Page 7 of 17
EN4.39 | Tonsillectomy and Adenoidectomy — SDL Guide
Learning Objectives
- State the indications for tonsillectomy and adenoidectomy and the criteria for each indication
- Identify the key instruments used in tonsillectomy and adenoidectomy and describe the principle underlying each
- Describe the step-by-step technique of tonsillectomy (dissection technique) and adenoidectomy (curettage technique) in a supervised or simulated setting
- Identify and describe the management of the major complications of tonsillectomy and adenoidectomy, particularly primary, reactionary, and secondary haemorrhage
- Describe the post-operative counselling and discharge instructions for a patient and family following tonsillectomy
INSTRUCTIONS
Tonsillectomy is one of the most commonly performed surgical procedures in ENT worldwide. At the KH (Knowledge for the Help of the Patient) level, EN4.39 requires you to observe and describe the indications, operative steps, and complications — not to perform the operation independently. This SDL builds the mental model of the operation that enables you to assist safely in theatre, counsel patients and families accurately about what to expect, and recognise and respond to post-operative complications, particularly the feared secondary haemorrhage that occurs 5–10 days after surgery.
References
- Dhingra PL. Diseases of Ear, Nose & Throat, 7th ed. Ch — Tonsils and Adenoids — Surgical Techniques (textbook)
- Hazarika P. Textbook of Ear, Nose & Throat and Head-Neck Surgery. Ch — Tonsillectomy and Adenoidectomy (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed. Vol 2 — Tonsillectomy: Surgical Techniques and Complications (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is day 8 after tonsillectomy in a 10-year-old boy. He was discharged on day 1 with no concerns. Tonight, his parents call the emergency department to say he has had two episodes of blood in his mouth and has spat out approximately 50 mL of fresh red blood. He is conscious and speaking but pale and anxious. His parents ask: 'Is this normal? Can we just wait and see?' What do you tell them, and what must happen in the next 30 minutes?
WHY THIS MATTERS
Tonsillectomy is among the top five most frequently performed operations in the ENT specialty, and adenoidectomy is often combined with it or performed independently in children with adenoid hypertrophy, recurrent otitis media with effusion, or obstructive sleep apnoea. As a final-year MBBS student and junior doctor, you will encounter post-tonsillectomy complications — particularly secondary haemorrhage — in the emergency department and surgical ward. You will be expected to counsel patients about what to expect after the operation, to recognise when a complication is developing, and to act appropriately. EN4.39 is set at the KH (Knowledge for the Help of the Patient) level — you must be able to observe the procedure and describe its indications, steps, and complications accurately, even though you will not perform it independently until you are a specialist trainee.
RECALL
Recall from the previous SDL (EN4.38) that the palatine tonsil lies within a fibrous capsule between the anterior and posterior tonsillar pillars, and that the peritonsillar space separates this capsule from the superior pharyngeal constrictor muscle. Tonsillectomy proceeds within this peritonsillar space — the correct surgical plane is between the capsule and the constrictor, which is relatively avascular when dissected carefully. The dominant blood supply is the tonsillar branch of the facial artery entering the lower pole, with contributions from the ascending palatine, lingual, and ascending pharyngeal arteries from above and below. Haemostasis at these vessels is the critical step in the operation. Recall also from Anatomy that the nasopharyngeal tonsil (adenoid) sits on the posterior wall of the nasopharynx, extending from the roof to the level of the choanae; it lies behind the posterior choanae and cannot be directly visualised through the mouth without special mirrors or endoscopes — which is why adenoidectomy is traditionally performed as a blind curettage technique.
Clinical Indication and Relevance of Tonsillectomy and Adenoidectomy
The decision to recommend tonsillectomy or adenoidectomy is one of the most common surgical decisions in ENT, and it must be based on validated evidence-based criteria rather than on clinical intuition or parental preference alone. The consequences of getting this wrong are significant in both directions: operating on a child who does not meet criteria exposes them to the risks of a general anaesthetic and surgery unnecessarily, while withholding surgery from a child with significant OSA allows progressive neurocognitive effects of sleep-disordered breathing to continue. Errors in indication — operating too early (before criteria are met) or too late (leaving a child with obstructive sleep apnoea without treatment) — are associated with preventable harm in either direction. At the KH level, you must know the indications well enough to advise a patient or parent correctly and to recognise when a referral for a surgical opinion is appropriate.
Indications for tonsillectomy:
- Recurrent tonsillitis — Paradise criteria (the primary indication in children and adults): ≥7 documented episodes in the preceding year, OR ≥5 documented episodes per year for 2 consecutive years, OR ≥3 documented episodes per year for 3 consecutive years. Each episode must be documented and must include sore throat plus at least one of: fever >38.3°C, cervical lymphadenopathy, tonsillar exudate, or positive throat swab for GABHS.
- Peritonsillar abscess (quinsy): a first quinsy is managed with needle aspiration followed by interval tonsillectomy 6–8 weeks later. Recurrent quinsy (≥2 episodes) is an absolute indication.
- Obstructive sleep apnoea (OSA) / sleep-disordered breathing due to tonsillar hypertrophy: especially in children with grade 3–4 tonsillar enlargement, significant desaturation on oximetry, or formal polysomnography confirmation. This is the most common indication for tonsillectomy in children under 5 years.
- Suspicion of malignancy: unilateral tonsillar enlargement in an adult — particularly when hard, fixed, or accompanied by cervical lymphadenopathy — requires tonsillectomy for histological diagnosis to exclude tonsillar lymphoma or squamous cell carcinoma.
- Other: halitosis from chronic tonsillitis unresponsive to conservative treatment; tonsillar calculi (tonsilloliths).
Indications for adenoidectomy:
- Nasopharyngeal obstruction: persistent mouth breathing, snoring, hyponasal speech, and sleep-disordered breathing due to adenoid hypertrophy.
- Recurrent otitis media with effusion (glue ear): adenoidectomy reduces the reinsersion rate of grommets; recommended in children ≥4 years old requiring repeat grommet insertion.
- Recurrent adenoiditis: frequent acute infections with nasal discharge, posterior nasal drip, and nasopharyngeal symptoms.
- Chronic rhinosinusitis in children where adenoid hypertrophy is a contributing factor.
Contraindications and pre-operative assessment:
- Cleft palate (absolute contraindication for adenoidectomy): removal of the adenoid in a child with a cleft palate or submucous cleft palate risks velopharyngeal insufficiency (VPI) — hypernasal speech and nasal regurgitation due to inadequate velopharyngeal closure. Always exclude a submucous cleft (bifid uvula, zona pellucida, notch in posterior border of hard palate) before adenoidectomy.
- Bleeding diathesis (pre-operative haemostasis screen in any child with a family or personal history of bleeding disorders).
- Active acute tonsillitis — operation should be delayed 4–6 weeks.
- Pre-operative assessment: FBC, blood group and save (or cross-match if high risk), anaesthetic assessment.
Instruments and Principles of Tonsillectomy and Adenoidectomy
The instruments used in tonsillectomy and adenoidectomy reflect the anatomical approach and the principles of the procedure — maintaining the correct tissue plane, providing adequate exposure, and achieving haemostasis. Familiarity with these instruments and their purpose is the baseline knowledge required to scrub in and assist effectively. The instrument set has evolved over decades but the core tools remain similar across most ENT units; newer energy-based devices (diathermy, coblation) have supplemented but not entirely replaced the classical instruments. A working knowledge of what each instrument does — and why — allows you to anticipate the surgeon's next step, prepare the correct instrument, and recognise when a complication is developing (e.g. that brisk arterial bleeding from the lower pole that the Negus forceps must control immediately).
Instruments for tonsillectomy:
- Boyle-Davis mouth gag: a self-retaining retractor that holds the mouth open during the operation. It has a central blade that depresses the tongue, and a ratcheted frame that holds the jaw open. It is suspended from a Draffin bipod or a stand attached to the table, freeing both surgeon's hands. The tongue blade size must be matched to the patient — too large crushes the tongue; too small gives inadequate exposure.
- Mollison's pillar retractor: a small retractor used to retract the anterior tonsillar pillar (palatoglossus) to expose the peritonsillar space and capsule.
- Curved tonsil scissors (Mety's or curved Mayo scissors): used to incise the anterior pillar mucosa and develop the plane between the tonsil capsule and the superior constrictor.
- Tonsil dissector (Mollison's haemostatic dissector): blunt dissection instrument used to develop the peritonsillar plane without tearing the capsule.
- Negus artery forceps: long curved haemostats used to clamp tonsillar vessels before tying or diathermising.
- Eve's tonsillar snare: a wire loop placed around the lower pole pedicle to sever the last attachment of the tonsil — used in the older 'dissect-and-snare' technique.
- Diathermy probe: monopolar or bipolar diathermy to achieve haemostasis of smaller vessels. Bipolar diathermy is preferred over monopolar for the tonsillar bed to minimise thermal spread and risk to surrounding structures.
- Coblation wand (in modern units): uses radiofrequency energy at a low temperature (~60°C) to ablate tissue with less thermal damage to surrounding structures than conventional diathermy.
Instruments for adenoidectomy:
- Adenoid curette (St Clair Thompson's curette): the traditional instrument — a curved metal scoop with a serrated leading edge, inserted blindly behind the soft palate and drawn forward firmly to remove the adenoid tissue from the posterior nasopharyngeal wall. Sizes vary; the appropriate size is selected based on age and estimated adenoid bulk.
- Post-nasal mirror: used to inspect the post-nasal space before and after curettage to assess adenoid bulk and confirm removal.
- Microdebrider or coblation: endoscopic-guided adenoidectomy under direct vision, increasingly used in units with appropriate equipment.
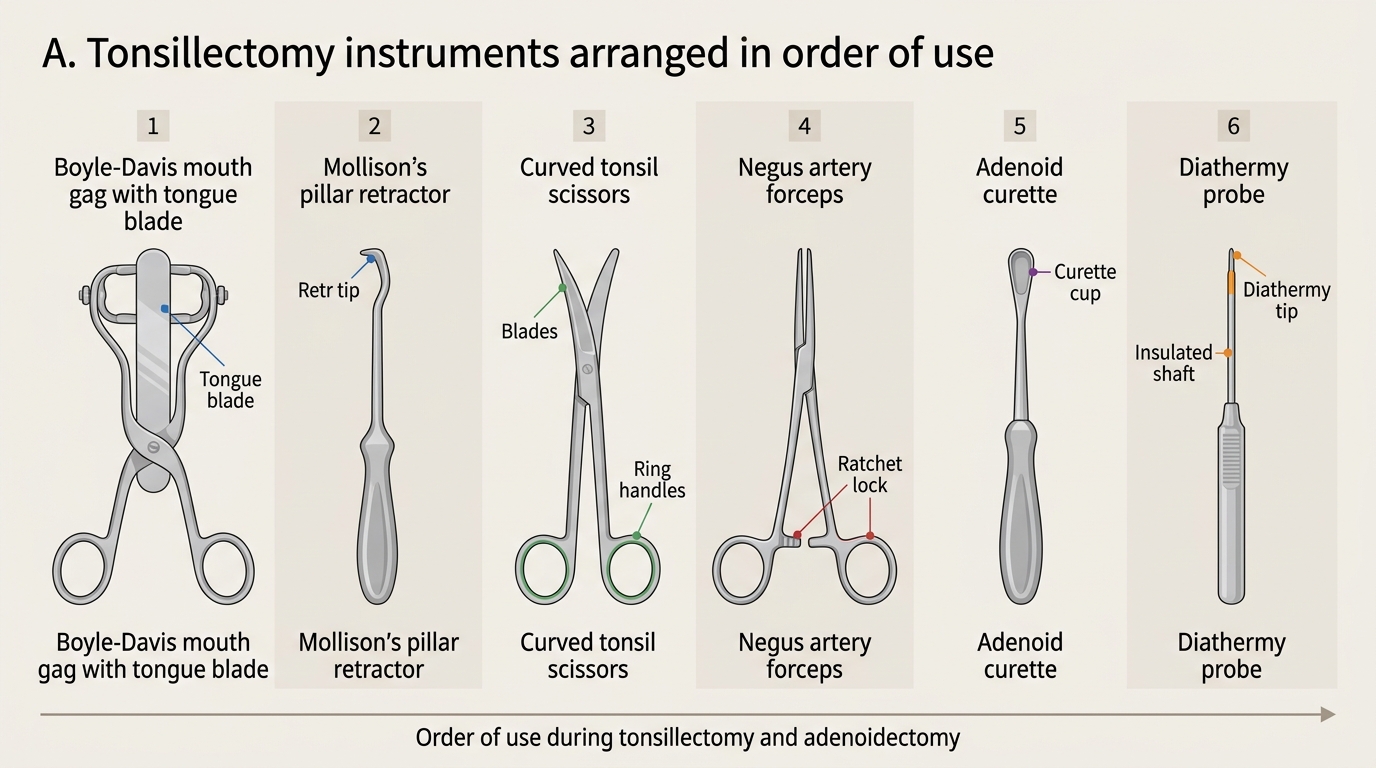
Tonsillectomy Instruments in Order of Use
SELF-CHECK
During a tonsillectomy, the surgeon asks you to identify the key surgical plane. The correct plane for tonsil dissection is:
A. Between the tonsillar capsule and the palatoglossus muscle (anterior pillar)
B. Between the tonsillar capsule and the superior pharyngeal constrictor (peritonsillar space)
C. Within the lymphoid tissue of the tonsil itself
D. Between the mucosal surface of the tonsil and the underlying lymphoid tissue
Reveal Answer
Answer: B. Between the tonsillar capsule and the superior pharyngeal constrictor (peritonsillar space)
The correct surgical plane for tonsillectomy is the peritonsillar space — the potential space between the fibrous capsule of the tonsil and the superior pharyngeal constrictor muscle. This plane is relatively avascular and allows safe extracapsular dissection with minimal bleeding if correctly entered. Dissection within the tonsillar tissue (intracapsular) risks leaving remnants and increases bleeding. The anterior pillar (palatoglossus) is retracted out of the way, not dissected through. Identifying and maintaining this plane is the defining technical skill of tonsillectomy.
Surgical Technique — Tonsillectomy and Adenoidectomy
Both tonsillectomy and adenoidectomy are performed under general anaesthesia with endotracheal intubation. The patient is positioned supine with a shoulder roll to extend the neck and improve oropharyngeal access. A throat pack is placed to prevent blood from entering the airway during the procedure. The surgeon typically sits at the head of the table; the anaesthetist is at the foot or to the side. Understanding the sequential steps of the operation helps the final-year student follow what is happening when observing in theatre and prepares them to scrub in and assist safely. Knowing the steps also enables you to anticipate complications — for example, a sudden increase in bleeding during lower pole dissection should prompt the surgeon to immediately secure the tonsillar branch of the facial artery, and a scrub nurse or assistant who understands this will have the Negus forceps ready.
Tonsillectomy — dissection technique (step-by-step):
- Insert the Boyle-Davis mouth gag: with the tongue blade appropriately sized, open the mouth and suspend the gag from the Draffin stand. Ensure adequate tongue depression and oropharyngeal exposure. Apply a throat pack to protect the airway.
- Identify the anterior tonsillar pillar (palatoglossus) and grasp the upper pole of the tonsil with Allis forceps. Apply gentle medial traction to pull the tonsil away from the superior constrictor — this opens the peritonsillar space.
- Incise the mucosa of the anterior pillar with curved scissors, just medial to the palatoglossus muscle, to enter the peritonsillar plane.
- Dissect bluntly in the peritonsillar space using the Mollison dissector, separating the tonsil capsule from the superior constrictor fibres. The dissection proceeds from the upper pole downward on the lateral aspect, and from the anterior pillar across to the posterior pillar.
- Control bleeding vessels as they are encountered: clamp with Negus forceps, tie with absorbable suture, or diathermy (bipolar preferred). The major vessels enter at the lower pole.
- Complete the lower pole dissection: the tonsillar pedicle at the lower pole is divided either with scissors under a ligature or with diathermy. This is where the tonsillar branch of the facial artery typically enters and must be secured.
- Inspect the tonsillar fossa: ensure complete haemostasis. Check the posterior pillar. Apply pressure with a gauze pack for 1–2 minutes. Suture ligation if persistent bleeding.
- Remove the throat pack at the end of the procedure. Verify the airway is clear and suction any blood from the oropharynx before extubation.
Adenoidectomy — curettage technique (step-by-step):
- Position the patient supine with a shoulder roll. Insert the Boyle-Davis gag. Have the post-nasal mirror and suction available.
- Select the appropriate adenoid curette (St Clair Thompson's curette — the size matching the estimated post-nasal space). Hold with the dominant hand, insert it through the oral cavity behind the soft palate, guided with a finger into the post-nasal space.
- Apply firm forward and downward stroke with the curette, hugging the posterior nasopharyngeal wall — the adenoid tissue is swept into the oral cavity. Apply immediately with a gauze swab and suction.
- Inspect the post-nasal space using a mirror or post-nasal endoscope: confirm the adenoid bulk has been adequately removed. Avoid excessive curettage near the Eustachian tube orifices (lateral walls) — only the posterior and superior walls are curetted.
- Haemostasis: typically achieved by sustained pressure with a moistened pack held for 3–5 minutes. Active bleeding may require bipolar diathermy under direct endoscopic vision.
Intraoperative hazards:
- Trauma to the soft palate or posterior pharyngeal wall from an oversized curette or forceful curettage
- Damage to the Eustachian tube orifice from lateral curettage — avoid
- Excessive tonsillar bed bleeding from failure to maintain the correct surgical plane or inadequate vessel ligation
- Airway soiling with blood — prevented by throat pack; must be counted before extubation
SELF-CHECK
During an adenoidectomy, you are instructed to avoid curettage of the lateral walls of the nasopharynx. The primary reason for this instruction is to:
A. Prevent damage to the internal carotid artery which runs lateral to the nasopharynx
B. Avoid injury to the Eustachian tube orifices which open on the lateral walls
C. Preserve the tubal tonsils which perform immunological functions
D. Prevent damage to the trigeminal nerve branches which run laterally
Reveal Answer
Answer: B. Avoid injury to the Eustachian tube orifices which open on the lateral walls
The Eustachian tube orifices (the pharyngeal openings of the Eustachian tubes) are located on the lateral walls of the nasopharynx, just posterior to the inferior turbinate. The adenoid tissue (nasopharyngeal tonsil) lies on the posterior and superior walls of the nasopharynx. During adenoidectomy curettage, only the posterior and superior walls are curetted; lateral curettage risks traumatising the Eustachian tube orifices, potentially causing scarring and Eustachian tube dysfunction — the very condition that adenoidectomy is intended to treat. The carotid artery and trigeminal nerve are not at risk from an appropriately performed curettage.