid systems. On the anterior nasal septum, approximately 1 cm posterior to the mucocutaneous junction, five arteries converge and anastomose to form the Kiesselbach's plexus (also called Little's area): (1) the septal branch of the superior labial artery (branch of the facial artery → external carotid); (2) the anterior ethmoidal artery (branch of the ophthalmic artery → internal carotid); (3) the posterior ethmoidal artery (internal carotid system); (4) the greater palatine artery (maxillary artery → external carotid); (5) the sphenopalatine artery (maxillary artery → external carotid). The sphenopalatine artery — the terminal branch of the internal maxillary artery — is the main blood supply to the posterior nasal cavity and lateral nasal wall, branching into the posterior septal artery and the posterior lateral nasal artery. The plexus on the posterior inferior nasal septum is called Woodruff's plexus.
Clinical Presentation and Classification of Epistaxis
The clinical presentation of epistaxis must be immediately classified as anterior or posterior — this single determination drives the management pathway. The history and physical examination together establish not just the bleed site but also the severity, likely cause, and appropriate management escalation level.
Anterior epistaxis accounts for approximately 90% of all nosebleeds. The bleeding arises from Little's area (Kiesselbach's plexus) on the anteroinferior nasal septum. It presents as blood emerging from one or both nostrils in a forward direction — the patient notices blood dripping from the nose. It is usually self-limiting with simple first aid, common in children and young adults, and rarely causes haemodynamic compromise. Anterior rhinoscopy usually identifies the bleeding point.
Posterior epistaxis accounts for approximately 10% of nosebleeds but is responsible for the majority of serious and life-threatening cases. It arises from the sphenopalatine artery (or its branches) or from Woodruff's plexus on the posterior inferior nasal septum. It presents with blood running down the posterior pharynx (post-nasal bleed), the patient spitting or swallowing blood, and bilateral nasal bleeding. The patient often has no visible anterior bleeding point on rhinoscopy. Posterior epistaxis is more common in elderly patients with hypertension or arteriosclerosis, and may cause haemodynamically significant blood loss.
Key clinical distinguishing features:
- Anterior: blood from front of nose, unilateral, usually stops with pinching, responds to first aid, common in children/young adults.
- Posterior: blood running down throat, bilateral nasal bleeding, no visible anterior source on rhinoscopy, does not stop with anterior pinching, more common in elderly hypertensives.
History taking in epistaxis must include:
- Which nostril (unilateral vs bilateral).
- Direction of bleeding (forward or into throat).
- Duration and volume of blood loss (approximate cup measurement).
- Number of previous episodes and family history of bleeding disorder.
- Medications: anticoagulants (warfarin, direct oral anticoagulants — DOACs), antiplatelet agents (aspirin, clopidogrel), NSAIDs.
- Systemic diseases: hypertension (commonest associated systemic cause), coagulopathy, liver disease, renal failure, hereditary haemorrhagic telangiectasia (HHT/Osler-Weber-Rendu disease — recurrent epistaxis + telangiectasias on skin/mucosa + family history).
- Trauma, nasal picking (digital trauma — the commonest cause in children).
- Prior nasal surgery, DNS, foreign body.
Vascular Anatomy — Little's Area and Woodruff's Plexus
The vascular anatomy of the nasal septum is the foundation of epistaxis management — knowing which vessels feed each anatomical zone dictates both the examination approach and the surgical intervention required when packing fails. The nasal septum is one of the most richly vascularised mucosal surfaces in the body, receiving blood from both the internal carotid and external carotid systems. This dual blood supply is the reason why simple external carotid artery ligation is an inadequate treatment for severe anterior epistaxis — the anterior and posterior ethmoidal arteries arise from the ophthalmic artery (a branch of the internal carotid) and bypass the external carotid entirely. Understanding the anatomy of Little's area is therefore not merely a memorisation exercise but the direct clinical basis for why targeted endoscopic sphenopalatine artery ligation or ethmoidal artery ligation must be planned based on the bleed site rather than applied as a blanket surgical procedure.
Little's area (Kiesselbach's plexus) is the anastomotic vascular network on the anteroinferior nasal septum, approximately 1 cm behind the columella. It is formed by the convergence of five arterial branches:
1. Anterior ethmoidal artery — from the ophthalmic artery (internal carotid territory)
2. Posterior ethmoidal artery — from the ophthalmic artery (internal carotid territory)
3. Sphenopalatine artery — from the internal maxillary artery (external carotid territory)
4. Greater palatine artery — from the internal maxillary artery (external carotid territory)
5. Septal branch of the superior labial artery — from the facial artery (external carotid territory)
The dual internal carotid and external carotid supply to Little's area explains why ligation of the external carotid artery alone is insufficient to control severe anterior septal bleeding — the anterior and posterior ethmoidal arteries (internal carotid branches) must also be addressed.
Woodruff's plexus is the venous plexus on the posterior inferior nasal septum, at the junction of the septum and the inferior turbinate, near the posterior choana. It receives venous drainage from the sphenopalatine system and is the site of posterior septal bleeds in elderly patients. The bleeding is venous (oozing) rather than arterial, but the posterior location makes it inaccessible to simple anterior pressure.
The sphenopalatine artery — the terminal branch of the internal maxillary artery — enters the nose through the sphenopalatine foramen (located in the posterior middle meatus, above the posterior attachment of the middle turbinate). It is the dominant arterial supply to the posterior nasal cavity and is the target of sphenopalatine artery ligation or endoscopic cauterisation for refractory posterior epistaxis.
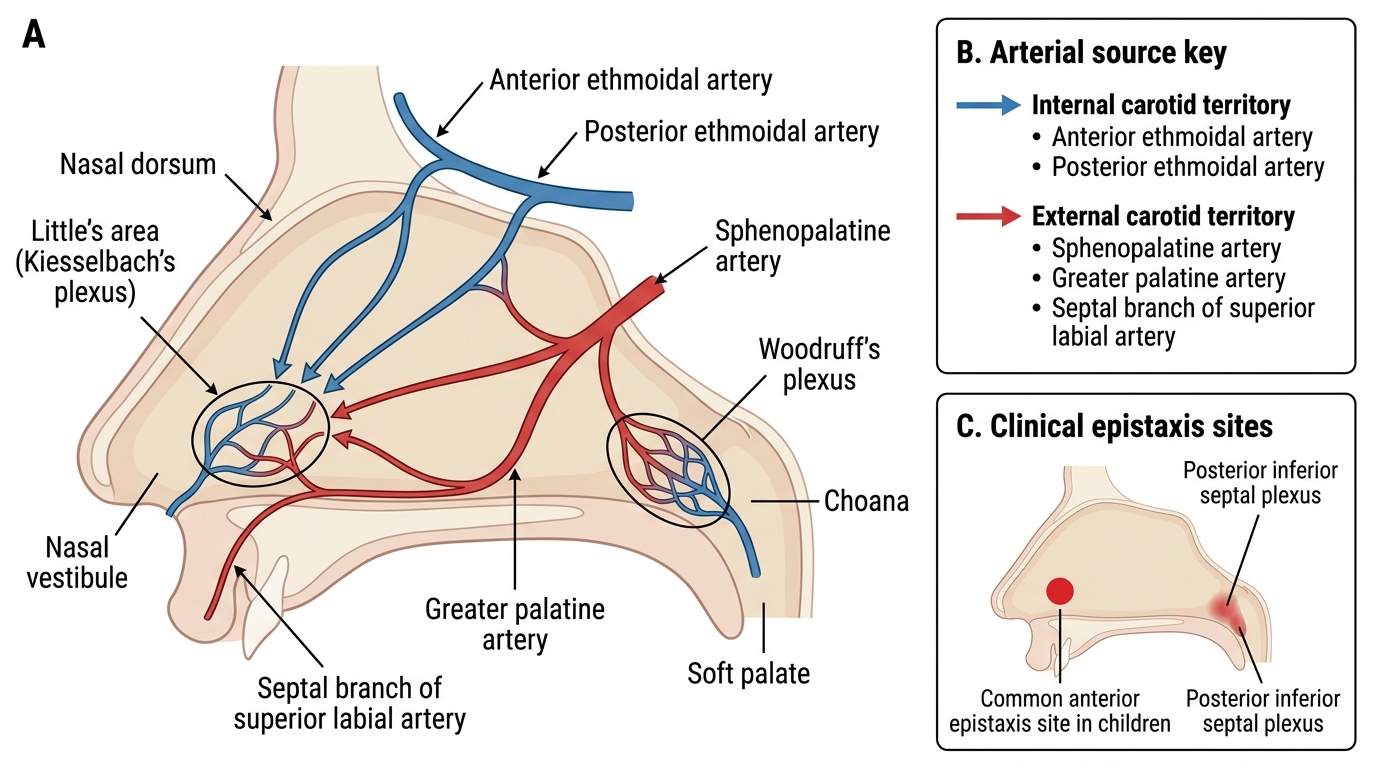
Vascular Plexuses of the Nasal Septum
SELF-CHECK
A 10-year-old girl has her third episode of right-sided nosebleed in a month. Each episode starts with digital nose-picking and stops within 5 minutes of pinching the nose just below the nasal bones. The bleed is from the right nasal cavity only, and blood flows forward from the nostril. The most likely bleeding site is:
A. The right posterior lateral nasal wall — sphenopalatine artery territory
B. Little's area (Kiesselbach's plexus) on the right anteroinferior nasal septum
C. Woodruff's plexus on the right posterior inferior nasal septum
D. The right ethmoid sinuses — anterior ethmoidal artery
Reveal Answer
Answer: B. Little's area (Kiesselbach's plexus) on the right anteroinferior nasal septum
Anterior epistaxis from Little's area (Kiesselbach's plexus) is by far the commonest site of nosebleed, accounting for ~90% of all epistaxis. In children, it is almost always caused by digital trauma (nose-picking), and the combination of unilateral, forward-flowing blood, stopping easily with anterior pinching, and recurrence with picking is pathognomonic. Little's area is on the anteroinferior nasal septum — the most exposed part of the nasal mucosa — and its rich anastomotic plexus (five vessels converging) is easily traumatised by fingers, drying, or minor mucosal disease. Posterior bleeds (sphenopalatine, Woodruff's) occur in elderly hypertensives and do not stop with anterior pinching.
Examination and Investigations
The examination of a patient with active epistaxis follows a sequence determined by the urgency: haemodynamic assessment first, then localisation of the bleeding site, then assessment for underlying causes. The airway, breathing, and circulation (ABC) principles apply — a patient with severe posterior epistaxis may be in haemorrhagic shock and swallowing large volumes of blood that risk aspiration. The common error in epistaxis examination is to go straight to looking in the nose before assessing the patient's haemodynamic state — in a patient who is pale, tachycardic, and confused, IV access and cross-match come before the nasal speculum. Equally, the blood pressure must be measured in every adult with epistaxis: hypertension is both the commonest systemic association with severe posterior bleeding and a modifiable factor whose control directly reduces the bleed.
Immediate assessment:
- Haemodynamic status: pulse, blood pressure, capillary refill, pallor, restlessness (signs of hypovolaemia). If haemodynamically compromised: IV access, fluid resuscitation, urgent cross-match.
- Blood pressure: hypertension (sustained BP >140/90) is the most important systemic association with severe posterior epistaxis in adults — treat the hypertension as part of the management.
- Airway: is the patient swallowing or spitting blood? Can they maintain their own airway? Position upright and leaning slightly forward.
Local examination:
- Anterior rhinoscopy with headlight: examine the nasal septum for a visible bleeding point in Little's area — appears as a small bright red eroded or crusted area on the anterior septum. If no anterior source is found, suspect posterior bleed.
- Post-nasal space examination / nasopharyngoscopy: direct visualisation of the nasopharynx with a flexible endoscope to confirm posterior bleeding.
Investigations:
- Full blood count (FBC): haemoglobin (to assess blood loss), platelet count (thrombocytopaenia).
- Coagulation screen: PT, APTT, INR — in patients on anticoagulants, with liver disease, or with recurrent unexplained bleeding.
- Blood group and cross-match: if blood transfusion may be required.
- Nasal endoscopy: to identify the site, plan cauterisation.
- CT angiography/MRI: if a vascular lesion (JNA, aneurysm) is suspected as the cause — never proceed to biopsy of a suspected vascular nasopharyngeal mass without imaging first.
- Bleeding time, PFA-100: if hereditary haemorrhagic telangiectasia (HHT) or von Willebrand disease is suspected.