Page 13 of 29
EN4.25 | Vasomotor Rhinitis — SDL Guide
Learning Objectives
- Elicit a structured history from a patient with vasomotor rhinitis, distinguishing it from allergic rhinitis and other rhinitis types
- Describe the pathophysiology of vasomotor rhinitis as autonomic nasal hyperreactivity
- Describe the clinical features and characteristic triggers of vasomotor rhinitis
- Choose appropriate investigations and state why allergy tests are negative
- Describe the principles of management including avoidance, intranasal corticosteroids, intranasal anticholinergics, and surgical options
INSTRUCTIONS
Vasomotor rhinitis is the second most common cause of chronic rhinitis after allergic rhinitis, yet it is frequently misdiagnosed as allergic rhinitis and treated ineffectively with antihistamines and allergy tests that yield no useful information. EN4.25 requires you to take a correct history, describe clinical features, choose appropriate investigations, and describe management. Understanding vasomotor rhinitis requires understanding what it is NOT — it is not IgE-mediated, not seasonal, and not allergen-driven — and what it IS: a disorder of autonomic regulation of the nasal mucosal vasculature.
References
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery. 8th ed. Chapter on Vasomotor Rhinitis (textbook)
- Hazarika P, Nayak DR, Balakrishnan R. Textbook of Ear, Nose and Throat — Head and Neck Surgery. Chapter on Rhinitis (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery. 8th ed. Vol 2: Rhinology — Non-allergic Rhinitis (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 38-year-old teacher presents with a 6-year history of bilateral nasal obstruction, runny nose, and post-nasal drip. Symptoms are worst when she enters an air-conditioned room from outside, when she smells perfume or cigarette smoke, and when she drinks a glass of wine. There is no sneezing, no eye symptoms, and no seasonal variation. Her symptoms are present every day of the year. Her general practitioner ordered a skin prick test (negative to all 20 allergens) and told her 'nothing is wrong.' She has tried antihistamines — no benefit. She is frustrated and wants an answer. What is wrong with her? Why did the allergy test come back negative? And what treatment will actually help?
WHY THIS MATTERS
Vasomotor rhinitis (non-allergic rhinitis, idiopathic rhinitis) accounts for approximately one-third of all chronic rhinitis cases in adults, making it a significant public health burden. Unlike allergic rhinitis, there is no identifiable immune mechanism, no allergy test positive, and no single curative treatment. It is a diagnosis of exclusion — made after allergic, infectious, drug-induced, and structural causes are ruled out. Understanding vasomotor rhinitis is clinically important because it is frequently mismanaged: patients undergo repeated allergy workups, receive antihistamines that do not help, or are reassured that 'nothing is wrong' when in fact their quality of life is significantly impaired. Recognising the clinical pattern and explaining its autonomic basis is the foundation of effective management.
RECALL
Recall from your physiology sessions the autonomic control of the nasal mucosa. The inferior turbinate mucosa contains a rich submucosal vascular plexus of venous sinusoids that can engorge (congestion) or decongest depending on autonomic tone. Parasympathetic stimulation (via the vidian nerve, carrying secretomotor fibres from the superior salivatory nucleus via the pterygopalatine ganglion to the nasal glands and vessels) causes vasodilation of turbinate sinusoids and increased nasal gland secretion — producing nasal congestion and rhinorrhoea. Sympathetic stimulation causes vasoconstriction and decongestion. The physiological nasal cycle alternates between these states every 2–6 hours. In vasomotor rhinitis, this autonomic balance is dysregulated — the nasal mucosa is chronically hyper-responsive to stimuli that do not affect normal noses, with the parasympathetic system predominating or reacting excessively to trivial triggers.
Clinical Presentation of Vasomotor Rhinitis
Vasomotor rhinitis has a highly characteristic clinical presentation that can be distinguished from allergic rhinitis by taking a careful history focused on the pattern of symptoms, the nature of triggers, the presence or absence of itch and sneezing, and the seasonality. The defining feature is that the nasal mucosa reacts excessively to non-immunological, non-allergenic stimuli — environmental physical and chemical triggers that do not cause nasal symptoms in normal individuals.
The predominant symptoms of vasomotor rhinitis are nasal obstruction (bilateral, alternating or constant) and rhinorrhoea (which may be watery or mucoid). These are the same two symptoms found in allergic rhinitis — the critical distinguishing features are what is absent and what triggers the symptoms:
What is absent (distinguishes from allergic rhinitis):
- No or minimal sneezing (occasional mild sneezing may occur, but not the violent paroxysmal 10–20 sneeze attacks of allergic rhinitis).
- No nasal itch (nasal itch is histamine-driven and a cardinal feature of allergic rhinitis — its absence points away from an IgE-mediated mechanism).
- No eye symptoms (no allergic conjunctivitis — red itchy watery eyes).
- No seasonal variation.
- No allergen-specific triggers (no correlation with pollen season, no pet-specific onset).
Characteristic triggers of vasomotor rhinitis:
- Temperature and humidity changes: entering an air-conditioned room from a warm outdoor environment; stepping outside from central heating into cold air; monsoon weather changes. These stimuli activate the autonomic response.
- Strong smells and chemical irritants: perfumes, deodorants, paint fumes, smoke, petrol, cleaning agents, strong food odours.
- Alcohol: alcohol is a direct vasodilator — wine, particularly red wine, triggers nasal congestion in vasomotor rhinitis patients.
- Emotional and psychological triggers: stress, anxiety, emotional upset.
- Exercise: exertion can trigger vasomotor symptoms in some patients.
- Hormonal changes: vasomotor rhinitis often worsens during pregnancy (rhinitis of pregnancy) due to oestrogen-mediated effects on nasal vasculature, and around the menstrual cycle.
- Spicy food and hot beverages: the so-called gustatory rhinitis variant — eating hot or spicy food triggers profuse watery rhinorrhoea via a vagally mediated reflex.
The pattern is perennial (year-round), present every day, and not linked to any specific pollen season or identifiable allergen. Patients often describe their nose as 'always running' or 'always blocked' with no obvious cause.
Pathophysiology of Vasomotor Rhinitis
The pathophysiology of vasomotor rhinitis is not fully understood, but the central mechanism is an exaggerated, non-immune autonomic response of the nasal mucosa to stimuli that are normally sub-threshold. The autonomic imbalance theory holds that in vasomotor rhinitis, the parasympathetic tone of the nasal mucosa is chronically increased or the threshold for triggering a parasympathetic response is dramatically lowered.
The nasal mucosa is supplied by the vidian nerve (nerve of the pterygoid canal), which carries both parasympathetic secretomotor fibres (from the superior salivatory nucleus via the pterygopalatine ganglion) and sympathetic vasoconstrictor fibres. In normal individuals, these two systems are balanced — a mild cool breeze causes mild transient congestion followed by rapid recovery. In vasomotor rhinitis, the same mild stimulus causes a disproportionate and prolonged parasympathetic response: vasodilatation of the erectile turbinate sinusoids (congestion), increased nasal gland secretion (rhinorrhoea), and hypersensitive sensory nerve responses.
The neuropeptide hypothesis proposes that vasomotor rhinitis involves dysregulation of sensory neuropeptides — particularly substance P and vasoactive intestinal peptide (VIP) — in the nasal mucosa. These neuropeptides, released from sensory nerve endings, act as neurogenic inflammatory mediators, causing vasodilation and glandular secretion. Abnormally elevated neuropeptide levels or reduced enzyme degradation of these peptides may account for the exaggerated response. This is why intranasal anticholinergics (ipratropium bromide) are effective in the rhinorrhoea-dominant subtype of vasomotor rhinitis — they block the parasympathetic (muscarinic) receptors on nasal glands, reducing secretion.
Vasomotor rhinitis is classified into two main subtypes based on dominant symptom:
1. Rhinorrhoea-dominant: watery or mucoid anterior nasal discharge and post-nasal drip predominate; responds better to intranasal anticholinergics.
2. Obstruction-dominant: bilateral nasal congestion predominates; responds better to intranasal corticosteroids and decongestants.
Many patients have a mixed pattern. The subtype classification guides pharmacotherapy selection.
SELF-CHECK
A 45-year-old man reports profuse watery nasal discharge and nasal congestion every time he eats a hot spicy meal or drinks hot tea. There is no sneezing, no nasal itch, no eye symptoms, and skin prick testing is negative. This is an example of:
A. Intermittent allergic rhinitis triggered by food allergens
B. Gustatory rhinitis — a subtype of vasomotor rhinitis triggered by spicy food or hot beverages via a vagal reflex
C. Chronic rhinosinusitis exacerbated by dietary inflammatory triggers
D. Non-allergic rhinitis with eosinophilia syndrome (NARES)
Reveal Answer
Answer: B. Gustatory rhinitis — a subtype of vasomotor rhinitis triggered by spicy food or hot beverages via a vagal reflex
Gustatory rhinitis is a well-recognised subtype of vasomotor (non-allergic) rhinitis in which eating hot or spicy food triggers profuse watery anterior rhinorrhoea and nasal congestion via a vagally mediated (cholinergic) reflex. The mechanism is a direct parasympathetic-secretomotor response to sensory stimulation of the oral and pharyngeal mucosa — not an allergen-specific IgE reaction. The negative SPT confirms the absence of IgE-mediated sensitisation. NARES would show eosinophilia on nasal smear (it is negative here). Gustatory rhinitis responds well to prophylactic intranasal ipratropium bromide (anticholinergic) used before meals.
Examination and Investigations
The examination and investigation of a patient with vasomotor rhinitis are primarily directed toward excluding other causes of chronic rhinitis rather than finding positive diagnostic features of vasomotor rhinitis itself. The diagnosis is one of exclusion — confirmed by the clinical history, the absence of allergic features, and negative allergy investigations. A positive examination finding or a positive investigation suggests a different or co-existing diagnosis.
Anterior rhinoscopy: The inferior turbinates appear hypertrophied and erythematous or congested — typically more red-pink and fleshy in appearance than the pale, boggy, bluish-white turbinates of allergic rhinitis. The mucosa is not as pale and oedematous as in allergy. Nasal secretions may be watery or mucoid. There are no polyps (absence of polyps distinguishes vasomotor rhinitis from ethmoidal polyposis, though polyps can coexist). The septum may be deviated.
Investigations — all negative by definition in pure vasomotor rhinitis:
- Skin prick test (SPT): NEGATIVE to all common aeroallergens — this is the key finding that excludes allergic rhinitis. The clinical diagnosis of vasomotor rhinitis requires a negative SPT or negative serum-specific IgE.
- Serum-specific IgE: negative.
- Nasal cytology (nasal smear): in vasomotor rhinitis, the smear shows predominantly neutrophils or a non-specific cellular pattern — there is NO eosinophilia (eosinophilia on nasal smear would suggest NARES — non-allergic rhinitis with eosinophilia syndrome, a distinct entity that also lacks positive allergy tests but has eosinophilic mucosal inflammation and responds better to INCS).
- CT PNS: normal or shows only inferior turbinate hypertrophy; no sinus disease. Indicated if sinusitis is clinically suspected.
- Rhinomanometry: may show increased nasal resistance; not required for routine diagnosis.
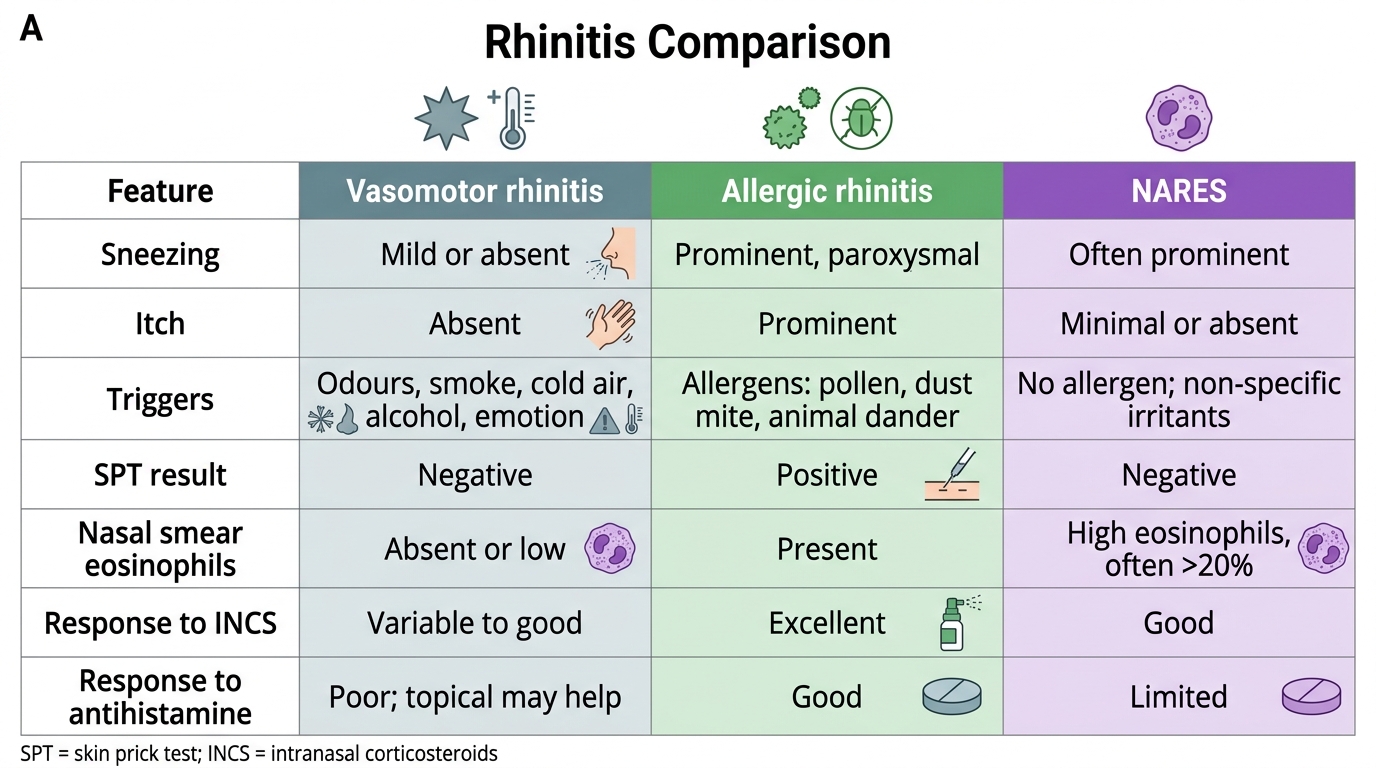
Vasomotor Rhinitis vs Allergic Rhinitis vs NARES