Page 1 of 17
EN4.37 | Dysphagia — SDL Guide
Learning Objectives
- Elicit and document a structured history from a patient presenting with dysphagia, including onset, progression, solid vs liquid discrimination, and associated symptoms
- Describe the clinical features that distinguish oropharyngeal dysphagia from oesophageal dysphagia
- List the principal causes of dysphagia under a systematic classification (mechanical vs motility; oropharyngeal vs oesophageal)
- Select and justify appropriate investigations for a patient presenting with dysphagia
- Describe the principles of management for the major causes of dysphagia encountered in clinical practice
INSTRUCTIONS
Dysphagia — difficulty swallowing — is both a common outpatient complaint and a potential alarm symptom for pharyngeal or oesophageal malignancy. An intern who can take a structured dysphagia history and order the right investigation in the right sequence can make a diagnosis that changes a patient's life. This module builds the clinical reasoning framework you need, anchored in ENT anatomy and the pathophysiology of swallowing. By the end, you should be able to reach a probable diagnosis from the history alone and confirm it systematically.
References
- Dhingra PL. Diseases of Ear, Nose & Throat, 7th ed. Ch 52 — Dysphagia (textbook)
- Hazarika P. Textbook of Ear, Nose & Throat and Head-Neck Surgery. Ch — Oesophagus and Dysphagia (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed. Vol 2 — Pharynx and Oesophagus (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old retired schoolteacher presents to your ENT OPD with a three-month history of difficulty swallowing. It started with solids — bread and rice were getting 'stuck' in her chest — and has now progressed to include soft foods. She has lost 5 kg without trying. On direct questioning, she points to the mid-sternal region when asked where food gets stuck. She denies heartburn or regurgitation of undigested food. Her husband mentions that she seemed perfectly well a year ago. What diagnosis must you exclude first, and what is the single most important investigation you will order?
WHY THIS MATTERS
Dysphagia is the presenting complaint in some of the most consequential diagnoses in ENT and upper gastrointestinal surgery — pharyngeal and oesophageal carcinoma, achalasia, and pharyngeal pouch among them. In India, where carcinoma of the hypopharynx and oesophagus carry significant morbidity (tobacco and alcohol use, nutritional deficiencies, and Plummer-Vinson syndrome contributing), delay in diagnosis is directly linked to late-stage presentation and reduced survival. EN4.37 is a Skill at the Supervised/Simulated (SH) level — you must be able to elicit the history, choose the correct investigation, and describe management principles not just in theory but in a supervised clinical interaction. The doctor who knows the three alarm features of dysphagia — progressive solid-food difficulty, weight loss, and age over 40 — and acts on them promptly is the doctor who saves lives in an outpatient clinic.
RECALL
Recall from your Physiology sessions that swallowing is a complex, precisely coordinated reflex involving over 25 muscle groups and five cranial nerves. The process has three phases: the oral preparatory and propulsive phase (voluntary — the tongue propels the food bolus to the oropharynx), the pharyngeal phase (involuntary, triggered by contact with the posterior pharyngeal wall — lasts about 1 second; the larynx elevates, the vocal cords adduct, the epiglottis deflects, the cricopharyngeus relaxes to open the upper oesophageal sphincter), and the oesophageal phase (involuntary peristalsis carries the bolus to the stomach; the lower oesophageal sphincter relaxes to admit it). Recall also from Anatomy that the pharynx is divided into the nasopharynx, oropharynx, and hypopharynx (laryngopharynx), and that the hypopharynx is the most clinically important site for malignant dysphagia in ENT. The cricopharyngeus muscle is the main component of the upper oesophageal sphincter; Killian's dehiscence is the triangular weak spot in the posterior pharyngeal wall between the oblique thyropharyngeus fibres and the horizontal cricopharyngeus fibres — the site where pharyngeal pouches develop.
Clinical Presentation of Dysphagia
Dysphagia is defined as difficulty in swallowing — the sensation that food or liquid is not passing normally from the mouth to the stomach. It must be distinguished from odynophagia (painful swallowing, e.g., in acute tonsillitis or oesophagitis), globus pharyngeus (a persistent sensation of a lump in the throat without true difficulty in swallowing, usually functional in origin), and aphagia (complete inability to swallow). These distinctions matter because they point to entirely different aetiologies and urgencies, and conflating them leads to missed diagnoses or inappropriate investigations. Dysphagia is a symptom, not a diagnosis, and the clinical history is usually sufficient to generate a working diagnosis before the first investigation is ordered. The structured history — covering onset, the solid-versus-liquid distinction, the site of sticking, progression, associated symptoms, and risk factors — is the foundation on which all subsequent investigation and management rests. When these seven questions are asked in order and the answers are interpreted systematically, the probability of missing a serious or treatable cause falls dramatically. This history framework is the core clinical skill assessed in EN4.37.
- Onset and duration: Acute onset (hours to days) suggests foreign body impaction, acute tonsillitis, Ludwig's angina, or quinsy. Gradual onset over weeks to months raises the suspicion of malignancy or achalasia. Intermittent episodes over years suggest a benign structural cause (Schatzki ring, pharyngeal pouch).
- Solid vs liquid discrimination: This is the single most diagnostically important question. Solid-only dysphagia indicates mechanical obstruction (carcinoma, peptic stricture, Schatzki ring, foreign body, pharyngeal web). Dysphagia to both solids AND liquids from the outset indicates a motility disorder (achalasia, diffuse oesophageal spasm, neurological disease). Progressive solid-only dysphagia that evolves to include liquids indicates a mechanical lesion that is rapidly enlarging.
- Site of sticking: High cervical sensation suggests oropharyngeal or hypopharyngeal pathology; substernal sensation more reliably localises to the mid or lower oesophagus.
- Progression: Rapidly progressive solid-to-liquid dysphagia in an elderly person is an alarm symptom for malignancy. Slowly progressive dysphagia over years suggests achalasia or a benign peptic stricture.
- Associated symptoms: Weight loss (alarm feature for malignancy), regurgitation of undigested food (pharyngeal pouch, achalasia), nasal regurgitation of liquids (palatal palsy), hoarseness (recurrent laryngeal nerve involvement), coughing on swallowing (oropharyngeal aspiration), blood-stained sputum or haematemesis.
- Risk factors: Tobacco and alcohol use (carcinoma), iron-deficiency anaemia in middle-aged women (Plummer-Vinson syndrome), chronic GORD (peptic stricture, Barrett's oesophagus), systemic sclerosis.
- Age and sex: Younger patients with solid-food dysphagia are more likely to have benign causes. Patients over 40 with progressive solid dysphagia must have malignancy excluded urgently.
Anatomy and Pathophysiology of Swallowing
Understanding why dysphagia occurs requires a working anatomical model of the swallowing apparatus and the two fundamental mechanisms by which it fails. The swallowing passage runs from the oral cavity through the oropharynx, the hypopharynx (the part of the pharynx at the level of the larynx), the cricopharyngeus (upper oesophageal sphincter), the oesophagus (approximately 25 cm long), the lower oesophageal sphincter (LOS), and the gastric cardia. At each level, the bolus must pass through an opening of sufficient diameter with a propulsive force sufficient to move it onward. When either the lumen size or the propulsive mechanism is compromised, dysphagia results. These two failure modes map directly onto the solid-vs-liquid discrimination in the history — a fact that makes the history both cheap and powerful as a diagnostic tool.
Two pathophysiological mechanisms of dysphagia:
1. Mechanical obstruction (also called transport dysphagia in oesophageal disease): the lumen is physically narrowed by a lesion — intrinsic (growing from the wall into the lumen) or extrinsic (pressing the wall inward from outside). Solid boluses are held up before liquids because a solid cannot deform to squeeze through a narrowed lumen, whereas liquid can. Intrinsic causes include carcinoma, peptic stricture, Schatzki ring, mucosal web, foreign body. Extrinsic causes include retrosternal goitre, mediastinal nodes, aortic aneurysm, enlarged left atrium.
2. Neuromuscular (motility) dysfunction (also called transfer dysphagia at the oropharyngeal level): the propulsive mechanism is defective — peristalsis is absent, discoordinated, or the sphincters fail to relax appropriately. Both solids and liquids are affected from the outset because the problem is not lumen size but propulsion. Oropharyngeal neuromuscular dysphagia arises from bulbar palsy (stroke, MND, myasthenia gravis). Oesophageal motility disorders include achalasia (absent LOS relaxation + absent peristalsis) and diffuse oesophageal spasm.
Killian's dehiscence is an anatomical weak point in the posterior pharyngeal musculature between the oblique fibres of the thyropharyngeus and the horizontal fibres of the cricopharyngeus. Increased intrapharyngeal pressure during swallowing, combined with a poorly co-ordinated cricopharyngeus, can cause the posterior pharyngeal mucosa to herniate through this dehiscence — producing a pharyngeal pouch (Zenker's diverticulum).
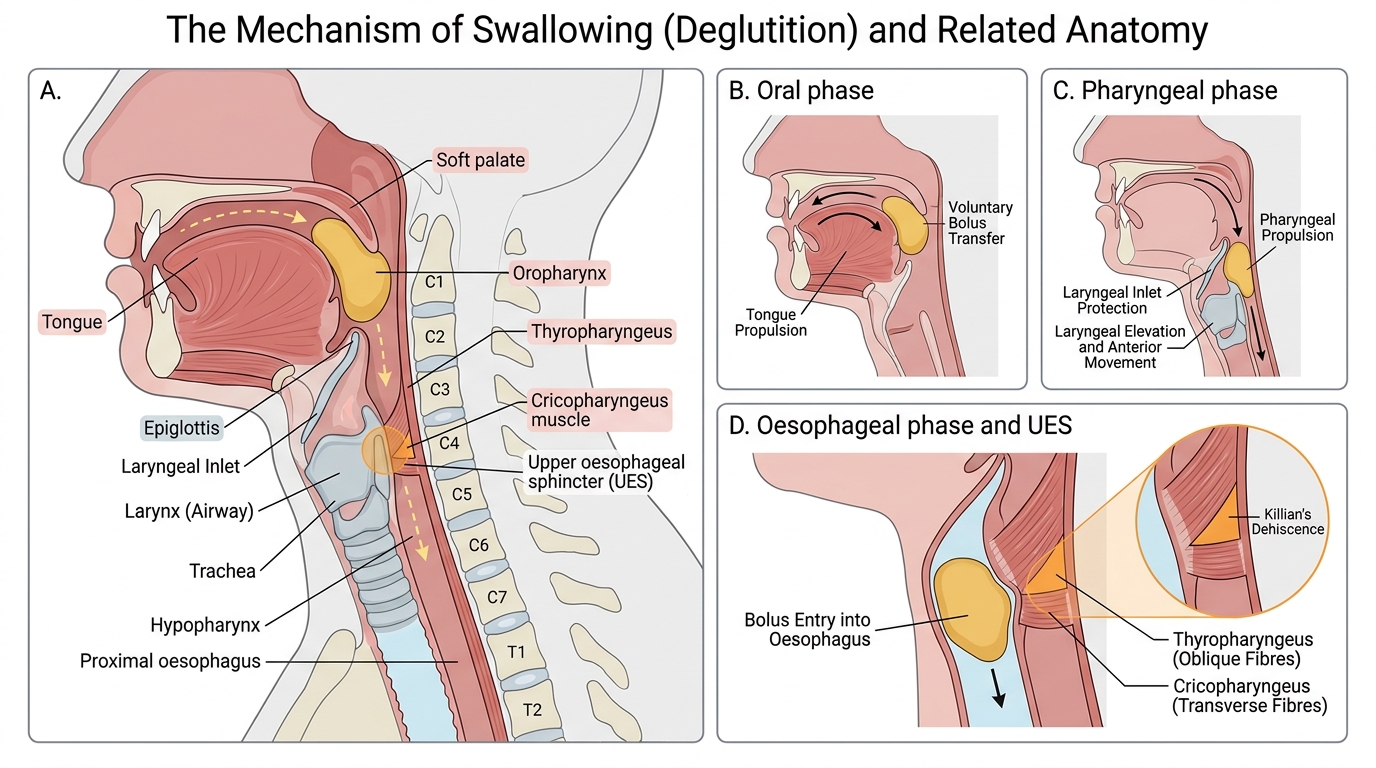
Swallowing Phases and Upper Oesophageal Sphincter Anatomy
Causes of Dysphagia — Classification and Key Conditions
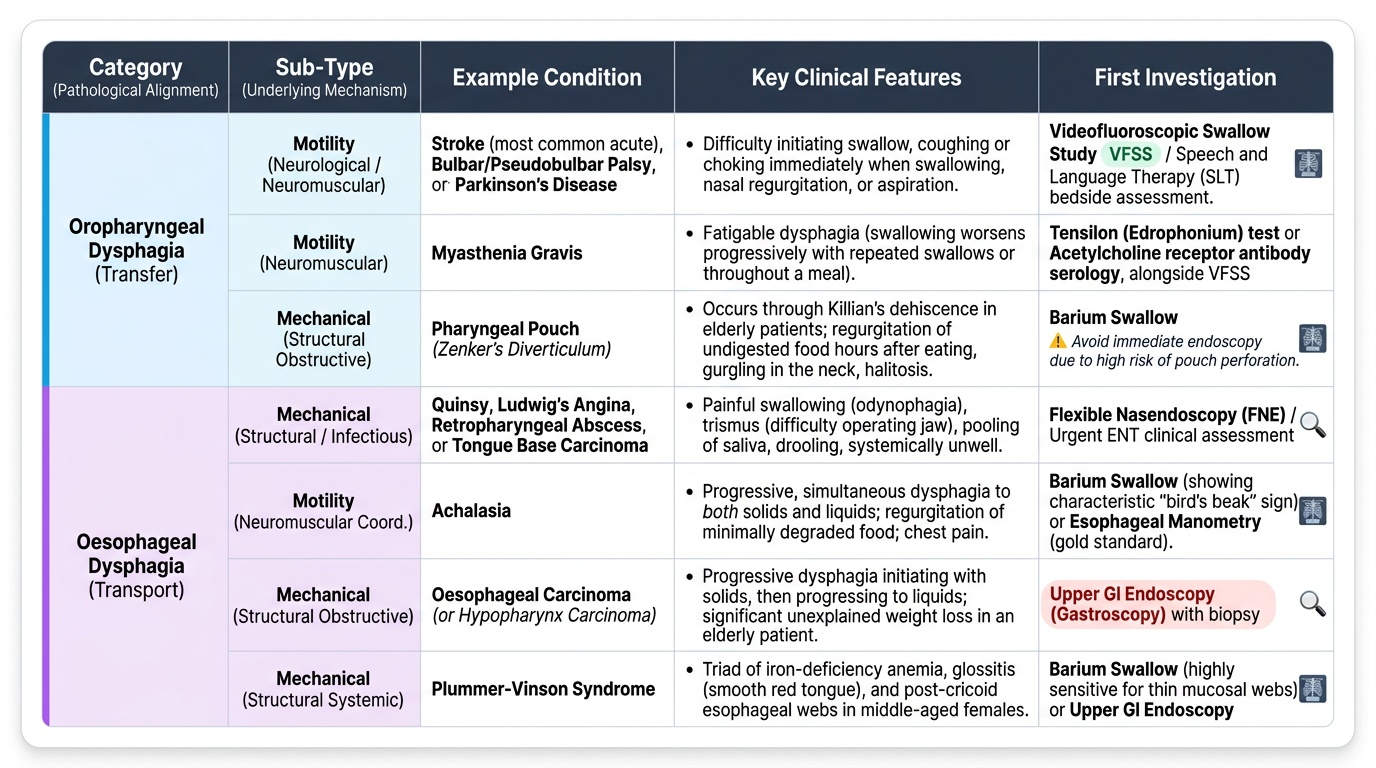
A systematic classification based on anatomical level (oropharyngeal vs oesophageal) and mechanism (mechanical vs motility) organises the differential diagnosis and guides the choice of investigation. This classification maps directly onto the history framework: oropharyngeal causes produce transfer dysphagia (difficulty initiating the swallow, coughing immediately on swallowing, nasal regurgitation, or aspiration), while oesophageal causes produce transport dysphagia (sensation of food sticking in the chest or back after the swallow is initiated). Understanding which category a patient falls into from the history determines which investigation to order first and avoids the common error of ordering the wrong test. The conditions described below — particularly carcinoma of the hypopharynx and oesophagus, achalasia, pharyngeal pouch, and Plummer-Vinson syndrome — are the ones most likely to appear in clinical examinations and, more importantly, in your outpatient practice as a final-year student and junior doctor. Knowing their distinguishing clinical features by heart is a non-negotiable component of clinical competence in ENT.
Provided image
I. Oropharyngeal dysphagia (transfer dysphagia)
- Neurological: stroke (most common cause of acute oropharyngeal dysphagia), bulbar palsy (MND, syringobulbia), pseudobulbar palsy, Parkinson's disease.
- Neuromuscular: myasthenia gravis (fatigable dysphagia worse with repeated swallows).
- Structural: carcinoma of the tongue base or posterior pharyngeal wall, quinsy, Ludwig's angina, retropharyngeal abscess.
- Pharyngeal pouch (Zenker's diverticulum): a pulsion diverticulum through Killian's dehiscence. Presents in elderly patients with dysphagia, regurgitation of undigested food (sometimes hours after eating), gurgling in the neck, halitosis, and Boyce's sign (soft compressible neck swelling that reduces on pressure). Risk of aspiration pneumonia.
- Plummer-Vinson syndrome (Paterson-Brown-Kelly syndrome): the triad of postcricoid web + iron-deficiency anaemia + dysphagia, predominantly in middle-aged women. The web is considered premalignant — increased risk of postcricoid carcinoma. Visible as a shelf-like filling defect on lateral barium swallow.
II. Oesophageal dysphagia — Mechanical/structural causes:
- Carcinoma of the oesophagus: the most important cause to exclude in progressive solid-food dysphagia in patients over 40. Squamous cell carcinoma (SCC) in the upper and middle thirds (alcohol + tobacco); adenocarcinoma in the lower third (Barrett's oesophagus from chronic GORD). Progressive solid dysphagia, weight loss, and advancing to liquid dysphagia. Barium swallow shows an irregular filling defect with 'shouldering' (rat-tail or apple-core appearance).
- Carcinoma of the hypopharynx: arises in the pyriform fossa (most common), posterior pharyngeal wall, or postcricoid region. Solid dysphagia, weight loss, referred otalgia (via Arnold's nerve), hoarseness.
- Peptic stricture: benign fibrous narrowing of the lower oesophagus from chronic GORD. Smooth tapered narrowing on barium swallow.
- Schatzki ring (B ring): a thin mucosal ring at the gastro-oesophageal junction causing episodic (not progressive) solid dysphagia — the 'steakhouse syndrome.'
- Oesophageal foreign body: impaction at the three natural oesophageal narrowings — cricopharyngeus, level of the aortic arch, and gastro-oesophageal junction.
- Extrinsic compression: retrosternal goitre, mediastinal lymphadenopathy, aortic aneurysm, enlarged left atrium (mitral stenosis).
III. Oesophageal dysphagia — Motility causes:
- Achalasia: failure of LOS relaxation + absent peristalsis due to degeneration of Auerbach's myenteric plexus. Dysphagia to both solids AND liquids from the outset, regurgitation of undigested food, nocturnal cough. Barium swallow shows dilated oesophagus with smooth 'bird-beak' narrowing at the cardia.
- Diffuse oesophageal spasm: uncoordinated simultaneous contractions; chest pain + intermittent dysphagia to both solids and liquids; barium shows 'corkscrew oesophagus.'
SELF-CHECK
A 62-year-old male smoker presents with a 10-week history of progressive difficulty swallowing solids, now also affecting semi-solids. He has lost 7 kg. He points to his mid-sternum as the site of sticking. The single most important next investigation is:
A. CT scan of the thorax and abdomen
B. Upper GI endoscopy (oesophagoscopy) with biopsy
C. Barium swallow
D. Oesophageal manometry
Reveal Answer
Answer: B. Upper GI endoscopy (oesophagoscopy) with biopsy
This patient has the classic alarm triad for oesophageal malignancy: progressive solid dysphagia, weight loss, and age over 40 with a smoking history. Upper GI endoscopy with biopsy is the investigation of choice — it visualises the lesion directly, allows tissue diagnosis (histology), and permits staging biopsy. CT scan follows AFTER histological confirmation (for staging). Barium swallow may suggest the diagnosis but does not provide tissue. Manometry is for motility disorders (achalasia), not mechanical obstruction.