Page 4 of 17
EN4.38 | Acute and Chronic Tonsillitis — SDL Guide
Learning Objectives
- Elicit and document a structured history from a patient presenting with acute or chronic tonsillitis, including frequency of episodes, associated complications, and impact on daily activity
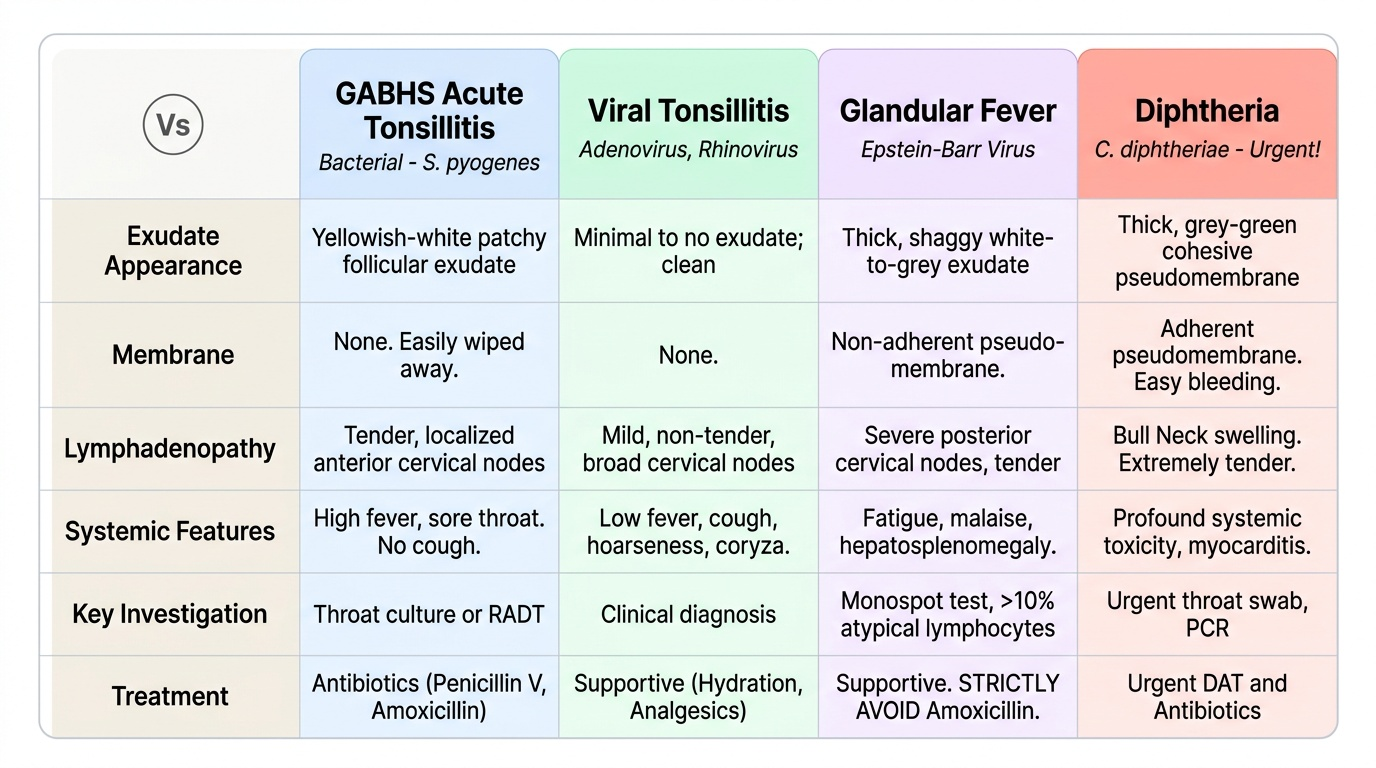
- Describe the clinical features of acute tonsillitis and differentiate bacterial (GABHS) from viral and other causes (EBV, diphtheria, Vincent's angina)
- List the local, regional, and systemic complications of acute and chronic tonsillitis
- Select and justify appropriate investigations for a patient with tonsillitis
- Describe the principles of management of acute tonsillitis, peritonsillar abscess, and the indications for tonsillectomy
INSTRUCTIONS
Tonsillitis is among the most common infections encountered in general practice and ENT, yet it conceals serious diagnostic traps and potentially dangerous complications. The student who can distinguish streptococcal from viral tonsillitis at the bedside, recognise a developing quinsy before it becomes an airway emergency, and apply the Paradise criteria for tonsillectomy is well equipped for both examinations and clinical practice. This module also addresses the non-suppurative complications — rheumatic fever and post-streptococcal glomerulonephritis — whose prevention depends entirely on completing a full antibiotic course.
References
- Dhingra PL. Diseases of Ear, Nose & Throat, 7th ed. Ch — Tonsils and Adenoids (textbook)
- Hazarika P. Textbook of Ear, Nose & Throat and Head-Neck Surgery. Ch — Diseases of the Tonsils (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed. Vol 2 — Oropharynx and Tonsil (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 19-year-old college student presents to casualty at midnight with a 4-day history of severe sore throat and high fever. He has been unable to eat or drink properly for the past two days. Today he noticed that his voice has become 'hot-potato' or muffled in quality, and he is having difficulty opening his mouth fully. On examination, you notice that the right tonsillar region appears bulging, the uvula is displaced to the left, and the patient is drooling saliva. What is your diagnosis, and what is your immediate management plan?
WHY THIS MATTERS
Tonsillitis affects all age groups but is particularly prevalent in children and young adults, making it one of the most common reasons for antibiotic prescriptions in India and globally. While most cases resolve with simple treatment, the clinician who under-treats bacterial tonsillitis risks the development of quinsy (peritonsillar abscess), parapharyngeal abscess, or — critically — rheumatic fever and post-streptococcal glomerulonephritis. At the other extreme, over-prescribing antibiotics for viral tonsillitis contributes to antimicrobial resistance, and prescribing amoxicillin for glandular fever (EBV tonsillitis) causes a characteristic maculopapular rash. EN4.38 requires you to elicit a structured history, describe clinical features, choose correct investigations, identify complications, and describe management principles — all at the SH (Supervised/Simulated) level. The Paradise criteria for tonsillectomy, the Centor scoring system, and the management of quinsy are clinical facts that appear in every ENT examination and must be known accurately.
RECALL
Recall from your Anatomy sessions that Waldeyer's ring is the lymphoid ring guarding the entrance to the aerodigestive tract. It is composed of the paired palatine tonsils (in the tonsillar fossae between the anterior and posterior tonsillar pillars), the nasopharyngeal tonsil (adenoids) on the posterior wall of the nasopharynx, the paired tubal tonsils near the opening of the Eustachian tubes, and the lingual tonsil at the base of the tongue. The palatine tonsil has a fibrous capsule and numerous deep crypts that extend from the free surface into the lymphoid tissue — these crypts normally drain secretions; in chronic tonsillitis they become colonised by mixed oral bacteria and fill with tonsillar debris (plugs). The tonsil's blood supply comes primarily from the tonsillar branch of the facial artery (dominant lower pole supply), with contributions from the ascending palatine, lingual, and ascending pharyngeal arteries. The peritonsillar space between the tonsil capsule and the superior pharyngeal constrictor is the anatomical site where peritonsillar abscess (quinsy) forms. Recall also from Physiology and Microbiology that Group A beta-haemolytic Streptococcus (Streptococcus pyogenes) is the bacterium whose M protein can trigger autoimmune cross-reactions with cardiac valves — the basis of rheumatic fever — which is why a full 10-day penicillin course is mandatory even after symptom resolution.
Clinical Presentation of Tonsillitis
The clinical presentation of tonsillitis varies by acuity (acute vs chronic), by causative organism (bacterial vs viral), and by whether complications have developed. Taking a structured history is the essential first step in distinguishing uncomplicated tonsillitis from a developing abscess and in determining whether the frequency of attacks justifies surgical intervention. A student who asks only 'how long has the throat been sore?' will miss the frequency and complication data that drive management decisions. In particular, documenting the number of episodes per year with their clinical features is the prerequisite for any meaningful discussion of tonsillectomy — the Paradise criteria require documented episodes, not merely a patient's recollection. The history must therefore be detailed, systematic, and prospective whenever possible, which means advising patients to keep a record of future episodes if their current episode count is approaching the surgical threshold.
Acute tonsillitis — characteristic history:
- Sore throat (odynophagia): sudden onset, severe, worsening with swallowing. Often bilateral.
- Fever: high-grade (38–40°C) in bacterial infection; lower-grade or absent in viral.
- Referred otalgia: ear pain from referred pain via the glossopharyngeal nerve (IX) — the nerve supplying the tonsil also supplies the ear via Jacobsen's branch. This referred otalgia does not indicate ear pathology.
- Dysphagia and drooling: as the pain worsens, the patient stops swallowing saliva.
- 'Hot-potato' voice (muffled, potato-in-mouth quality): strongly suggests peritonsillar abscess (quinsy) — the pus displaces the soft palate, alters resonance, and impairs articulation. This is an alarm sign requiring urgent assessment.
- Trismus (inability to open the mouth fully): spasm of the medial pterygoid muscle due to adjacent infection — another sign of peritonsillar or parapharyngeal abscess.
- Fever, malaise, and generalised lymphadenopathy: more prominent in viral causes, especially glandular fever (infectious mononucleosis) due to Epstein-Barr virus (EBV).
Chronic tonsillitis — characteristic history:
- Recurrent episodes: the single most important historical feature. Document the number of episodes per year, whether each was documented by a doctor, and the duration of illness with each episode (Paradise criteria require each episode to include sore throat + at least one of: temperature >38.3°C, cervical lymphadenopathy, tonsillar exudate, or positive throat swab for GABHS).
- Persistent foetor oris (bad breath): from tonsillar debris (caseous plugs filling chronically infected crypts).
- Persistent soreness or foreign body sensation in the throat.
- Snoring and sleep-disordered breathing: when tonsillar hypertrophy is prominent.
- Poor general health, school/work absences: from recurrent febrile episodes.
Anatomy and Pathophysiology of the Tonsils
The palatine tonsil is a secondary lymphoid organ embedded in the lateral wall of the oropharynx, between the anterior tonsillar pillar (palatoglossus muscle) and the posterior tonsillar pillar (palatopharyngeus muscle). Its medial surface, which faces the oropharyngeal airway, bears 10–30 deep crypts lined by stratified squamous epithelium — the same epithelium as the pharynx. These crypts normally allow antigens from the ingested material and inhaled air to be sampled by the underlying lymphoid tissue, stimulating immune responses. The tonsil lacks afferent lymphatics; it instead receives antigens directly via the crypt epithelium. The lateral surface of the tonsil is enclosed within a fibrous capsule that separates it from the peritonsillar space — a potential space between the capsule and the superior pharyngeal constrictor muscle. This peritonsillar space is the critical anatomical site for abscess formation in quinsy.
Microbiology of tonsillitis:
The most important bacterial cause is Group A beta-haemolytic Streptococcus (GABHS, Streptococcus pyogenes), responsible for approximately 30% of acute tonsillitis cases in children and young adults. Other bacteria include Haemophilus influenzae, Moraxella catarrhalis, and anaerobes (important in chronic and peritonsillar infection). The majority of acute tonsillitis cases are viral — adenovirus (most common), rhinovirus, influenza, parainfluenza, and Epstein-Barr virus (EBV) (glandular fever). EBV tonsillitis is characterised by a more severe and prolonged illness, marked cervical lymphadenopathy, splenomegaly, and a membranous exudate that may mimic diphtheria.
Pathophysiology of chronic tonsillitis:
In chronic tonsillitis, repeated acute infections lead to progressive fibrous scarring of the lymphoid tissue and distortion and deepening of the tonsillar crypts. Debris (desquamated epithelium, food particles, bacteria) accumulates in these crypts as tonsillar plugs (caseous material), perpetuating low-grade infection and halitosis. The tonsil may appear small and scarred (from fibrosis) rather than enlarged — students must not equate the absence of tonsillar hypertrophy with the absence of chronic tonsillitis. The pathological entity in chronic tonsillitis is crypt pathology and persistent bacterial colonisation, not necessarily size.
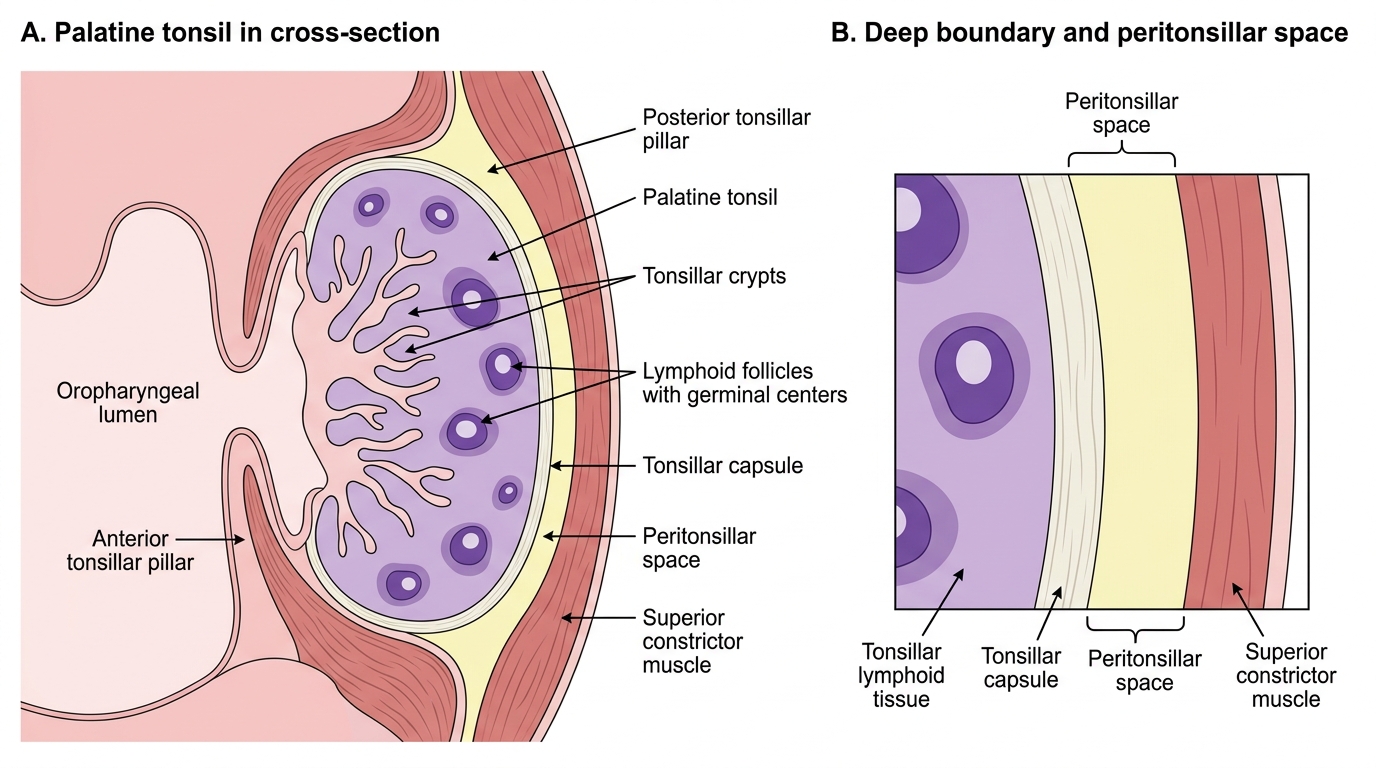
Palatine Tonsil in Cross-Section
Examination and Investigation of Tonsillitis
A careful examination of the oropharynx, combined with systematic assessment of the neck and general condition, allows the clinician to distinguish uncomplicated tonsillitis from a developing peritonsillar or parapharyngeal abscess and to differentiate bacterial from viral causes. The examination takes priority over investigations in acute tonsillitis, because in the case of a developing abscess, immediate drainage is required regardless of culture results. This systematic approach — from general inspection to oropharynx to neck to investigations — takes no more than 5–10 minutes and should be conducted in the same order at every encounter so that no key finding is missed. The sequence described here also helps the student distinguish features of uncomplicated tonsillitis from those of quinsy — a distinction with immediate management consequences that must never be missed.
Provided image
Oropharyngeal examination findings:
- Acute tonsillitis: bilateral tonsillar enlargement; erythema of the tonsils and anterior pillars; exudate may be present as white or yellow follicles (follicular tonsillitis) or a membranous sheet on the tonsil surface (membranous tonsillitis). Uvula is central (distinguishes from quinsy).
- Grading of tonsillar size (0–4+): Grade 0 = tonsils within the tonsillar fossae; Grade 1 = occupy <25% of the oropharyngeal width; Grade 2 = 25–50%; Grade 3 = 50–75%; Grade 4 = >75% ('kissing tonsils', occupying most of the airway width). Grades 3–4 with symptoms of sleep-disordered breathing support surgical indication.
- Peritonsillar abscess (quinsy): unilateral tonsillar and peritonsillar swelling; uvula displaced to the contralateral side; soft palate pushed forward and medially; trismus (cannot open the mouth fully); 'hot-potato' muffled voice. The pus lies in the peritonsillar space above the upper pole of the tonsil (anterosuperior quadrant is the most common site).
- Chronic tonsillitis: tonsils may be small, scarred, and asymmetric; crypts visible with caseous debris; anterior pillar may be hyperaemic.
Neck examination: cervical lymphadenopathy — tender anterior cervical nodes in bacterial tonsillitis; posterior cervical chain and generalised lymphadenopathy in EBV glandular fever.
The Centor criteria estimate the probability of GABHS infection: (1) tonsillar exudate, (2) tender anterior cervical lymphadenopathy, (3) fever >38°C, (4) absence of cough. Score 0–1: low probability of GABHS, antibiotic not recommended. Score 2–3: moderate probability, consider throat swab and antibiotic. Score 4: high probability, empirical antibiotic appropriate.
Investigations:
- Throat swab and culture: to confirm GABHS and guide antibiotic choice; rapid antigen detection test (RADT) available in some settings.
- Monospot test (Paul-Bunnell / heterophile antibody test): positive in infectious mononucleosis (EBV); sensitive in the second week of illness.
- Full blood count: neutrophilia in bacterial infection; lymphocytosis with atypical lymphocytes (Downey cells) in EBV glandular fever.
- EBV-specific antibodies (VCA IgM): confirmatory for EBV when monospot is negative.
- Blood culture: in systemically unwell patients with suspected deep space infection (parapharyngeal abscess, Ludwig's angina).
- CT scan of the neck (with contrast): to distinguish peritonsillar cellulitis from frank abscess (ring-enhancing collection), and to assess extension into the parapharyngeal or retropharyngeal space.
SELF-CHECK
A 17-year-old presents with a 5-day sore throat, high fever, and cervical lymphadenopathy. Examination shows bilateral tonsillar exudate and marked splenomegaly. A monospot test is positive. The doctor prescribes amoxicillin. What is the expected complication of this prescription?
A. Agranulocytosis requiring bone marrow biopsy
B. A widespread maculopapular rash due to the combination of amoxicillin with EBV infection
C. Stevens-Johnson syndrome from penicillin allergy
D. Toxic shock syndrome from streptococcal superinfection
Reveal Answer
Answer: B. A widespread maculopapular rash due to the combination of amoxicillin with EBV infection
Infectious mononucleosis (EBV) is a viral illness and does not respond to antibiotics. If amoxicillin (or ampicillin) is prescribed to a patient with acute EBV infection, approximately 80–100% of patients develop a widespread maculopapular skin rash — this is an immune-mediated reaction specific to the EBV-amoxicillin combination and is NOT a true penicillin allergy. It is the classic trap for a clinician who diagnoses 'bacterial tonsillitis' without considering EBV. The monospot (heterophile antibody) test being positive here clinches the diagnosis of glandular fever. Treatment is supportive (rest, analgesia, fluids) not antibacterial.