Page 12 of 21
EN4.33 | Tumours of Nose, Nasopharynx and Paranasal Sinuses — SDL Guide (Part 2)
Diagnosis and Staging
Staging of sinonasal and nasopharyngeal tumours follows TNM principles and determines treatment planning and prognosis. Two staging concepts are particularly important for final-year students: Ohngren's line for maxillary sinus carcinoma and the AJCC/UICC NPC staging. Staging is not merely an academic exercise — it directly governs the surgical approach, the extent of resection, whether orbital exenteration is needed, and whether the patient will receive concurrent chemotherapy in addition to radiotherapy. The most clinically powerful staging tool for maxillary sinus tumours is Ohngren's line, which is simple enough to apply at the bedside using anatomical landmarks and predicts operability and prognosis without any equipment. For NPC, the bilateral nodal involvement and skull base T-stage are the key determinants of whether concurrent chemotherapy is added to radiotherapy. Beyond formal TNM staging, the clinician must maintain awareness of the 'red flag' features in any patient presenting with nasal symptoms — features that mandate urgent investigation rather than empirical sinusitis treatment.
Ohngren's line for maxillary sinus SCC:
Ohngren's line is drawn from the medial canthus (inner corner of the eye) to the angle of the mandible. This imaginary plane divides the maxillary sinus into:
- Anteroinferior (infrastructure): below and in front of the line. Tumours in this compartment tend to present earlier (facial swelling, dental symptoms, nasal obstruction) and are more amenable to surgical excision (total maxillectomy). Prognosis is better.
- Superoposterior (suprastructure): above and behind the line. Tumours here abut the orbital floor, pterygomaxillary fossa, infratemporal fossa, and skull base — structures that are difficult to achieve clear surgical margins around. Prognosis is significantly worse.
Ohngren's line is a prognostic tool — it helps predict the likelihood of achieving complete resection and the anticipated extent of surgery needed.
Staging of NPC (AJCC 8th edition):
- T1: confined to nasopharynx, oropharynx, or nasal fossa.
- T2: parapharyngeal space extension and/or medial pterygoid, lateral pterygoid, or prevertebral muscles.
- T3: bony structures (skull base, cervical vertebrae, pterygoid structures) or paranasal sinuses.
- T4: intracranial extension, cranial nerve involvement, orbit, hypopharynx, infratemporal fossa, or masticator space.
- N staging: bilateral nodal involvement is characteristic of NPC (unlike most head and neck cancers which are predominantly ipsilateral at early stages).
Red flags for malignancy in nasal and sinus disease:
- Unilateral symptoms (obstruction, discharge, epistaxis) in a middle-aged or elderly adult;
- Blood-stained nasal discharge — persistent, not explained by trauma;
- Bone erosion on CT;
- Nerve symptoms: paraesthesia of cheek (infraorbital nerve), jaw, or palate;
- Cervical lymphadenopathy — particularly posterior triangle or bilateral upper cervical nodes;
- Failure to respond to appropriate treatment for sinusitis;
- Rapid progression of symptoms.
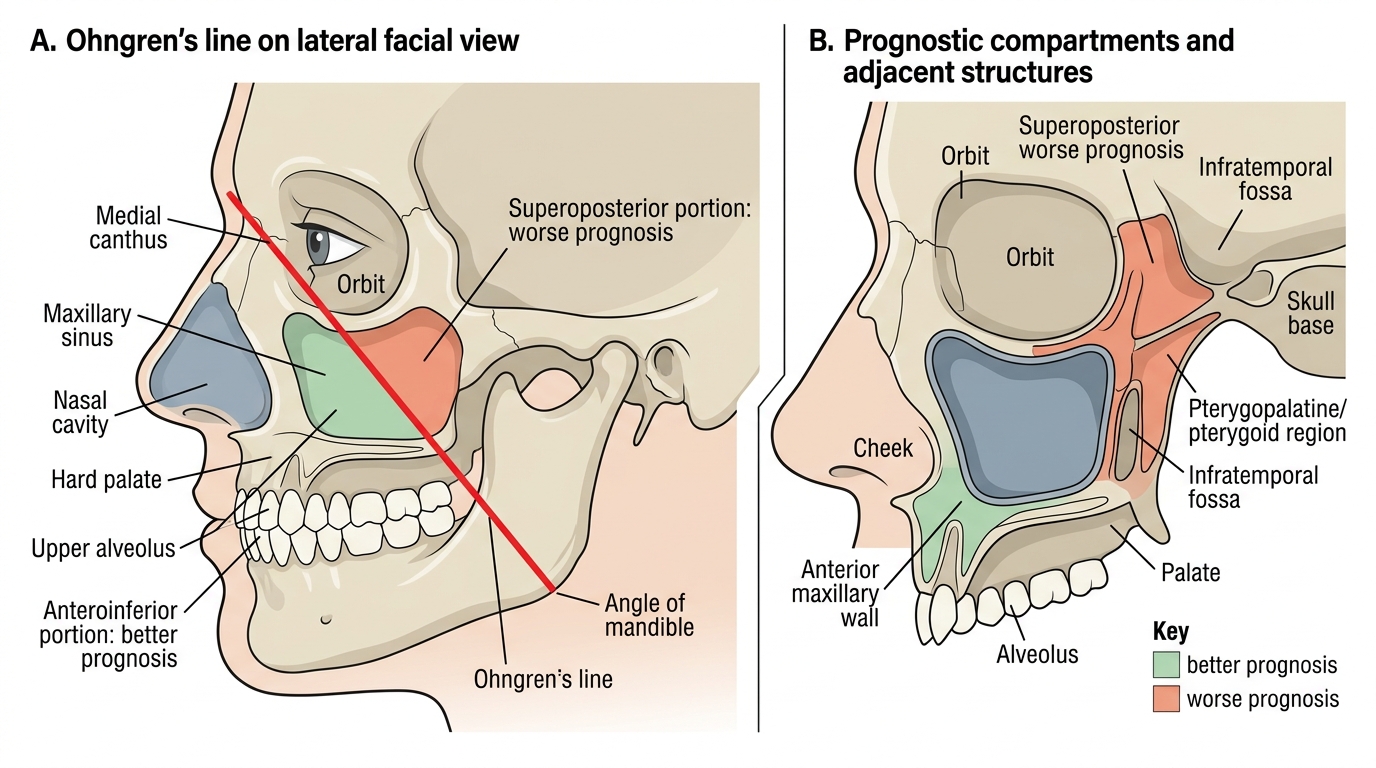
Ohngren's Line and Prognostic Compartments of the Maxillary Sinus
SELF-CHECK
A 38-year-old Cantonese-speaking man presents to your ENT clinic with 3 months of painless bilateral posterior cervical lymphadenopathy. He has unilateral left-sided conductive hearing loss and reports 'blood in his spit' in the morning. Nasal endoscopy reveals an irregular mass in the left fossa of Rosenmüller. The most likely diagnosis and the most important aetiological agent are:
A. Hodgkin lymphoma; aetiology is EBV but lymph node FNAC is the first investigation
B. Nasopharyngeal carcinoma (Type III undifferentiated); strongly EBV-associated; nasopharyngeal biopsy required for definitive diagnosis
C. Anaplastic thyroid carcinoma; rapidly progressive; requires urgent FNA of the neck mass
D. Nasopharyngeal angiofibroma; biopsy is contraindicated; contrast CT is the first investigation
Reveal Answer
Answer: B. Nasopharyngeal carcinoma (Type III undifferentiated); strongly EBV-associated; nasopharyngeal biopsy required for definitive diagnosis
The combination of a young-middle-aged patient of Chinese/Southeast Asian or African origin, bilateral posterior cervical lymphadenopathy (characteristically bilateral and posterior in NPC), unilateral conductive deafness (from Eustachian tube obstruction), blood-stained postnasal secretions, and a nasopharyngeal mass in the fossa of Rosenmüller is the classic presentation of nasopharyngeal carcinoma (NPC Type III undifferentiated). EBV is the dominant aetiological agent for Types II and III. Nasopharyngoscopic biopsy is required for definitive diagnosis. Hodgkin lymphoma can present with cervical nodes and EBV association, but the nasopharyngeal mass in the fossa of Rosenmüller is specific for NPC. JNA affects adolescent males with severe epistaxis, not a fossa of Rosenmüller mass and conductive deafness in a 38-year-old.
CLINICAL PEARL
Two rules that prevent dangerous diagnostic delays with nasal tumours: (1) Any unilateral nasal symptom in a middle-aged or elderly adult that does not resolve with standard treatment within 4–6 weeks must be investigated with nasal endoscopy and CT — never assume 'chronic sinusitis' without objective evidence. (2) Unilateral conductive hearing loss (glue ear) in an adult, especially of Asian or African origin, must be investigated with nasopharyngoscopy to exclude NPC at the Eustachian tube opening in the nasopharynx. These two rules — if applied consistently — would detect most nasal and nasopharyngeal malignancies at an earlier and more curable stage.
Principles of Management
The management of sinonasal and nasopharyngeal tumours is highly dependent on histological type, site, and stage. The broad principles are: malignant sinonasal tumours are treated primarily with surgery (when resectable) combined with post-operative radiotherapy; NPC is treated primarily with radiotherapy and concurrent chemotherapy (because Types II and III are radiosensitive and surgery in the nasopharynx carries high morbidity).
Inverted papilloma:
Complete surgical excision with adequate margins — the gold standard is endoscopic medial maxillectomy (resection of the medial maxillary wall including the attachment site on the lateral nasal wall). The critical point is to remove the entire attachment site to prevent recurrence. Recurrence after incomplete excision approaches 70%. Because of the ~10% malignant transformation risk, all excised tissue must be submitted for histopathological examination to exclude synchronous or metachronous SCC.
Maxillary sinus SCC:
The standard surgical procedure for resectable maxillary SCC is total maxillectomy — resection of the entire maxillary bone, including the hard palate, the floor and walls of the maxillary sinus, and sometimes the orbital floor (radical maxillectomy). The approach is via a lateral rhinotomy incision (or a Weber-Ferguson incision for wider access). Where the orbital contents are not grossly invaded, the eye may be preserved (subtotal or limited orbital resection); where the orbital fat or globe is involved, orbital exenteration may be required. Post-operative radiotherapy is given to the resection bed. For infrastructure tumours (below Ohngren's line), partial maxillectomy may be sufficient. Chemotherapy (cisplatin-based) is added for locally advanced or unresectable disease in a palliative or concomitant intent.
Nasopharyngeal carcinoma:
NPC (particularly Types II and III) is radiosensitive — it responds well to radiotherapy. Surgery plays no primary role because the nasopharynx is surgically inaccessible with adequate margins, and the tumour is radio-responsive. The standard treatment for Stage I NPC is radiotherapy alone. For Stage II–IVB, the standard is concurrent cisplatin-based chemoradiotherapy (CRT) — the Intergroup 0099 trial demonstrated that concurrent CRT significantly improves both progression-free survival and overall survival compared with radiotherapy alone. Intensity-modulated radiotherapy (IMRT) is the modern standard for NPC, minimising radiation dose to the salivary glands, spinal cord, and temporal lobes while delivering tumoricidal doses to the nasopharynx and cervical nodes.
Olfactory neuroblastoma:
Craniofacial resection (combined transcranial and transnasal approach) for complete resection of the cribriform plate and associated tumour, followed by post-operative radiotherapy. Chemotherapy is added for high-grade (Hyams Grade 3–4) tumours. Prognosis is stage-dependent.
Palliative management: Patients with unresectable, metastatic, or recurrent disease receive palliative chemotherapy, radiotherapy for symptom control (epistaxis, pain, cranial nerve symptoms), and supportive care. Early hospice and palliative care consultation is appropriate for advanced disease.
| Tumour | Primary Treatment | Adjuvant/Combined |
|---|---|---|
| Inverted papilloma | Endoscopic medial maxillectomy (complete excision) | None; surveillance for recurrence |
| Maxillary SCC (infrastructure) | Partial/total maxillectomy | Post-op radiotherapy |
| Maxillary SCC (suprastructure/advanced) | Total/radical maxillectomy | Post-op CRT |
| NPC Stage I | IMRT radiotherapy alone | — |
| NPC Stage II–IVB | Concurrent cisplatin CRT | Adjuvant chemotherapy considered |
| Olfactory neuroblastoma | Craniofacial resection | Post-op radiotherapy |
| Ethmoid adenocarcinoma | Endoscopic or craniofacial resection | Post-op radiotherapy |
Self-Assessment: Sinonasal and Nasopharyngeal Tumours
Use these scenarios to test your clinical reasoning on sinonasal and nasopharyngeal tumour diagnosis and management.
Scenario 1: A 55-year-old male smoker is found on CT to have a 3.5 cm mass in the right maxillary sinus with erosion of the orbital floor but without evidence of orbital fat invasion. The medial wall is eroded. He has infraorbital nerve paraesthesia. Histology confirms squamous cell carcinoma. Is this an infrastructure or suprastructure tumour, and what surgical procedure would be planned?
Expected answer: Orbital floor erosion (roof of the maxillary sinus) places this tumour in the suprastructure (above Ohngren's line), which carries a worse prognosis. The infraorbital nerve paraesthesia confirms involvement of the orbital floor/inferior orbital fissure region. Planned surgery: total maxillectomy with assessment of the orbital floor — if orbital fat is not invaded, the orbital contents may be preserved (orbital floor resection with orbital preservation). If orbital fat is involved on MRI, orbital exenteration must be discussed with the patient. Post-operative radiotherapy is given to the resection bed and regional nodes.
Scenario 2: A 29-year-old Malaysian man presents with bilateral posterior cervical lymphadenopathy and unilateral right-sided hearing loss for 6 months. He has no nasal obstruction or nosebleeds. Nasopharyngoscopy reveals a smooth-looking mucosa over the right fossa of Rosenmüller, but there is subtle fullness compared to the left. What do you do next, and what would you look for on MRI?
Expected answer: NPC must be excluded — nasopharyngoscopy-guided biopsy of the fossa of Rosenmüller bilaterally (the tumour may be submucosal and not visibly irregular). Serum EBV VCA-IgA. MRI nasopharynx and skull base to detect a submucosal mass, parapharyngeal space extension, and skull base invasion. Submucosal NPC (also called 'silent' NPC) can have a normal or near-normal nasopharyngeal surface but is visible as a T2-hyperintense mass or asymmetric parapharyngeal fullness on MRI.
Scenario 3: What is the significance of Gardner's syndrome when managing a patient found to have a frontal sinus osteoma?
Expected answer: Gardner's syndrome is an autosomal dominant condition (APC gene mutation) characterised by familial adenomatous polyposis (FAP) of the colon, multiple osteomas (especially craniofacial), epidermoid cysts, and desmoid tumours. An osteoma found incidentally on head CT should prompt enquiry about bowel symptoms, family history, and referral for colonoscopy to exclude FAP — which has a near-100% risk of malignant transformation to colorectal carcinoma if untreated. Identifying Gardner's syndrome from an apparently innocent osteoma is a potentially life-saving diagnosis.
SELF-CHECK
A patient with Stage III nasopharyngeal carcinoma (NPC) is being planned for treatment. Which of the following is the evidence-based standard of care for this stage?
A. Surgery alone (total nasopharyngectomy with neck dissection)
B. Radiotherapy alone to the nasopharynx and bilateral neck
C. Concurrent cisplatin-based chemoradiotherapy (CRT) — established by the Intergroup 0099 trial
D. Induction chemotherapy alone, followed by watchful waiting if there is good response
Reveal Answer
Answer: C. Concurrent cisplatin-based chemoradiotherapy (CRT) — established by the Intergroup 0099 trial
For Stage II–IVB nasopharyngeal carcinoma, concurrent cisplatin-based chemoradiotherapy (CRT) is the standard of care, established by the landmark Intergroup 0099 trial, which demonstrated significantly improved progression-free survival and overall survival with concurrent CRT compared with radiotherapy alone. Surgery has no primary role in NPC management because the nasopharynx is not surgically accessible with adequate margins, and NPC (Types II and III) is radiosensitive. Radiotherapy alone may be adequate for Stage I NPC, not Stage III. Induction chemotherapy without definitive locoregional treatment is not standard. The modern radiotherapy technique is IMRT, which protects the salivary glands, temporal lobes, and spinal cord.