Page 4 of 15
PE1.2 | Growth Assessment and Anthropometry — SDL Guide
Learning Objectives
- Describe the methods of growth assessment and the principles underlying the WHO and IAP reference standards
- Enumerate the anthropometric parameters used for assessing physical growth in infants, children, and adolescents
- Perform anthropometric measurements (weight, length/height, head circumference, MUAC) using correct technique
- Document measurements on appropriate growth charts and interpret findings using standardised SD/percentile cut-offs
- Classify nutritional status as SAM, MAM, or normal using WHO/IMNCI criteria and initiate appropriate action
INSTRUCTIONS
Anthropometry is the clinical skill that transforms growth monitoring from an abstract concept into an actionable assessment. A correctly measured, correctly plotted weight-for-height is a diagnostic test for acute malnutrition—as objective as a blood glucose for diagnosing diabetes. This module takes you through the instruments, technique, standards, and interpretation framework, culminating in the practical skill of reading a growth chart and classifying a child's nutritional status in a clinical or community setting.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 2–3 (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 24 (textbook)
- WHO Child Growth Standards (MGRS), WHO Press 2006 (guideline)
- IAP 2015 Growth Charts for Height, Weight and BMI for 5–18 Year Indian Children (guideline)
- WHO/UNICEF/WFP Joint Statement: Community-Based Management of SAM, 2007 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
At a district hospital outpatient clinic, a community health worker brings in a 2-year-old boy she is worried about. 'He doesn't look right,' she says—but she has no written record and cannot say when he was last weighed. You measure him: weight 7.8 kg, length 80 cm, MUAC 11.0 cm, no bilateral pedal oedema. Is this child malnourished? Severely? Moderately? Does he need inpatient admission right now? The answers to all these questions flow directly from knowing how to measure, which chart to use, and what the numbers mean. That is the skill this module builds.
WHY THIS MATTERS
Anthropometric assessment is the most widely used clinical and epidemiological tool in global child health. At the individual level, it identifies malnutrition before clinical signs of severe deficiency appear, guides therapeutic feeding decisions, and provides an objective endpoint for monitoring treatment response. At the population level, the prevalence of stunting, wasting, and underweight are core indicators of the Sustainable Development Goals, the National Nutrition Mission (POSHAN Abhiyan), and the National Family Health Survey. In India, every Anganwadi worker, every Auxiliary Nurse-Midwife, and every doctor at a Primary Health Centre performs these measurements as part of routine child health surveillance. Mastery of this skill is therefore a professional competency that will be exercised throughout your career.
RECALL
From the preceding module on growth terminology, recall:
• Growth velocity is the rate of change over time; more sensitive for detecting faltering than a single attained measurement.
• Normal weight landmarks: birth weight doubles at ~5 months, triples at ~12 months.
• SAM (Severe Acute Malnutrition) is defined by weight-for-height <−3 SD, or MUAC <11.5 cm (6–59 months), or bilateral pedal oedema.
From clinical training, recall that Holliday-Segar maintenance fluids (100/50/20 mL/kg/day) are weight-based—underscoring why accurate weight measurement is essential before any inpatient therapeutic plan.
Why Standardised Anthropometry Is the Cornerstone of Child Health Surveillance
Anthropometry—the science of measuring the human body's physical dimensions—provides the only objective, non-invasive, inexpensive, and universally applicable method for assessing nutritional status and growth in children. Unlike biochemical markers, which require laboratory infrastructure, or clinical signs of malnutrition (which appear only after significant tissue depletion), anthropometric measurements can be obtained with simple instruments in any setting, from a village Anganwadi to a tertiary neonatal unit.
The clinical indications for growth assessment are essentially universal in paediatric practice. At every well-child visit, at every immunisation contact, at every hospital admission, and at every nutritional rehabilitation review, a child's weight and, depending on age, length/height and head circumference should be measured, plotted, and interpreted. The IMNCI (Integrated Management of Neonatal and Childhood Illness) algorithm—used by front-line health workers across India—incorporates MUAC measurement as a rapid field-screening tool for acute malnutrition, enabling early identification and referral before the child reaches the stage of severe wasting with complications.
At the programme level, anthropometry is the key output metric for ICDS (Integrated Child Development Services), which monitors the weight of all children under 6 years through monthly Anganwadi-level weighing. The POSHAN Abhiyan (National Nutrition Mission, launched 2018) has a direct target of reducing stunting prevalence in under-5s by 2% per year. These national targets are measured through anthropometry—making the clinician who performs measurements accurately a direct contributor to national health surveillance validity.
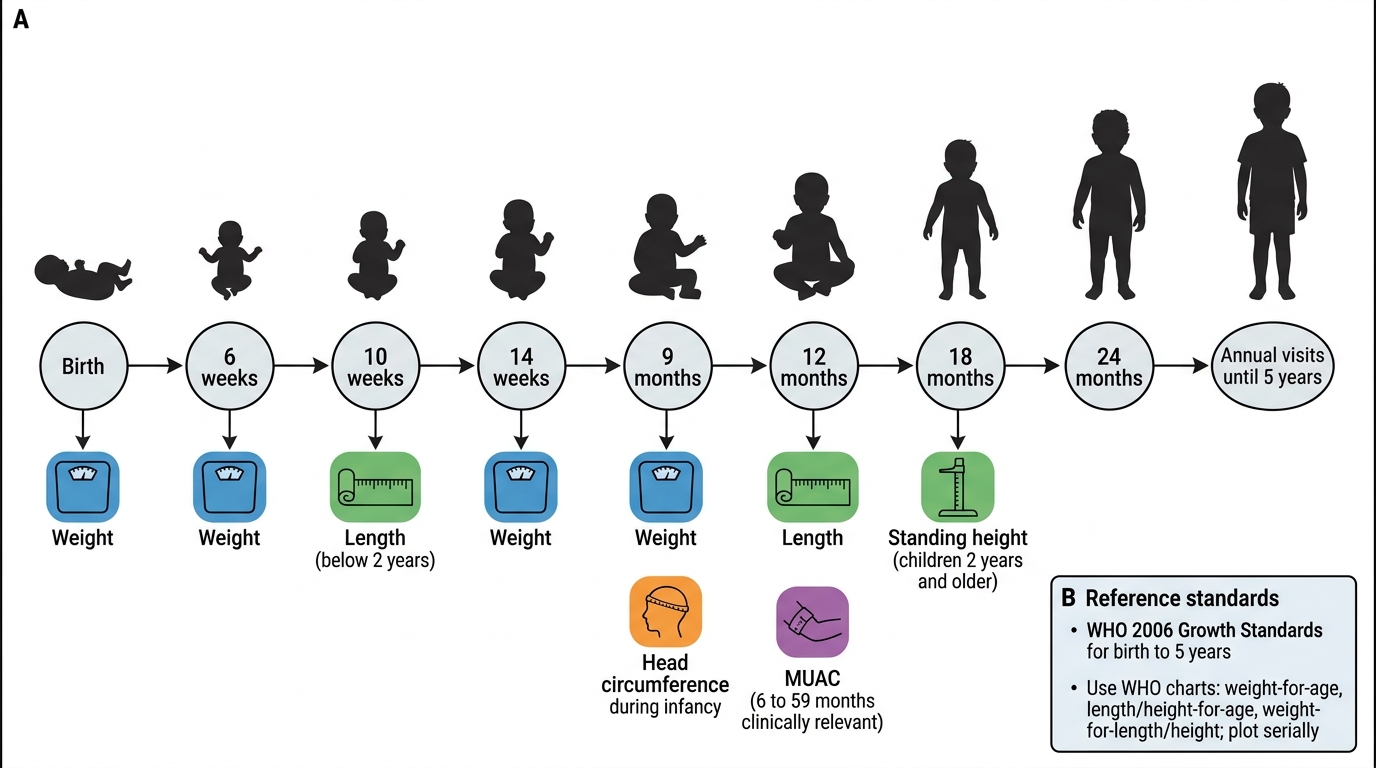
Child Growth Surveillance Contacts from Birth to 5 Years
Reference Standards: WHO and IAP Growth Charts
Growth charts are only meaningful when measurements are compared against an appropriate reference standard—a dataset of measurements from a healthy, well-nourished reference population. Two standards are relevant for Indian paediatric practice, and understanding which to use and why is essential before picking up a chart.
Provided image
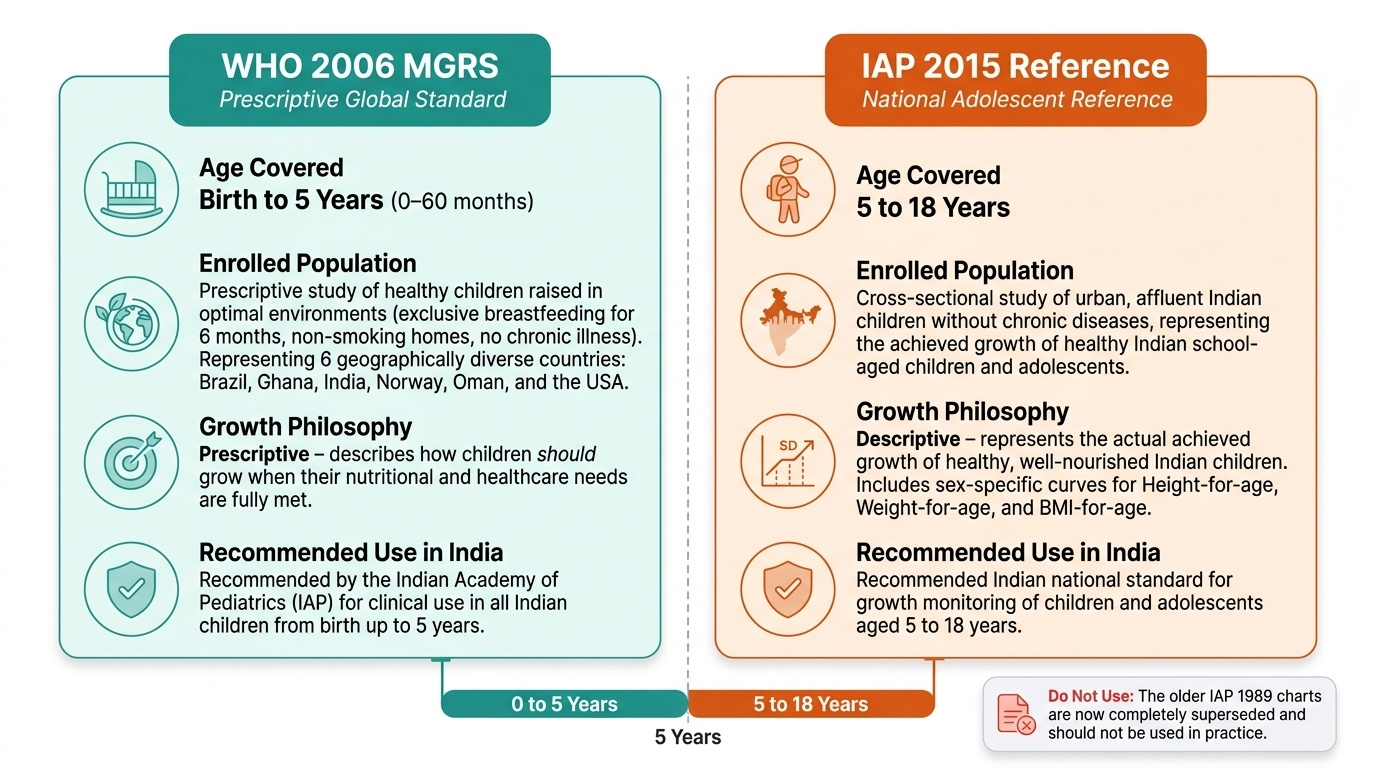
WHO 2006 Multicentre Growth Reference Study (MGRS): This is the international standard for children from birth to 5 years, and it is the reference currently recommended by the Indian Academy of Pediatrics (IAP) for this age group. It was derived from a prescriptive study—meaning it enrolled children raised in optimal conditions (exclusive breastfeeding for 6 months, non-smoking households, no chronic disease) across six geographically diverse countries: Brazil, Ghana, India, Norway, Oman, and the USA. The MGRS is deliberately prescriptive rather than descriptive: it describes how children should grow when their needs are met, not simply how they do grow in any given population. This distinction matters—it means the WHO standard is appropriate for all children globally, including Indian children, and is not 'too generous' for a resource-limited setting.
IAP 2015 Growth Reference: The IAP 2015 charts are the recommended Indian reference for children aged 5–18 years. They were derived from a cross-sectional study of urban, affluent Indian children without chronic disease—designed to represent the achieved growth of healthy Indian children in the school-age and adolescent range, which is not covered by the WHO MGRS. For this age group, IAP 2015 provides height-for-age, weight-for-age, and BMI-for-age charts with sex-specific curves.
Practical rule: Use WHO 2006 charts for all children from birth to 5 years. Use IAP 2015 charts for children 5–18 years. Do not use the older IAP 1989 charts, which are now superseded.
Understanding percentiles vs SD scores: Both systems express a child's position relative to the reference population. Percentiles state what percentage of the reference population falls below the child's value (e.g. 3rd percentile = 97% of healthy children are larger). SD scores (z-scores) express how many standard deviations from the reference mean the child's value lies. For clinical decision-making in malnutrition, SD scores are preferred because they are more precise at the extremes of the distribution—a child at −3 SD is in an unambiguously high-risk range regardless of percentile calculations. WHO-recommended cut-offs for malnutrition use SD scores.
Parameters for Assessing Physical Growth: What to Measure and When
Different anthropometric parameters are appropriate at different ages and serve distinct clinical purposes. Selecting the right parameter for the right age group is the first decision in any growth assessment, before picking up an instrument.
Weight is the single most important and universally applicable parameter. It reflects current nutritional status and is required at every clinical contact. In infants, it is measured using a digital infant scale with a weighing pan; in ambulant children, a standing scale is used. Weight in conjunction with height/length is used to calculate weight-for-height, the index most sensitive for acute malnutrition.
Length (recumbent) is used for children under 2 years who cannot stand reliably, measured using an infantometer (length board) with the child lying supine. Height (standing) is used for children 2 years and older, using a stadiometer or height board. The transition from length to height at 2 years introduces a systematic 0.7 cm measurement difference (length exceeds height by ~0.7 cm due to posture); this should be accounted for when comparing measurements across this boundary.
Head circumference (HC) is measured routinely from birth to 2 years (and up to 3 years if neurological concern exists), using a non-stretchable tape. It is the most important parameter for monitoring brain growth and detecting microcephaly or macrocephaly.
Mid-Upper Arm Circumference (MUAC) is the preferred rapid screening tool for acute malnutrition in children aged 6–59 months in community and emergency settings. It requires only a colour-coded MUAC tape, is less affected by oedema than weight-for-height, does not require a reference standard lookup, and can be performed by community health workers with minimal training. Cut-offs: MUAC <11.5 cm = SAM; 11.5–12.5 cm = MAM; ≥12.5 cm = normal.
Skin-fold thickness (triceps, subscapular) assesses body fat percentage and is used in research and specialised nutritional assessments; Harpenden calipers are required. It is not routinely used in primary care.
BMI (Body Mass Index) = weight (kg) / height (m²) is used from 2 years onward and is expressed as BMI-for-age using age- and sex-specific charts (IAP 2015 for school-age; WHO charts for 2–5 years). It is the preferred index for identifying overweight and obesity.
| Parameter | Instrument | Age group | Derived index | Clinical use |
|---|---|---|---|---|
| Weight | Digital infant/standing scale | All ages | Weight-for-age, weight-for-height, BMI | Undernutrition, obesity, drug dosing |
| Recumbent length | Infantometer (length board) | Birth–2 years | Length-for-age, weight-for-length | Stunting, wasting in infants |
| Standing height | Stadiometer | ≥2 years | Height-for-age | Stunting, linear growth monitoring |
| Head circumference | Non-stretchable tape | Birth–3 years | HC-for-age | Brain growth, micro/macrocephaly |
| MUAC | Colour-coded MUAC tape | 6–59 months | Direct classification | SAM/MAM screening in community |
| Skin-fold thickness | Harpenden calipers | Research / specialist | Body fat % | Nutritional research, obesity |
| BMI | Calculated | ≥2 years | BMI-for-age | Overweight, obesity in school-age |
SELF-CHECK
A 14-month-old child is brought for growth assessment. Which instrument is used to measure her length?
A. Stadiometer (standing height board)
B. Infantometer (recumbent length board)
C. MUAC tape
D. Skin-fold caliper
Reveal Answer
Answer: B. Infantometer (recumbent length board)
Recumbent length using an infantometer is used for children under 2 years who cannot stand reliably. A stadiometer measures standing height and is used from 2 years onward. MUAC tape screens for acute malnutrition in 6–59 month olds. Skin-fold calipers assess body fat and are not used for length.