Page 2 of 26
PE18.1-2 | UIP Framework and Vaccine Preventable Disease Epidemiology — SDL Guide (Part 2)
Mechanisms Behind Programme Effectiveness: Herd Immunity and Cold Chain
The programmatic rationale for achieving high vaccination coverage is grounded in two interacting mechanisms: herd immunity (the population-level indirect protection that emerges when enough individuals are immune) and cold chain integrity (the infrastructure that ensures vaccines remain potent from manufacture to administration).
Provided image
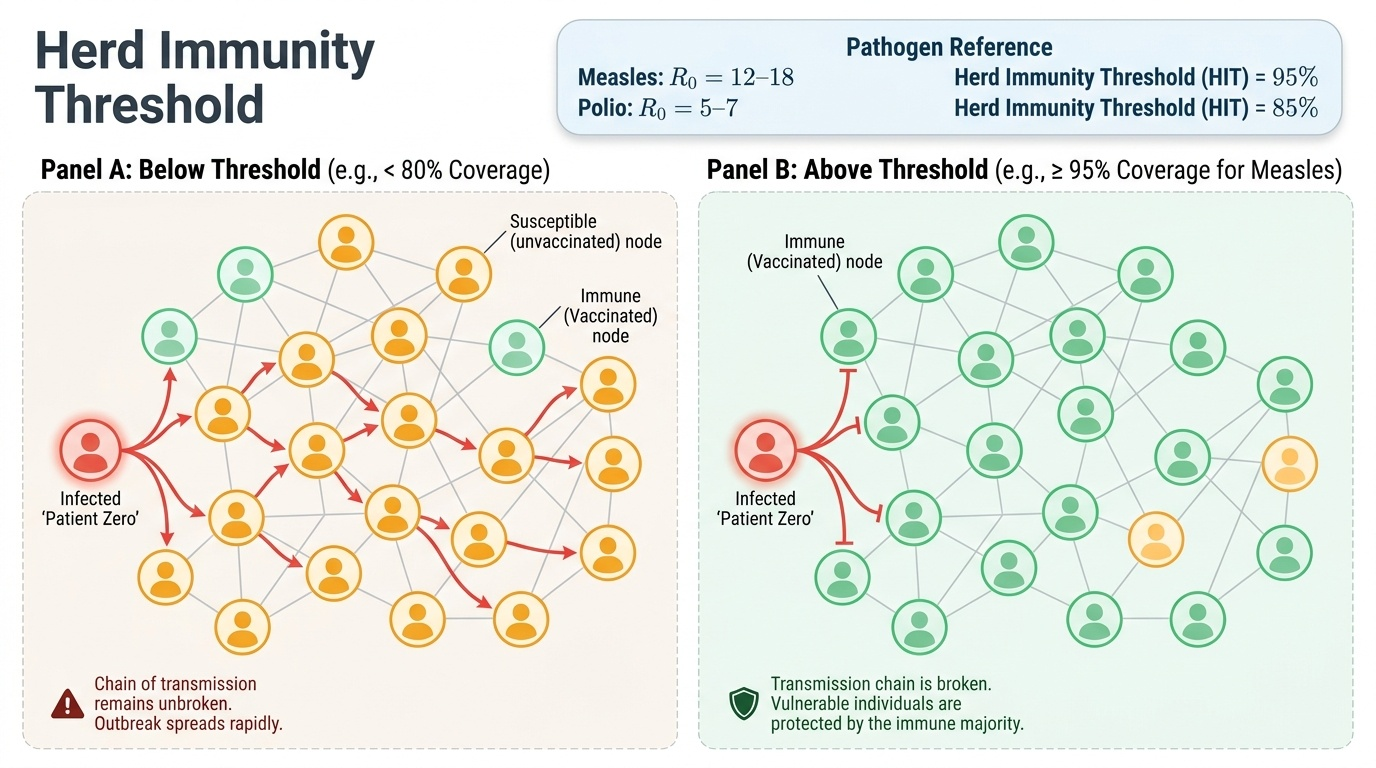
Herd immunity and the threshold concept: When an immunised individual cannot be infected, they cannot transmit the pathogen to others — breaking the chain of transmission. The proportion of the population that must be immune to prevent sustained transmission is the herd immunity threshold (HIT), and it is directly determined by the pathogen's R0 (basic reproduction number): HIT = 1 − (1/R0). Because measles has one of the highest known R0 values (12–18), its HIT is 92–95% — meaning that if even 5–8% of the community is susceptible, measles can spread. This explains why a single unvaccinated cluster in an otherwise high-coverage population can ignite a measles outbreak, as illustrated in the hook scenario. Poliovirus has a lower R0 (5–7), yielding an HIT of ~80–85%, which is why polio was achievable before measles elimination.
The implication is that coverage must be uniformly high — district-level or village-level pockets of low coverage create geographically concentrated susceptibles, enabling cluster outbreaks even when national FIC appears adequate.
Cold chain: Vaccines are biological products that are irreversibly degraded by heat, freeze-thaw cycles, and light. The cold chain is the unbroken series of refrigerated storage and transport steps that maintains the vaccines' required temperature from manufacturer to the administered dose:
- Ice-Lined Refrigerators (ILR): 2–8°C — most vaccines (BCG, MR, DPT, Hep-B, pentavalent, fIPV)
- Deep Freezers: −15 to −25°C — OPV must be stored frozen (the only NIS vaccine requiring deep freeze); rotavirus can be stored at 2–8°C
- Vaccine carrier with ice packs: for field outreach sessions (2–8°C); the ANM loads vaccines just before leaving for the outreach site
- Vaccine Vial Monitor (VVM): a heat-sensitive label on each vial that darkens irreversibly when cumulative heat exposure exceeds a threshold, signalling that vaccine potency may be compromised. Reading the VVM is mandatory before administration — a darkened inner square means DO NOT USE.
One critical error pattern that destroys vaccines is freeze damage: freeze-sensitive vaccines (DPT, Hep-B, pentavalent, fIPV) are permanently damaged if accidentally frozen, yet they show no visible change. The shake test distinguishes freeze-damaged adsorbed vaccines from intact ones — freeze-damaged vaccines form a compact sediment that does not re-suspend.
Coverage determinants: The WHO identifies three categories of determinants for immunisation coverage gaps: (1) Supply-side barriers — cold chain failures, vaccine stock-outs, insufficient outreach sessions, inadequate ANM staffing; (2) Demand-side barriers — vaccine hesitancy, misinformation, religious objections, lack of awareness, prior bad experience (AEFI); (3) Access barriers — geographic remoteness, migration, seasonal floods, urban slum dynamics, displaced and tribal populations. The RED (Reaching Every District) strategy operationalises systematic identification and re-engagement of under-served populations to close coverage gaps.
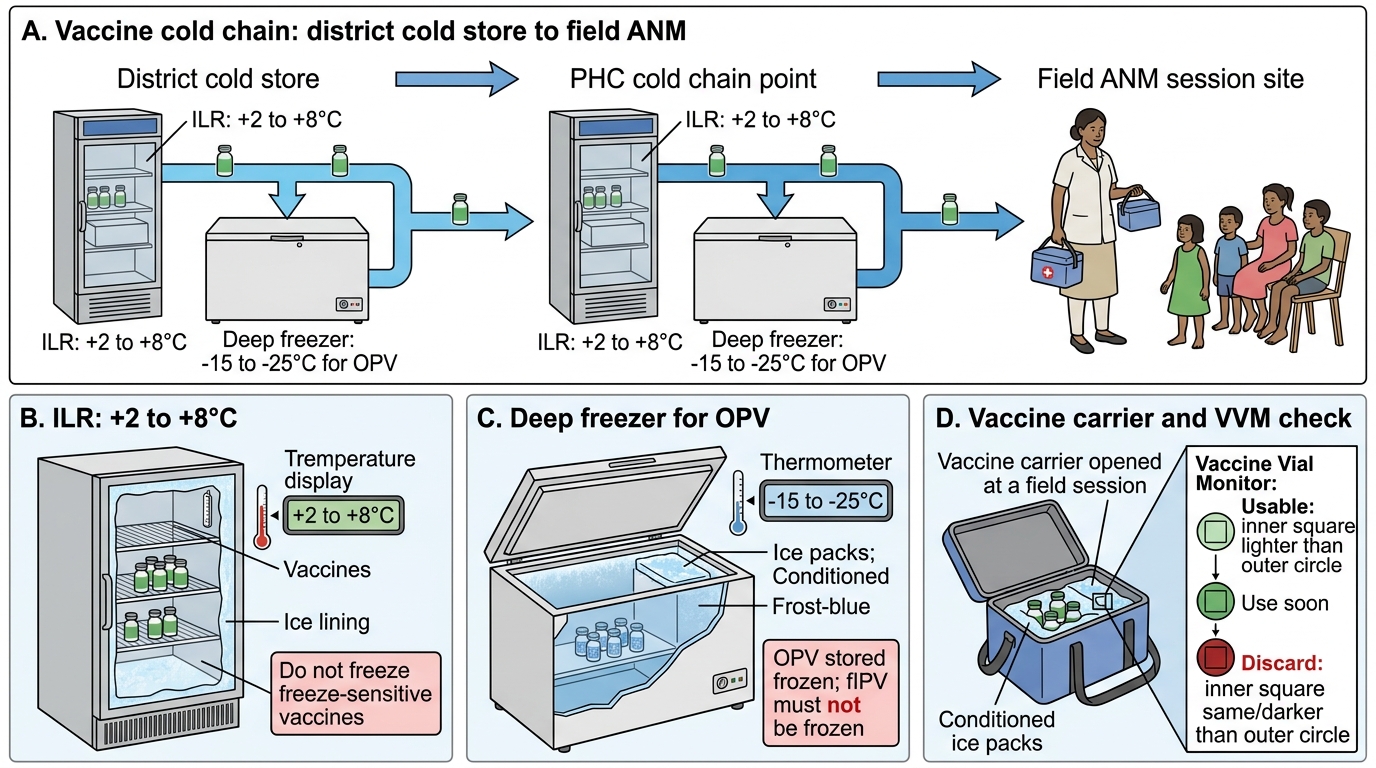
Vaccine Cold Chain Equipment and Field Flow
SELF-CHECK
A village reports a measles outbreak despite a stated district-level vaccination coverage of 87%. Which concept BEST explains why an outbreak is still occurring at this coverage level?
A. Measles vaccine has an unusually low efficacy
B. The herd immunity threshold for measles (~92-95%) has not been reached, leaving susceptible clusters
C. The cold chain was adequate so the outbreak must be a different infection
D. OPV rather than MR vaccine was given to these children
Reveal Answer
Answer: B. The herd immunity threshold for measles (~92-95%) has not been reached, leaving susceptible clusters
Measles R0 of 12–18 requires 92–95% population immunity for herd protection. At 87% coverage, approximately 13% of children remain susceptible. If these susceptible individuals are geographically clustered (as in a village with low uptake), the local transmission rate exceeds 1 even when district-wide average is below the threshold — producing local outbreaks despite apparently adequate overall coverage. This is the core epidemiological argument for achieving uniformly high sub-district coverage, not just aggregate statistics.
CLINICAL PEARL
OPV must be stored frozen — but fIPV must NOT be frozen. This is the single most common cold-chain error at field level: a zealous cold-chain handler stores ALL injectables in the deep freezer, irreversibly damaging the fIPV (an adsorbed inactivated vaccine). The NIS now uses both OPV (oral, −20°C) and fIPV (intradermal, 2–8°C) in the same session at 6 and 14 weeks. When checking vaccine orders and cold chain at an outreach session, confirm OPV vials come from the deep freezer and fIPV from the ILR. Use the VVM (inner square lighter than outer ring = use; inner square same or darker = do not use) and always perform the shake test for suspected freeze-damaged adsorbed vaccines.
Programme Impact, Surveillance, Eradication and AEFI Management
India's Universal Immunization Program has produced measurable, historically significant reductions in vaccine preventable disease burden — and in one landmark case, the complete eradication of wild poliovirus transmission. The programme's impact extends across multiple VPDs, achieved through decades of sustained political commitment, a nationwide cold chain infrastructure, and the mobilisation of frontline health workers at sub-centre level. These achievements are not merely historical — they demonstrate what is possible when a programmatic immunisation system achieves and sustains coverage above herd immunity thresholds, and they set the benchmark for India's ongoing targets of measles elimination and further VPD reduction. Understanding these outcomes is essential for every clinician, as it grounds the counselling conversation with families in real evidence of benefit.
Provided image
Programme impact and milestones:
- Polio eradication: The last case of wild poliovirus in India was reported on 13 January 2011 (a child in West Bengal with WPV1). India was certified polio-free by WHO in April 2014, after the required 3-year surveillance period without a wild poliovirus case. This was achieved through a combination of routine immunisation, National Immunisation Days (NIDs) with house-to-house OPV delivery, and acute flaccid paralysis (AFP) surveillance. India's success was remarkable given its population density, sanitation challenges, and the persistence of poliovirus in the environment.
- Measles: India is working toward measles elimination (defined as <1 case/million/year with no endemic transmission). The MR vaccination campaign (2017–2019) covered 324 million children aged 9 months to <15 years, substantially raising population immunity. Measles deaths have declined by over 90% compared to pre-vaccine era estimates.
- Neonatal tetanus: India achieved elimination status (defined as <1 case/1,000 live births/district) nationally in 2015, primarily through TT/Td immunisation of pregnant women and clean delivery practices.
- Mission Indradhanush outcomes: IMI 1–4 and Intensified MI reached an estimated 38 million children with one or more vaccines, significantly increasing full immunisation coverage in high-priority districts.
Surveillance systems for VPDs:
- Acute Flaccid Paralysis (AFP) surveillance: All children <15 years with AFP (sudden onset of flaccid weakness) are reported and investigated for poliomyelitis. This is the global standard for poliovirus surveillance, with a performance indicator of ≥2 AFP cases/100,000 children <15 years per year.
- Integrated Disease Surveillance Programme (IDSP): Weekly and outbreak-alert surveillance for VPDs including measles, diphtheria, and pertussis.
- AEFI (Adverse Event Following Immunization) surveillance: See below.
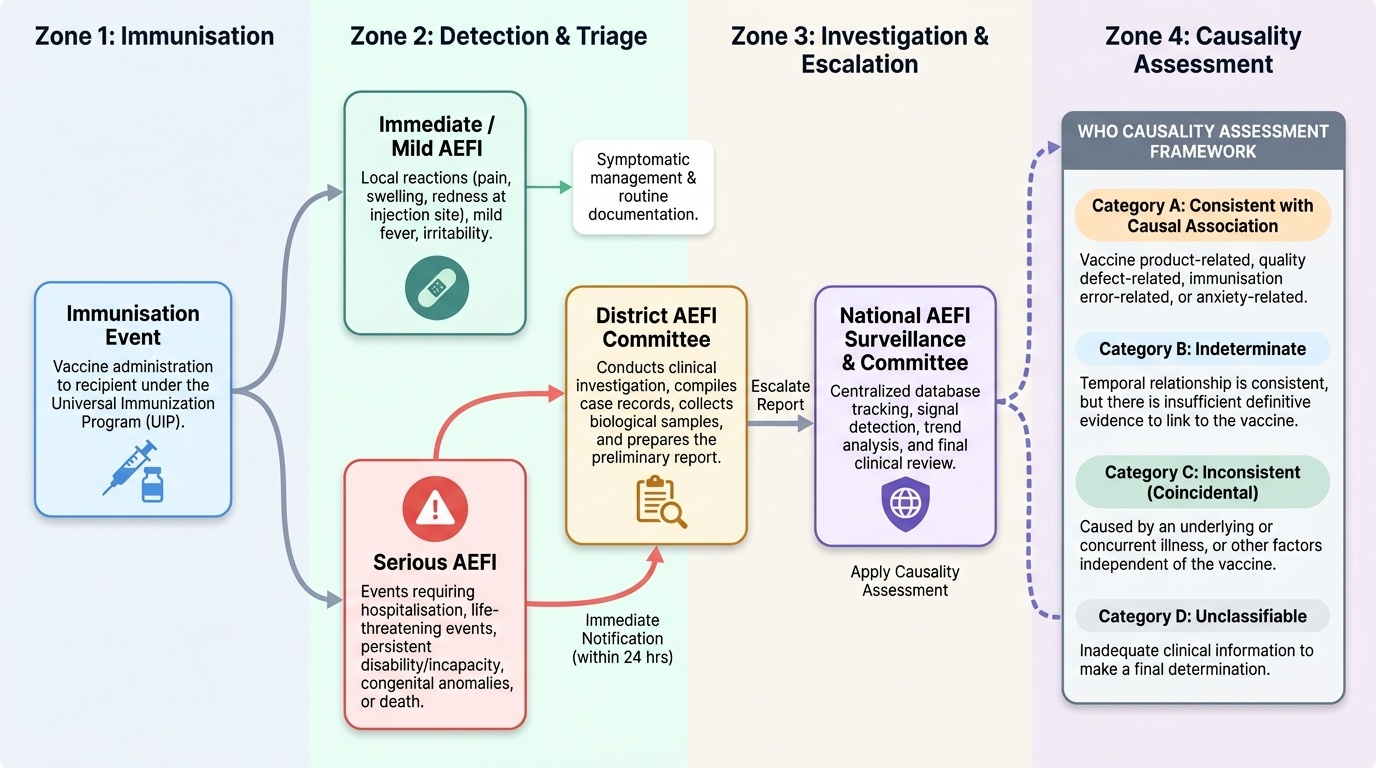
AEFI — classification and management:
Adverse Events Following Immunization are any untoward medical occurrence temporally associated with vaccination. The WHO-CIOMS framework classifies AEFIs as:
1. Vaccine-induced reactions (vaccine-product-related): e.g., OPV-associated paralytic poliomyelitis (VAPP — 1:750,000 first doses OPV), BCG abscess, febrile seizure with DPT.
2. Vaccine-quality defects (vaccine-quality-related): from manufacturing or storage errors.
3. Immunization error-related reactions: incorrect dose, wrong site, contaminated vial.
4. Immunization anxiety-related reactions: fainting, vasovagal — independent of vaccine.
5. Coincidental events: would have occurred regardless.
Severity classification for reporting purposes:
- Serious AEFI: causes hospitalisation, significant disability, life-threatening illness, death, or a congenital anomaly. Mandatory reporting within 24 hours to district AEFI committee.
- Non-serious (mild) AEFI: local reactions (pain, swelling, erythema at injection site within 48 h), low-grade fever, irritability — managed symptomatically; counsel families that these are expected and transient.
The district AEFI committee investigates serious events, classifies causality (using the WHO causality assessment algorithm), and reports upward to the state and national AEFI surveillance cell. This reporting chain protects programme credibility — timely transparent response to AEFIs prevents vaccine hesitancy escalation.
Counselling families on AEFI: A critical clinical skill is anticipatory guidance — informing parents before vaccination what to expect (mild local reactions, low-grade fever within 24–48 h with DPT), what to monitor (any rash, high fever, difficulty breathing, unusual crying — report immediately), and the risk-benefit framing: the risk from the VPD is many orders of magnitude higher than any serious AEFI risk.
Self-Assessment: Consolidating UIP and VPD Epidemiology
Now that you have worked through the epidemiology of vaccine preventable diseases, the structure of India's Universal Immunization Program, the mechanisms of herd immunity and cold chain, and the programme's impact and surveillance systems, it is time to consolidate your understanding through active recall and self-testing. The competencies PE18.1 and PE18.2 require you to be able to explain — not merely list — the components of the UIP/NIP and the epidemiology of the targeted VPDs. This means you should be able to justify why each vaccine is given at its specific age-point (connecting VPD biology to schedule timing), apply the herd immunity threshold concept to real coverage scenarios, and counsel a family about AEFI with accurate risk-benefit framing. Use the micro-quizzes and reflection questions in this module to identify any gaps, then return to the relevant sections to reinforce those areas before your examinations and clinical postings.
SELF-CHECK
A 6-week-old infant develops fever of 38.5°C and local redness at the injection site 24 hours after receiving pentavalent and OPV at the PHC. The mother is alarmed. What is the MOST appropriate response?
A. Admit the child immediately for observation and investigation for AEFI
B. Advise no more vaccination as the child has had an adverse reaction
C. Reassure the mother that mild local reactions and low-grade fever are expected with DPT-containing vaccines and are self-limiting; return if high fever, rash, or unusual crying
D. Report this as a serious AEFI to the district committee within 24 hours
Reveal Answer
Answer: C. Reassure the mother that mild local reactions and low-grade fever are expected with DPT-containing vaccines and are self-limiting; return if high fever, rash, or unusual crying
Low-grade fever and local redness within 24–48 hours of DPT-containing (pentavalent) vaccination are classified as mild non-serious AEFIs — they are vaccine-product-related expected reactions, not a reason to withhold future doses. Serious AEFIs (hospitalisation, disability, anaphylaxis, death) require 24-hour reporting to the district committee. The correct clinical response here is anticipatory guidance: validate the mother's concern, confirm this is expected and self-limiting, advise paracetamol for fever if above 38.5°C, and provide specific return-to-care criteria.