Page 2 of 15
PE1.1 | Growth Terminology and Determinants — SDL Guide (Part 2)
Determinants of Growth: Genetic and Hormonal Factors
Growth is the product of an interaction between the child's genetic blueprint and the environment in which that blueprint is expressed. The major determinants can be grouped into two broad categories: intrinsic (genetic and hormonal) and extrinsic (environmental). Understanding each category is essential for diagnosing growth disorders, because the clinical approach differs depending on whether the aetiology is constitutional, endocrine, nutritional, or psychosocial.
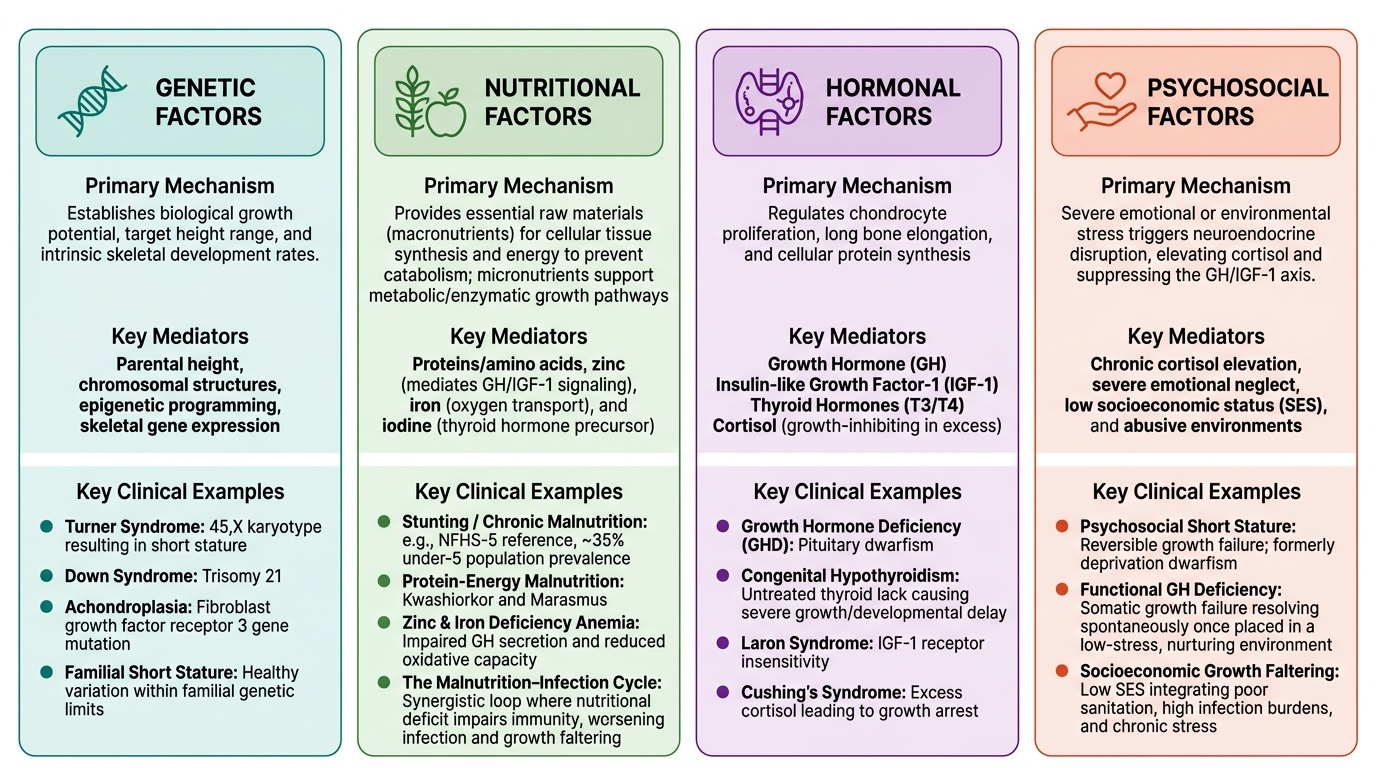
Genetic determinants set the upper limit of growth potential. A child inherits polygenic influences from both parents that determine target height, body proportions, and the tempo of growth (constitutional early or late maturers). Familial stature is the single strongest predictor of a child's eventual height: children of tall parents tend to be taller, and children of short parents shorter, independent of nutrition, provided environmental conditions are adequate. Constitutional growth delay—a normal variant in which growth tempo is slower than average—often shows a family history of late puberty and catch-up to normal adult height.
Hormonal determinants are the principal postnatal regulators of growth velocity:
- Growth hormone (GH) and IGF-1: GH from the anterior pituitary is the dominant driver of postnatal growth; it stimulates hepatic IGF-1 production, which acts directly on growth-plate chondrocytes to stimulate linear growth. GH deficiency causes proportionate short stature with normal body proportions and delayed bone age.
- Thyroid hormone (thyroxine, T4): essential for normal GH secretion and for GH receptor expression at the growth plate. Congenital hypothyroidism, if untreated, causes profound growth failure and irreversible intellectual disability—the rationale for newborn thyroid screening.
- Insulin: the principal anabolic hormone of fetal growth (explains macrosomia in infants of diabetic mothers); less dominant postnatally but still important for protein synthesis and tissue deposition.
- Sex steroids (oestrogen and testosterone): responsible for the pubertal growth spurt; oestrogen, even in boys (converted from testosterone peripherally), is essential for growth-plate closure.
- Glucocorticoids: catabolic at supraphysiological levels; chronic exogenous steroid use is a common iatrogenic cause of growth failure in children with asthma or inflammatory conditions.
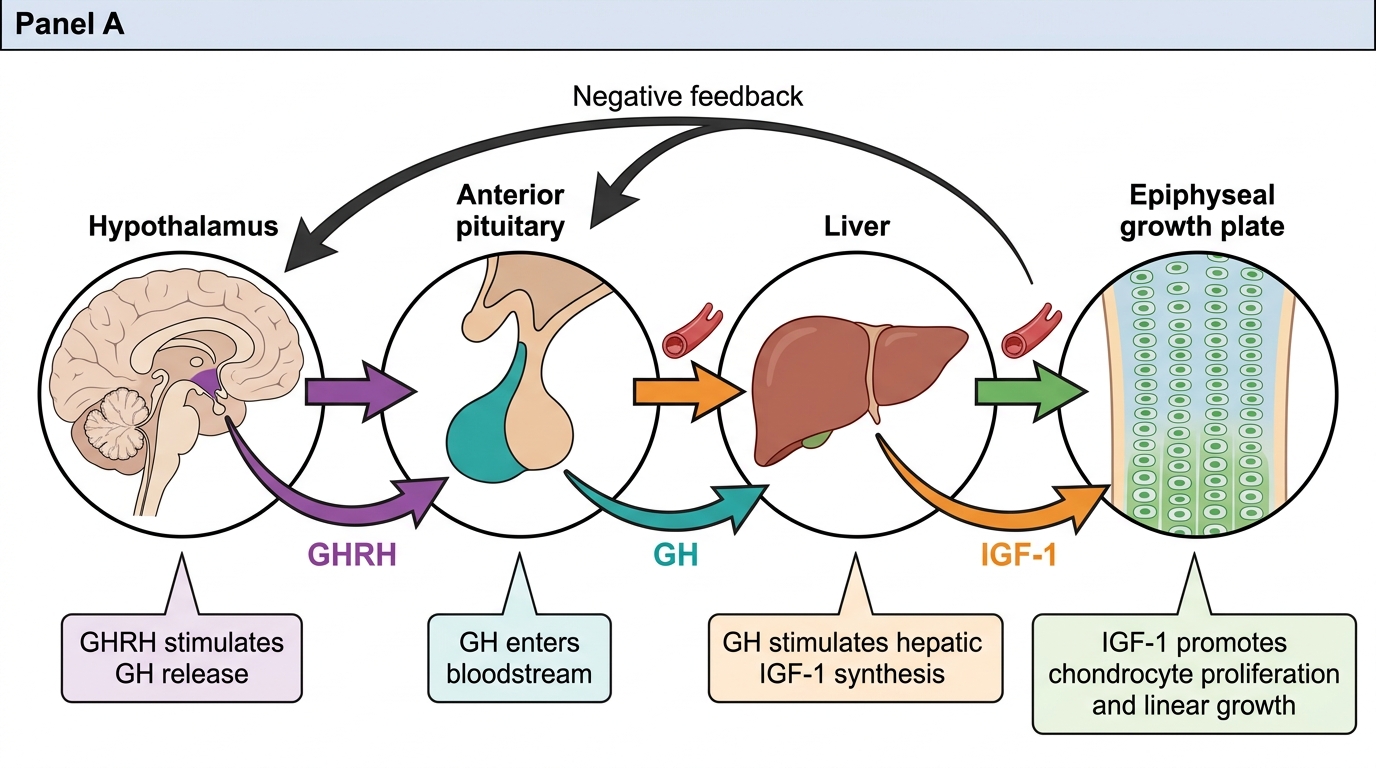
Growth Hormone Axis and IGF-1 Feedback
Determinants of Growth: Environmental and Nutritional Factors
Genetic and hormonal potential can only be realised if the child's environment provides adequate raw materials and freedom from chronic stressors. The environmental determinants of growth are particularly important in the Indian context, where suboptimal nutrition, frequent infections, and socioeconomic disadvantage continue to exert a measurable negative impact on child growth at the population level.
Provided image
Nutritional determinants are the most important environmental factor for growth globally. Protein and energy are the primary macronutrient requirements: adequate protein provides amino acids for tissue synthesis; adequate energy allows protein to be used for growth rather than catabolism. Micronutrient deficiencies exert specific, sometimes outsized effects: zinc deficiency directly impairs GH secretion and IGF-1 receptor signalling; iron deficiency causes anaemia and reduces oxidative capacity needed for growth; iodine deficiency causes hypothyroidism, compromising both GH action and neurodevelopment. In India, the National Family Health Survey (NFHS-5) documents that approximately 35% of children under 5 remain stunted—underscoring the scale of nutritional impact on growth at the population level.
Illness and infection: acute infections transiently suppress growth through cytokine-mediated reduction in appetite, increased catabolism, and reduced IGF-1 sensitivity. Chronic recurrent infections (e.g. repeated diarrhoeal episodes, parasitic infestations, tuberculosis) cause sustained growth faltering. The 'infection–malnutrition cycle' is an important concept: malnutrition impairs immunity, which increases infection susceptibility, which worsens malnutrition.
Psychosocial factors: children raised in environments of neglect, abuse, or severe psychological deprivation can develop 'psychosocial short stature' (formerly 'deprivation dwarfism')—reversible growth failure associated with functional GH deficiency that resolves when the child is placed in a nurturing environment. This is mechanistically mediated through cortisol-mediated GH suppression.
Socioeconomic status (SES) integrates multiple growth determinants: higher SES correlates with better nutrition, healthcare access, lower infection burden, and superior psychosocial environment. The secular trend in height (gradual increase in mean adult height over generations) is predominantly a reflection of improving SES and nutrition rather than genetic change.
Geographic and seasonal variation: altitude (chronic hypoxia) slightly retards growth; seasonal food availability affects growth velocity in agricultural communities (children in India often gain more weight during and after the harvest season).
SELF-CHECK
Which of the following is the MOST important determinant of postnatal linear growth?
A. Insulin
B. Growth hormone and IGF-1
C. Oestrogen
D. Cortisol
Reveal Answer
Answer: B. Growth hormone and IGF-1
Growth hormone (GH) from the anterior pituitary, acting via insulin-like growth factor-1 (IGF-1), is the dominant driver of postnatal linear growth. Insulin is the primary anabolic hormone of fetal (intrauterine) growth. Oestrogen drives the pubertal growth spurt and eventually closes the growth plate. Cortisol at supraphysiological levels is catabolic and inhibits growth.
CLINICAL PEARL
Catch-up growth is not automatic—it requires two conditions to occur together: (1) removal of the growth-limiting factor (e.g. treating hypothyroidism, rehabilitating nutrition), AND (2) adequate ongoing nutritional support to sustain the accelerated anabolic demand. A child with hypothyroidism started on thyroxine will not catch up in height unless protein and energy intake are simultaneously adequate. Clinicians who correct the hormonal deficiency without addressing nutrition may be puzzled by the incomplete catch-up—this is a common clinical trap. Similarly, catch-up growth has a critical window: the younger the child when the limiting factor is removed, the more complete the catch-up, because growth plate cartilage retains more proliferative capacity.
Clinical Applications: Catch-up Growth, Growth Failure, and Paediatric Surveillance
The clinical significance of understanding growth terminology and determinants lies in its direct application to three practical tasks: identifying growth failure, explaining catch-up growth to parents, and organising population-level surveillance.
Growth failure (growth faltering) is defined as a sustained downward crossing of two or more major percentile lines on a growth chart, or as weight-for-age, height-for-age, or weight-for-height below –2 SD (3rd percentile) on standardised growth charts. Growth failure is not a diagnosis—it is a clinical sign that requires systematic evaluation of the determinants: nutritional adequacy, chronic illness screen (renal, hepatic, haematological, endocrine), psychosocial history, and family history of stature and growth tempo.
Catch-up growth is clinically important as a therapeutic endpoint: when a child with nutritional rehabilitation or treated hypothyroidism shows a velocity that is faster than expected for age (crossing upward on the growth chart), the clinician is observing biological confirmation that the treatment is working. The maximum extent of catch-up is inversely related to the severity and duration of the growth-limiting insult: a 6-month episode of moderate undernutrition in a 2-year-old is more completely reversible than a chronic 3-year insult starting in infancy.
Paediatric growth surveillance in India is structured around the Under-5 child health programme: the child health card (growth card) documents weight at each contact (birth, 6 weeks, 10 weeks, 14 weeks, 9 months, 12 months, 15 months, 18 months, 24 months, and annually up to 5 years). The ICDS system uses Anganwadi workers to plot weight monthly for children 0–3 years. These surveillance touchpoints are opportunities to identify growth faltering before it becomes severe acute malnutrition (SAM), defined by MUAC <11.5 cm, weight-for-height <–3 SD, or bilateral pedal oedema.
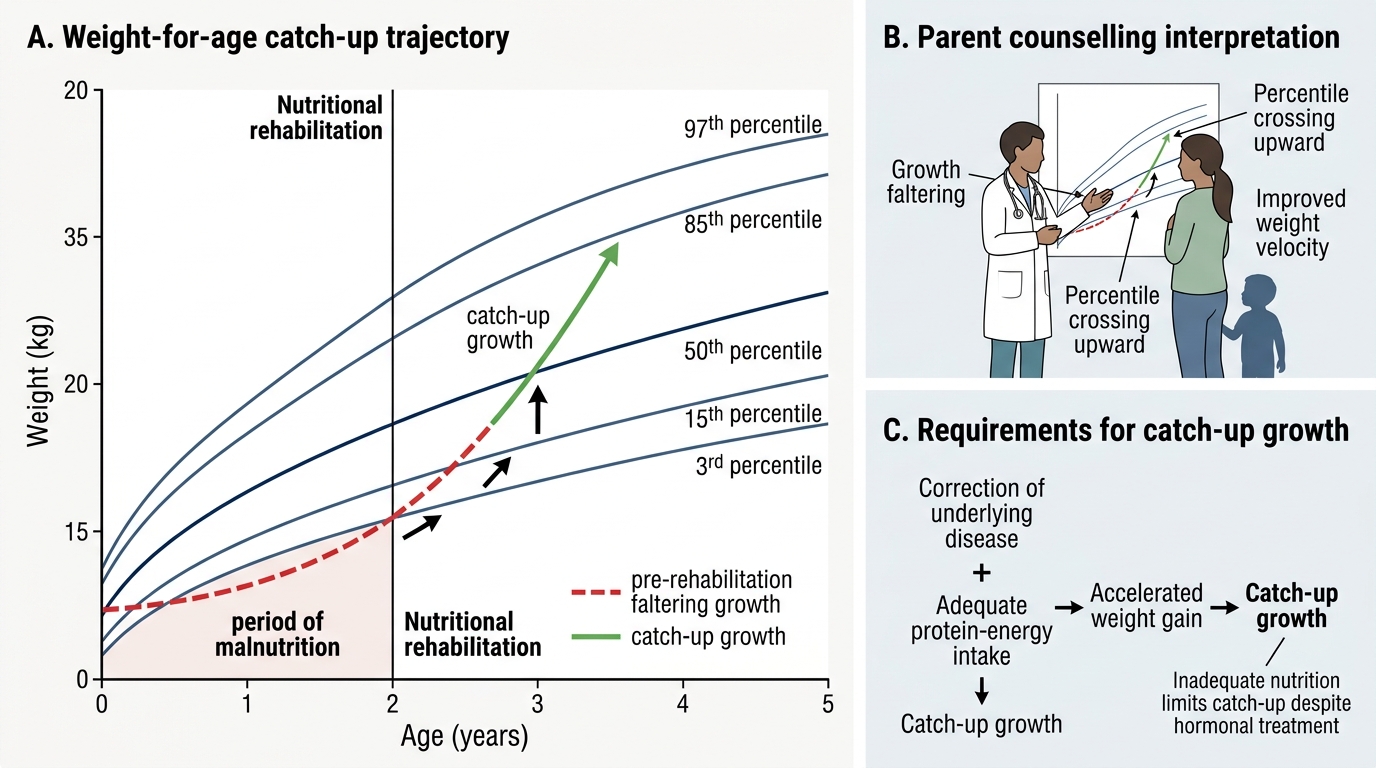
Catch-up Growth After Nutritional Rehabilitation
For the final-year MBBS student, competency in this domain means being able to interpret a growth chart, counsel a parent about the significance of a growth concern, and initiate a logical diagnostic workup when growth failure is suspected—skills all built on the foundation of the terminology and determinants covered in this module.
SELF-CHECK
A 3-year-old boy who was recovering from untreated hypothyroidism is now on thyroxine replacement for 6 months but shows only modest height catch-up. The most likely additional factor limiting catch-up growth is:
A. Inadequate thyroxine dose
B. Insufficient nutritional intake
C. Persistent growth hormone deficiency
D. Chromosomal abnormality
Reveal Answer
Answer: B. Insufficient nutritional intake
Catch-up growth requires both hormonal correction AND adequate nutritional support. Thyroxine replacement alone is insufficient if protein and energy intake remain suboptimal — the accelerated anabolic demand of catch-up growth cannot be met without nutritional substrates. Inadequate thyroxine dose is possible but the question specifies 6 months on replacement with modest (not absent) catch-up, pointing to a nutritional co-determinant. GH deficiency as a co-morbidity is less common; chromosomal abnormality would usually be part of the initial evaluation.
Self-Assessment: Growth Terminology and Determinants
Use these questions to consolidate your understanding before moving to the next module on growth assessment and anthropometry.
Question 1: A mother says her 10-month-old daughter 'seems to be growing slowly.' Her weight was 7.5 kg at 9 months and is 7.7 kg at 10 months. Is this a concern? Apply your knowledge of normal growth velocity.
(Expected answer: Weight gain of approximately 200 g/month is within the normal range for 9–12 months [normal ~200 g/month], so this is NOT alarming. However, you would want to plot the weight on a growth chart and look at the trend from birth—a single month's velocity alone is insufficient for decision-making.)
Question 2: List three intrinsic (genetic/hormonal) and three extrinsic (environmental) determinants of growth and give one clinical example of how each can cause growth failure.
(Sample intrinsic: GH deficiency → isolated proportionate short stature; congenital hypothyroidism → proportionate short stature + developmental delay; Turner syndrome → short stature in females. Sample extrinsic: protein-energy malnutrition → stunting; recurrent intestinal parasitosis → growth faltering; psychosocial deprivation → functional GH deficiency.)
Question 3: Distinguish 'distance' growth from 'velocity' growth and explain why velocity is more sensitive for early detection of growth faltering.
(Distance = attained size at a single time point; velocity = rate of change over an interval. A child who is constitutionally small may have a weight consistently below the 3rd percentile but grow at normal velocity — velocity reveals that the child is tracking their centile, reassuring the clinician. Conversely, a child who was previously at the 50th percentile but is now tracking toward the 25th—detected only by velocity—signals a new problem that distance alone at either time point might not flag.)