Page 5 of 15
EN3.2 | Diagnostic Nasal Endoscopy — SDL Guide
Learning Objectives
- State the clinical indications for diagnostic nasal endoscopy and explain why it supersedes anterior rhinoscopy and plain radiographs for nasal and sinus assessment
- Identify the types of nasal endoscope (rigid vs flexible, 0°/30°/70°) and explain the Hopkins rod lens system and coaxial illumination principle
- Describe the pharmacological preparation of the nasal mucosa before DNE including decongestant and topical anaesthetic agents
- Describe the systematic three-pass endoscopic survey technique, naming the anatomical structures examined at each pass
- Interpret key diagnostic nasal endoscopy findings including normal anatomy, bilateral ethmoidal nasal polyps, unilateral antrochoanal polyp, ostiomeatal complex disease, adenoid hypertrophy, and nasopharyngeal mass
INSTRUCTIONS
Diagnostic nasal endoscopy (DNE) transformed the clinical assessment and surgical management of nasal and paranasal sinus disease from the 1970s onward. Before the Hopkins rod endoscope, surgeons examined the nasal cavity with a simple nasal speculum and a headlight, able to see only the anterior third of the cavity and unable to inspect the middle meatus, the ostiomeatal complex, or the nasopharynx without radiographs. DNE changed this completely — a rigid 4 mm telescope, passed systematically through the three nasal passes, now allows direct inspection of every clinically relevant nasal structure in an outpatient setting. The NMC EN3.2 competency requires you to observe and describe the indications and steps of DNE; as a final-year student your ability to interpret what is seen during this procedure and communicate findings accurately is the practical objective.
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th ed., Ch. 15: Nasal Endoscopy; Ch. 16: Functional Endoscopic Sinus Surgery (textbook)
- Hazarika P — Textbook of Ear, Nose and Throat, 3rd ed., Ch. 8: Endoscopy of the Nose and Paranasal Sinuses (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Vol. 2: Rhinology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 32-year-old woman presents with a two-year history of bilateral nasal obstruction, loss of smell, and recurrent rhinosinusitis that has not responded to three courses of antibiotics and multiple steroid nasal sprays. Her GP has sent her with a plain X-ray of her sinuses, which shows 'haziness in both maxillary sinuses.' You perform anterior rhinoscopy with a Thudicum speculum: you can see the anterior septum and the anterior ends of the inferior turbinates, but nothing beyond the first centimetre of the nasal cavity. The ENT surgeon picks up a 0° rigid nasal endoscope, applies decongestant, and within three minutes has surveyed the nasal floor, the middle meatus, and the nasopharynx. She sees bilateral grey, grape-like masses filling the middle meatus on both sides. 'Ethmoidal polyps — grade 2 bilateral,' she says. 'We need FESS.' The plain X-ray told you about opacity; the endoscope showed you what was causing it and exactly where it was. How does this systematic three-pass examination make that possible?
WHY THIS MATTERS
Diagnostic nasal endoscopy is now the standard of care for the assessment of nasal and sinus disease in any ENT outpatient department. It is performed routinely for chronic rhinosinusitis, nasal polyps, recurrent epistaxis, unexplained unilateral nasal symptoms, post-operative surveillance after functional endoscopic sinus surgery (FESS), and the evaluation of any nasopharyngeal mass. As a final-year MBBS student, you will observe DNE during your ENT clinical posting and are expected under EN3.2 to describe its indications and procedural steps. More practically, your ability to distinguish between a bilateral ethmoidal polyp and a unilateral antrochoanal polyp on endoscopy — and to understand why a unilateral nasal mass in an adolescent male triggers a 'do not biopsy' response — is directly relevant to primary-care triage. Patients with unilateral nasal symptoms, progressive obstruction, and epistaxis need ENT referral, not repeated antibiotic courses.
RECALL
Recall from your anatomy sessions that the nasal cavity on each side contains three turbinates projecting from the lateral wall: the inferior turbinate (largest, most anterior, most clinically visible), the middle turbinate (the key landmark for endoscopic surgery), and the superior turbinate (smallest, posteriorly placed). Under the middle turbinate lies the middle meatus, which receives drainage from the anterior ethmoidal sinuses, the maxillary sinus, and the frontal sinus via the ostiomeatal complex (OMC) — a functional drainage unit comprising the maxillary ostium, the infundibulum, the hiatus semilunaris, and the middle meatus. Blockage of the OMC is the mechanism underlying most maxillary and frontal sinusitis. The sphenoethmoid recess, located between the superior turbinate and the nasal septum, drains the sphenoid sinus and the posterior ethmoid air cells. The nasopharynx is the space posterior to the choana (posterior nasal aperture), above the level of the soft palate; the adenoid (pharyngeal tonsil) occupies its roof and posterior wall and is prominent in children up to puberty.
Clinical Indications for Diagnostic Nasal Endoscopy
Anterior rhinoscopy with a Thudicum speculum and a headlight allows inspection of only the anterior third of the nasal cavity — the anterior septum, the anterior ends of the inferior and middle turbinates, and the nasal vestibule. The key diagnostic areas of the nasal cavity — the middle meatus, the ostiomeatal complex, the sphenoethmoid recess, the posterior choana, and the nasopharynx — are completely invisible to anterior rhinoscopy. Plain radiographs of the paranasal sinuses show opacification but cannot distinguish between mucosal thickening, polyp, pus, tumour, or fluid. Diagnostic nasal endoscopy (DNE) overcomes both limitations by allowing direct, magnified, illuminated inspection of the entire nasal cavity and nasopharynx through the nostril, under local anaesthesia in the outpatient setting.
The principal clinical indications for DNE are:
Chronic rhinosinusitis (CRS) and nasal polyps:
- Assessment of bilateral nasal obstruction and anosmia not responding to medical treatment — endoscopy visualises whether the middle meatus contains polyp, oedematous mucosa, or purulent discharge
- Staging of nasal polyp extent (Grades 1–3 based on progression from middle meatus to obstruction of the nostril)
- Pre-operative assessment before functional endoscopic sinus surgery (FESS)
- Post-operative surveillance after FESS — endoscopy confirms healing, detects recurrent disease or synechia
Epistaxis:
- Localisation of the bleeding point when anterior rhinoscopy is inconclusive — allows identification of Little's area, Woodruff's plexus (posterior), or a vascular lesion
- Assessment for underlying cause including nasopharyngeal angiofibroma in adolescent males
Unilateral nasal symptoms:
- Any patient with unilateral nasal obstruction, discharge, or bleeding must have endoscopy to exclude unilateral polyp (antrochoanal), inverted papilloma, or malignancy — unilateral symptoms in the nose always raise suspicion of a structural lesion
Other indications:
- Assessment of adenoid hypertrophy in children (endoscopic visualisation of the nasopharynx)
- Evaluation of a suspected nasopharyngeal mass — biopsy under endoscopic guidance
- Assessment of post-nasal discharge (posterior drip) source
- Foreign body localisation in the nasal cavity or nasopharynx
Viewing Angles of Rigid Nasal Endoscopes
The Nasal Endoscope: Instrument, Optics, and Angles
The rigid nasal endoscope used for DNE in ENT outpatient departments worldwide is based on the Hopkins rod lens system, developed by Harold Hopkins in the 1960s and commercialised by Karl Storz. Understanding the optical principle explains why the image quality from these instruments is dramatically superior to older lens-based telescopes, and why the instrument is fragile and expensive.
Hopkins rod lens system: In a conventional lens telescope, a series of small glass lenses separated by long air spaces transmits the image. Because glass transmits light better than air, inverting this arrangement — using long glass rods separated by short air spaces — results in far superior light transmission, brightness, resolution, and colour fidelity. The Hopkins rod lens endoscope transmits approximately four times more light than a conventional lens telescope of the same diameter. This brightness is what allows the surgeon to see clearly into deep recesses of the nasal cavity without an external light source.
Light source and cable: An external halogen or xenon cold-light source (150–300 watts) connects to the endoscope via a fibre-optic light cable, delivering intense cold illumination to the distal tip. Cold light (fibre-optic) is essential — direct tungsten illumination at the tip generates heat and would burn the nasal mucosa.
Endoscope diameters: The standard adult nasal endoscope is 4 mm in diameter; a 2.7 mm instrument is used for children or narrow nasal passages. A camera system can be attached to the eyepiece for display on a monitor and recording, allowing the patient to see the findings and for documentation and teaching.
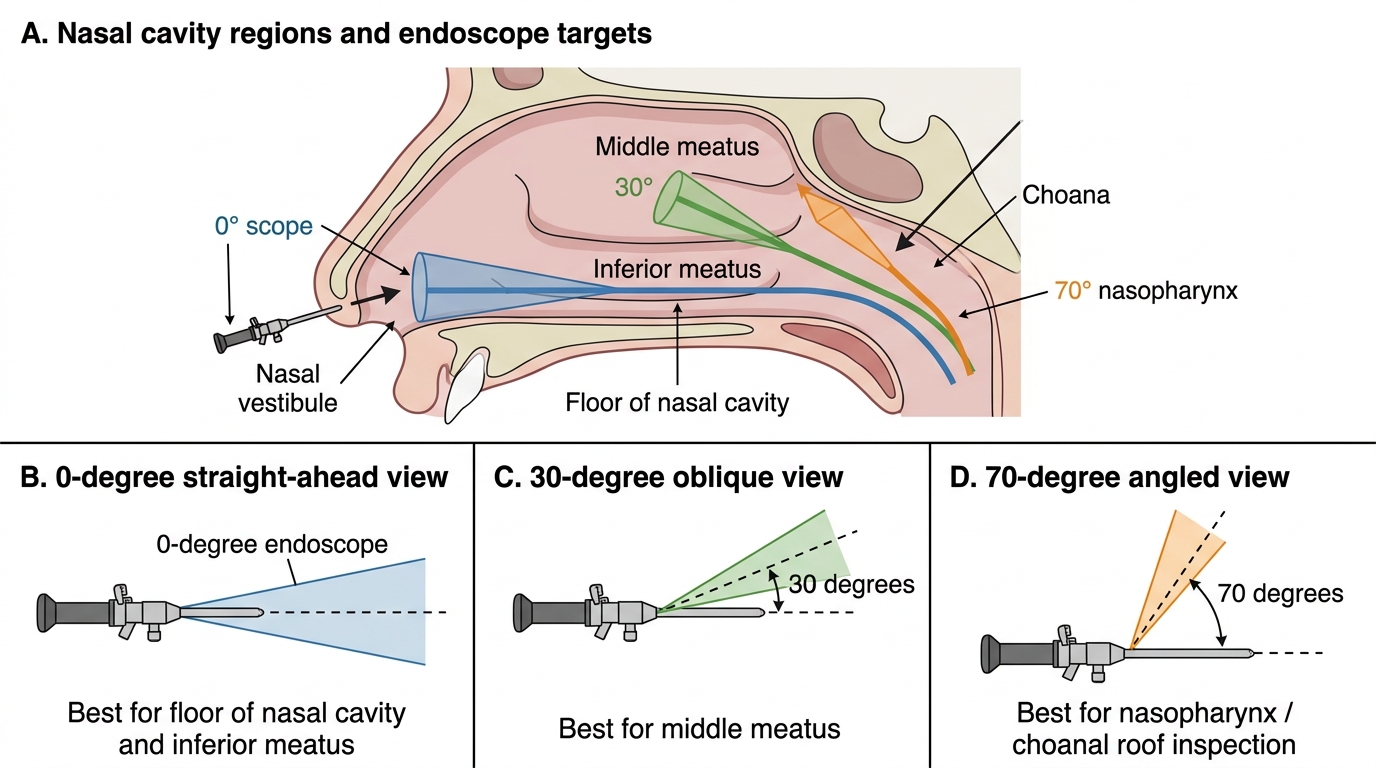
Viewing angles — the three standard angles:
- 0° (straight-forward view): The line of sight is along the long axis of the scope. Used for the initial survey of the nasal floor, inferior meatus, and nasopharynx (Pass 1). Provides the most intuitive orientation and is the standard starting angle.
- 30° (angled view): The line of sight is angled 30° from the scope axis. Used to look 'around the corner' of the middle turbinate into the middle meatus and ostiomeatal complex (Pass 2) — structures that are hidden directly behind the middle turbinate on a 0° view.
- 70° (wide-angle): The line of sight is nearly perpendicular to the scope axis. Used to inspect the roof of the nasopharynx, the choana, and in some configurations the maxillary antrum through the middle meatus after widening the ostium.
Rigid vs flexible endoscopes: The rigid Hopkins rod endoscope is used for diagnostic nasal endoscopy in adults because of its superior image quality and the ability to take biopsies through an adjacent instrument. Flexible nasopharyngoscopes are used in patients who cannot tolerate the rigid instrument (children, gag-reflex patients, hypersensitive airways) and for laryngoscopy (covered in EN3.3).
Preparation: Decongestion and Local Anaesthesia
Adequate preparation of the nasal mucosa before endoscopy is not optional — it is a prerequisite for a successful, comfortable, and diagnostically informative examination. The nasal mucosa is richly vascular and highly sensitive. Without decongestant, the turbinates remain engorged and obscure the middle meatus; without topical anaesthetic, the procedure is painful and the patient's eye-watering and sneezing prevent a systematic examination. Adequate preparation converts a difficult, limited procedure into a comfortable and complete one. The preparation step is itself an observation during your clinical posting — noting the agents used, their timing, and the method of application is part of the EN3.2 competency.
Step 1 — Decongestant:
Apply xylometazoline 0.1% or oxymetazoline 0.05% nasal spray to both nasal cavities. Wait 10 minutes for full mucosal shrinkage. The inferior and middle turbinates reduce in size and the airway widens, creating the space needed to pass the endoscope comfortably. Decongestant also reduces mucosal bleeding during the procedure — important when an instrument is being manoeuvred in a narrow cavity.
Step 2 — Topical local anaesthetic:
Apply 4% lignocaine spray to both nasal cavities, directing the spray toward the inferior and middle turbinates, or apply 5% cocaine-soaked cotton pledgets to the middle meatus region. Wait 5 minutes for anaesthesia. Cocaine has the combined advantage of being both a local anaesthetic and a potent vasoconstrictor and is frequently used in this context; however, it is a controlled drug requiring careful documentation and is not universally available. Lignocaine spray is the more common outpatient preparation.
Patient consent and explanation: Before beginning, explain to the patient that they will feel the cold of the decongestant spray, some mild pressure as the scope passes, and that the procedure takes approximately 5–10 minutes. This significantly reduces anxiety-induced breath-holding and sneezing. In children under 10 years, DNE under general anaesthesia (in theatre) is usually preferred over a clinic awake procedure.
SELF-CHECK
A 28-year-old man has chronic nasal obstruction and recurrent maxillary sinusitis. Before diagnostic nasal endoscopy, xylometazoline 0.1% nasal spray is applied and the patient waits 10 minutes. The primary purpose of this step is:
A. To sterilise the nasal cavity before introducing the endoscope
B. To shrink the nasal turbinate mucosa and widen the airway for endoscope passage and middle meatus visualisation
C. To provide complete local anaesthesia of the nasal mucosa before endoscopy
D. To dislodge nasal polyps from the middle meatus before the endoscopic survey
Reveal Answer
Answer: B. To shrink the nasal turbinate mucosa and widen the airway for endoscope passage and middle meatus visualisation
Xylometazoline is an alpha-adrenergic vasoconstrictor that causes mucosal shrinkage (decongestion) of the turbinates, widening the nasal airway and exposing the middle meatus — the key diagnostic zone. Without decongestion, engorged turbinates obstruct passage of the endoscope and hide the middle meatus. It is not a local anaesthetic (lignocaine or cocaine provides anaesthesia), does not sterilise the cavity, and does not displace polyps. However, it does reduce mucosal bleeding during the procedure.