Page 14 of 21
EN4.34 | Granulomatous Diseases of Nose — SDL Guide
Learning Objectives
- Describe the clinical features of the major granulomatous diseases affecting the nose, including tuberculosis, rhinoscleroma, rhinosporidiosis, granulomatosis with polyangiitis (GPA), leprosy, syphilis, and sarcoidosis
- Choose appropriate investigations — particularly biopsy and histopathology — for the diagnosis of granulomatous nasal disease
- Distinguish granulomatous nasal diseases from each other and from inflammatory and neoplastic conditions
- Describe the principles of management for the major granulomatous nasal diseases
INSTRUCTIONS
Granulomatous diseases of the nose form a distinctive clinical group characterised by chronic nasal obstruction, crusting, epistaxis, and, in advanced cases, septal perforation and saddle-nose deformity. In India, the differential is broad: tuberculosis, leprosy, syphilis, rhinoscleroma, and rhinosporidiosis all have significant prevalence, while granulomatosis with polyangiitis (Wegener's) and sarcoidosis represent important autoimmune causes. The unifying clinical clue is chronic nasal pathology that does not respond to standard antibiotic treatment — in such a patient, biopsy and histopathology are the central investigation. This module covers the clinical features, diagnostic approach, and management principles of each condition.
References
- Dhingra PL — Diseases of Ear, Nose & Throat, 7th ed., Ch 24-26 (textbook)
- Hazarika P — Textbook of ENT and Head & Neck Surgery, 3rd ed., Ch 15-17 (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed., Vol 2, Rhinology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old male agricultural worker from rural Tamil Nadu presents with a 2-year history of progressive bilateral nasal obstruction, foul-smelling bloody crusting in the nose, and recurrent epistaxis. He has lost most of his sense of smell. On anterior rhinoscopy you see dark, adherent crusts throughout the nasal cavity, a perforation in the cartilaginous nasal septum, and a pale, polypoid mass in the right nasal cavity with a 'strawberry' surface studded with white spots. His chest X-ray is normal. Nasal swab culture shows no growth on routine media. What is the most likely diagnosis, and what is the single most important investigation that will confirm it?
WHY THIS MATTERS
Granulomatous diseases of the nose are clinically important for three reasons that are specific to the Indian context. First, many of these diseases — tuberculosis, leprosy, syphilis, rhinoscleroma, and rhinosporidiosis — have significantly higher prevalence in India than in high-income countries, making them a necessary part of the ENT differential diagnosis that would not rank as highly in a Western setting. Second, these conditions are chronically progressive and irreversible if not diagnosed and treated appropriately — a patient with undiagnosed GPA can lose their airway, their kidneys, and their life within months; a patient with undiagnosed nasal TB continues to transmit disease. Third, the diagnostic approach for all granulomatous diseases converges on a single central investigation — biopsy and histopathology — and the student who understands this principle can navigate any granulomatous nasal diagnosis regardless of which specific entity it turns out to be. The competency EN4.34 (KH level, K domain) requires knowledge of clinical features, investigation, and management across this group.
RECALL
Recall from your pathology teaching that a granuloma is a specific type of chronic inflammation characterised by collections of activated macrophages — called epithelioid cells — sometimes fusing to form multinucleate giant cells (Langhans giant cells in tuberculosis, foreign body giant cells in foreign body reactions). Granuloma formation is the immune response to antigens that cannot be eliminated by acute inflammatory mechanisms — typically mycobacteria, fungi, parasites, or autoimmune targets. Granulomas may be caseating (with central eosinophilic necrosis resembling cottage cheese — classic in TB) or non-caseating (no central necrosis — seen in sarcoidosis, GPA, rhinoscleroma). From your microbiology recall that Mycobacterium tuberculosis is acid-fast (stained by Ziehl-Neelsen), Klebsiella rhinoscleromatis (Frisch bacillus) is a Gram-negative rod, and Rhinosporidium seeberi is an unusual organism (now classified as a mesomycetozoean) producing large endosporulating sporangia visible to the naked eye on the mucosal surface.
Clinical Presentation of Granulomatous Nasal Diseases
Granulomatous diseases of the nose share a cluster of symptoms that reflect the common pathological process of chronic granulomatous inflammation within the nasal mucosa and submucosa. Despite this shared symptom cluster, careful attention to the pattern of onset, the specific morphology of nasal lesions, associated systemic features, and the geographic and demographic background of the patient allows the clinician to narrow the differential diagnosis before investigations are requested. The shared symptom cluster — chronic nasal obstruction, foul-smelling crusting, epistaxis, and septal perforation — should be understood as the final common pathway of mucosal destruction, regardless of whether the cause is a mycobacterium, a Klebsiella, a sporangium-forming organism, or an autoimmune vasculitis. What varies between diseases is the rate of progression (rhinoscleroma is indolently chronic; GPA can progress rapidly), the systemic associations (pulmonary and renal in GPA; skin and peripheral nerves in leprosy; bilateral hilar lymphadenopathy in sarcoidosis), and the epidemiological context (rhinosporidiosis in coastal South Indian patients with a history of bathing in ponds; TB in a patient with pulmonary TB contacts; GPA in a patient presenting with haemoptysis and haematuria).
Shared clinical features across granulomatous nasal diseases:
- Chronic nasal obstruction: progressive, bilateral or unilateral, often insidious in onset, not responsive to standard antibiotic or antihistamine treatment.
- Nasal crusting: a characteristic feature — thick, dry, often foul-smelling (foetid) crusts adherent to the nasal mucosa; removal reveals a bleeding, raw surface. Crusting results from mucosal atrophy, destruction of seromucinous glands, and impaired mucociliary clearance.
- Epistaxis: recurrent, often mild but persistent; caused by mucosal erosion and granulation tissue vascularity.
- Hyposmia or anosmia: from mucosal destruction and obstruction of the olfactory cleft.
- Septal perforation: a key physical sign that indicates destruction of the nasal septal cartilage; caused by granulomatous vasculitis (GPA, syphilis) or direct mucosal necrosis (TB, leprosy). A septal perforation in the cartilaginous (anterior) septum — visible by direct examination — narrows the differential significantly.
- Saddle-nose deformity: collapse of the nasal bridge due to destruction of the septal cartilage; a sign of advanced, long-standing disease (classically seen in GPA, syphilis, leprosy, TB — the 'saddle nose' has a broad differential in granulomatous disease).
Distinguishing clinical features by diagnosis:
- Tuberculosis of nose: history of TB elsewhere (pulmonary, lymph node), constitutional symptoms (fever, night sweats, weight loss), positive Mantoux/IGRA.
- Rhinoscleroma: indurated mass in the nose and nasopharynx; progressive stenosis of the nasal airway; woodworker or farm exposure; endemic in Central Europe, Central America, parts of India; three stages (catarrhal → proliferative/granulomatous → sclerotic).
- Rhinosporidiosis: polypoidal mass in the nasal cavity with a characteristic 'strawberry' surface studded with white spots (sporangia visible to the naked eye); endemic in South India and Sri Lanka; history of bathing in rivers or ponds.
- GPA (Wegener's granulomatosis): bloody nasal crusting + epistaxis + saddle nose + systemic features (haemoptysis, haematuria, joint pain); most important non-infective granulomatous nasal disease.
- Sarcoidosis: often bilateral, associated with skin lesions (lupus pernio — violaceous plaque on nose), bilateral hilar lymphadenopathy on chest X-ray; elevated serum ACE.
- Leprosy: thickening and collapse of the anterior nasal septum and alae; nasal tip involvement; associated skin lesions (hypopigmented/anaesthetic patches) and peripheral nerve thickening.
- Syphilis: nasal bridge destruction (saddle nose) in tertiary/congenital syphilis; gumma formation; serology (VDRL/TPHA) positive.
Pathology and Specific Features of Each Granulomatous Disease
Each granulomatous nasal disease has a specific histological and microbiological signature that allows definitive diagnosis from biopsy material. Learning the key feature of each entity allows the student to interpret the biopsy report intelligently and to understand why each disease has its particular clinical behaviour.
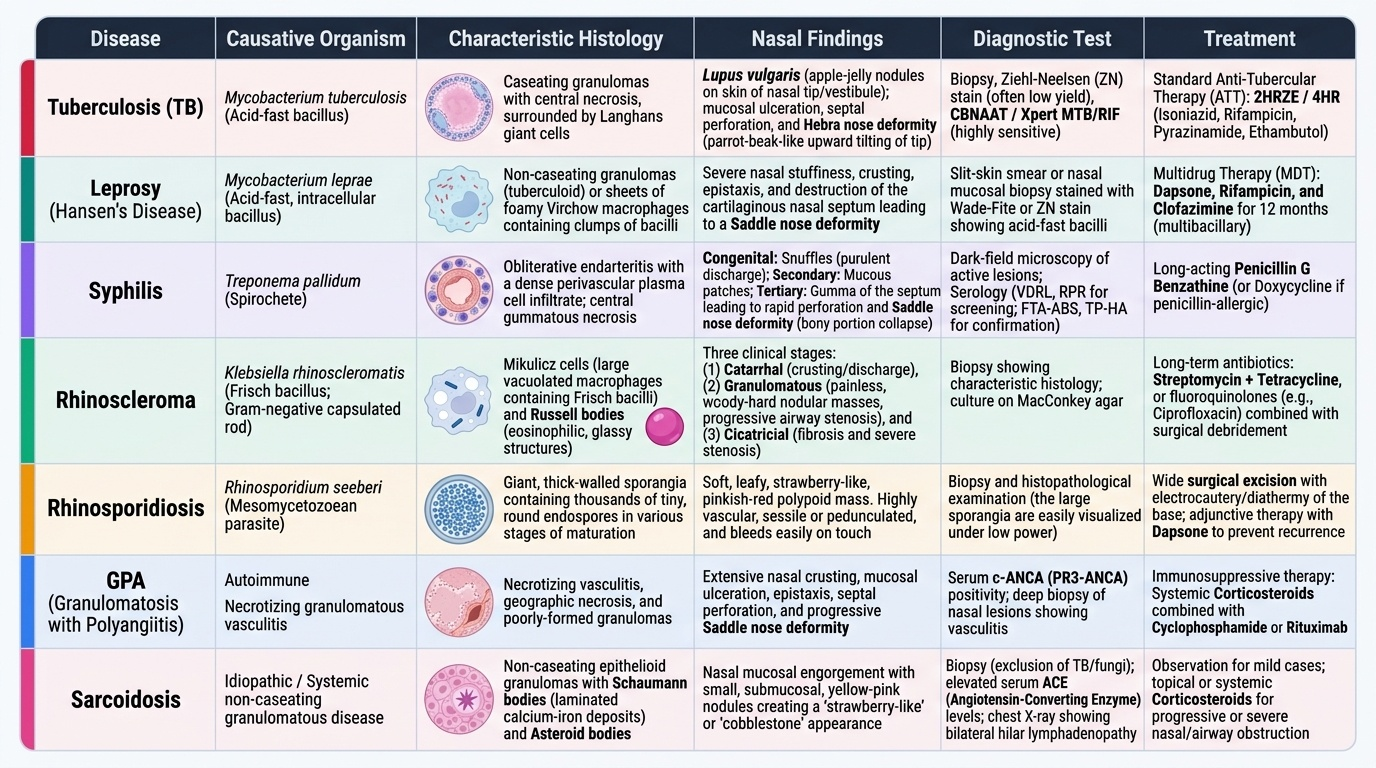
Provided image
Tuberculosis of the nose:
Lupus vulgaris is the most common form of cutaneous TB and frequently involves the nose — the most common site on the face for lupus vulgaris is the tip of the nose and the nasal vestibule. The lesion produces apple-jelly coloured nodules on the skin (diascopy — pressing a glass slide on the nodule reveals characteristic brown 'apple-jelly' colour from the underlying granulomas). More destructive nasal TB causes mucosal ulceration, septal perforation, and the Hebra nose deformity (destruction of the nasal septum and cartilage by TB, producing upward tilting of the nasal tip resembling a 'parrot beak' or tapir nose). Histology: caseating granulomas with Langhans giant cells; Ziehl-Neelsen stain positive for acid-fast bacilli (though yield from nasal tissue is low — CBNAAT/Xpert MTB/RIF is more sensitive). Treatment: standard antitubercular therapy (ATT) — isoniazid, rifampicin, pyrazinamide, ethambutol for 2 months; followed by isoniazid + rifampicin for 4 months (2HRZE/4HR).
Rhinoscleroma:
Caused by Klebsiella rhinoscleromatis (the Frisch bacillus), a Gram-negative capsulated rod. Rhinoscleroma is endemic in Central America, Central and Eastern Europe, and parts of India and Africa. It progresses through three clinical stages:
1. Catarrhal (rhinitic) stage: non-specific rhinitis with nasal discharge, crusting, and obstruction — clinically indistinguishable from chronic rhinitis.
2. Granulomatous (proliferative) stage: nodular indurated masses in the nasal cavity, nasopharynx, larynx, and trachea; progressive stenosis of the nasal airway. Histological hallmarks: Mikulicz cells (large vacuolated macrophages containing the bacilli) and Russell bodies (eosinophilic hyaline globules from plasma cell immunoglobulin accumulation). These two histological features are pathognomonic.
3. Sclerotic (cicatricial) stage: progressive fibrosis and stenosis; nasal airway may become severely compromised. Treatment: prolonged tetracyclines or ciprofloxacin for months to years; surgical debridement of obstructive granulation tissue; dilatation for stenosis.
Rhinosporidiosis:
Caused by Rhinosporidium seeberi, an unusual organism now classified as a mesomycetozoean (neither true fungus nor protozoan). Endemic in South India and Sri Lanka; infection is acquired through contact with water (bathing in rivers or stagnant ponds). The characteristic lesion is a soft, vascular, polypoidal mass in the nasal cavity with a strawberry-like surface due to white dots representing mature sporangia (each up to 300 μm diameter, visible to the naked eye). Histology: thickened mucosa with large sporangia at various stages of development — this is pathognomonic. Treatment: complete surgical excision with adequate margins (simple snare polypectomy causes haemorrhage and recurrence — the entire mass must be excised including the pedicle). No effective antifungal treatment exists; dapsone is sometimes used as an adjunct.
Granulomatosis with Polyangiitis (GPA — formerly Wegener's granulomatosis):
GPA is an ANCA-associated vasculitis affecting small and medium vessels, characterised by granulomatous inflammation of the upper and lower airways and pauci-immune necrotising crescentic glomerulonephritis. The nasal manifestation is the most common presenting feature: bloody nasal crusting, septal perforation (from vasculitic necrosis of the septal mucosa and cartilage), saddle-nose deformity, and recurrent sinusitis refractory to standard treatment. The diagnostic marker is c-ANCA (cytoplasmic ANCA directed against proteinase 3, PR3) — positive in >90% of active generalised GPA. Biopsy of nasal tissue shows necrotising granulomatous vasculitis with fibrinoid necrosis of vessel walls. GPA is treated with immunosuppression — induction with cyclophosphamide + high-dose corticosteroids (or rituximab as an equivalent or superior alternative per RAVE/WEGENT trials), followed by maintenance with azathioprine or methotrexate.
Sarcoidosis of the nose:
Sarcoidosis produces non-caseating granulomas (unlike TB, there is no central necrosis — the macrophages and giant cells are present but the granuloma centre is intact) in multiple organs. Nasal involvement occurs in ~20% of patients and may present with nasal obstruction, epistaxis, and the characteristic skin lesion lupus pernio — a violaceous, indurated plaque over the nose, cheeks, and lips. Systemic features include bilateral hilar lymphadenopathy (BHL) on chest X-ray, erythema nodosum (Löfgren's syndrome = BHL + erythema nodosum + periarthritis), elevated serum angiotensin-converting enzyme (ACE), and hypercalcaemia (from 1,25-dihydroxyvitamin D produced by granuloma macrophages). Treatment: systemic corticosteroids for symptomatic disease.
SELF-CHECK
A 40-year-old male presents with progressive nasal obstruction over 3 years. Rhinoscopy reveals indurated, nodular masses in both nasal cavities and the nasopharynx, with near-total nasal stenosis. He is from a rural part of Central India. Biopsy shows large vacuolated macrophages containing Gram-negative bacilli (Mikulicz cells) and Russell bodies. The diagnosis is:
A. Nasal tuberculosis — treat with standard antitubercular therapy (2HRZE/4HR)
B. Rhinoscleroma — caused by Klebsiella rhinoscleromatis; treat with prolonged ciprofloxacin or tetracyclines
C. Granulomatosis with polyangiitis — check c-ANCA and treat with cyclophosphamide
D. Rhinosporidiosis — treat with complete surgical excision
Reveal Answer
Answer: B. Rhinoscleroma — caused by Klebsiella rhinoscleromatis; treat with prolonged ciprofloxacin or tetracyclines
Mikulicz cells (large vacuolated macrophages containing Klebsiella rhinoscleromatis bacilli) and Russell bodies (eosinophilic hyaline globules from plasma cell immunoglobulin accumulation) are the pathognomonic histological features of rhinoscleroma. Rhinoscleroma is caused by Klebsiella rhinoscleromatis (Frisch bacillus) and produces progressive nasal stenosis through its three stages (catarrhal → granulomatous → sclerotic). Treatment is prolonged antibiotics (ciprofloxacin or tetracycline for months to years) with surgical debridement for stenosis. TB would show caseating granulomas with Langhans giant cells (not Mikulicz cells). GPA would show necrotising vasculitis. Rhinosporidiosis shows sporangia, not Mikulicz cells.
Examination and Investigations
The investigation of granulomatous nasal disease follows a logical sequence from clinical examination through targeted laboratory and pathological tests. The central principle is that biopsy and histopathology are the definitive investigation for virtually every granulomatous nasal disease — the clinical examination narrows the differential, but tissue diagnosis confirms it. Understanding this principle prevents the most common error in managing these patients: repeated courses of empirical antibiotics without tissue diagnosis. Each granulomatous disease has a specific histological signature — Mikulicz cells and Russell bodies in rhinoscleroma, sporangia in rhinosporidiosis, caseating granuloma with Langhans giant cells in TB, non-caseating granuloma in sarcoidosis, necrotising vasculitis in GPA — and the only way to identify these signatures is to obtain tissue. The clinician requesting the biopsy should communicate to the pathologist which diagnoses are being considered, so that the correct special stains (ZN for AFB, PAS/GMS for fungi, Gram for bacteria) are performed on the specimen from the outset rather than as afterthoughts when the H&E is non-diagnostic.
Anterior rhinoscopy findings: The clinician should document the following systematically:
- Distribution and character of crusting (diffuse vs localised, foul-smelling vs not);
- Mucosal appearance (ulcerated, granular, nodular, hypertrophied);
- Polypoidal masses — their surface (smooth vs strawberry = rhinosporidiosis), vascularity;
- Nasal septum — presence and location of perforation (cartilaginous septum: anterior, seen directly on rhinoscopy; bony septum: requires endoscopy); saddle-nose on external examination;
- Inferior and middle turbinate size and morphology.
Nasal endoscopy: Provides detailed visualisation of the posterior nasal cavity, middle and superior meatus, sphenoethmoidal recess, and nasopharynx. Essential for rhinoscleroma (which involves the nasopharynx and larynx) and for biopsy guidance.
Biopsy and histopathology: The central investigation for all granulomatous nasal diseases. The biopsy specimen should be sent for:
- Haematoxylin and eosin (H&E) staining — identifies granuloma architecture, type of giant cells, caseation;
- Ziehl-Neelsen (ZN) stain / CBNAAT (Xpert MTB/RIF) — for acid-fast bacilli (tuberculosis);
- PAS stain (Periodic Acid Schiff) and Grocott's methenamine silver (GMS) — for fungi and rhinosporidiosis sporangia;
- Gram stain and bacterial culture — for rhinoscleroma (Klebsiella);
- Immunofluorescence or immunohistochemistry — for GPA (pauci-immune vasculitis pattern).
Specific investigations by diagnosis:
- GPA: Serum c-ANCA (anti-PR3) — sensitivity >90% for active generalised GPA; urine dipstick for haematuria and proteinuria (renal involvement); CXR and CT chest for pulmonary involvement; renal function and consider renal biopsy if nephritis is suspected.
- Sarcoidosis: Serum ACE (elevated in ~60% of active sarcoidosis); serum calcium; CXR (bilateral hilar lymphadenopathy); CT chest; consider bronchoalveolar lavage (CD4:CD8 ratio >3.5 in pulmonary sarcoidosis); Kveim test (historical — not routinely used).
- Tuberculosis: Mantoux test (TST), IGRA (QuantiFERON Gold), CBNAAT on biopsy material; CXR for pulmonary TB; sputum AFB if pulmonary TB suspected.
- Syphilis: Serum VDRL (screening) and TPHA/FTA-ABS (confirmatory).
- Leprosy: Slit-skin smear from nasal mucosa for acid-fast bacilli (Fite-Faraco stain); skin biopsy; nerve conduction studies.
- Rhinosporidiosis: Diagnosis is clinical (strawberry polyp in endemic area) + biopsy showing sporangia.