Page 5 of 26
PE18.{3,6,14} | Vaccine Classification and Schedules — SDL Guide (Part 2)
Prescribing an Age-Appropriate Immunization Schedule
Prescribing an age-appropriate immunization schedule requires first assessing the child's fitness for vaccination (minor illness is NOT a contraindication; see below), then determining which vaccines are due at the current age, which have been missed, and whether any special clinical considerations apply. This clinical process — assess, determine, prescribe — is the practical application of schedule knowledge. Across all steps, the guiding principle is to maximise protection at every contact: a child presenting for any reason — a cough, a rash, a growth check — is an opportunity to administer due vaccines, and that opportunity must never be wasted by applying false contraindications or administrative delays.
Step 1 — Assess fitness for immunization:
Ask about the current health status. Minor illnesses (mild fever, upper respiratory tract infection, mild diarrhoea) are NOT contraindications to immunization — a common and harmful misconception that leads to missed opportunities. A child with a mild cold can and should receive scheduled vaccines. The following are TRUE contraindications:
• Anaphylaxis to a previous dose of the same vaccine or its components (e.g., egg allergy for some influenza vaccines — though most current influenza vaccines can be given with precaution).
• Live vaccines contraindicated in: primary immunodeficiency, HIV with CD4 <15% (or <200 cells/µL in older children), active malignancy on chemotherapy, high-dose corticosteroids (≥2 mg/kg/day for ≥2 weeks), organ transplant recipients on immunosuppression, and pregnancy (relevant for adolescent females).
• BCG: do NOT give if child has symptomatic HIV (CD4-based assessment needed per IAP guidelines).
• Pertussis component of DPT: avoid further doses if the child had encephalopathy within 7 days of a previous DPT dose.
False contraindications (do NOT withhold vaccine for these): mild fever, mild diarrhoea, mild skin infection, allergy to penicillin, stable neurological disease, family history of adverse reactions, prematurity (give as per chronological age), low birth weight ≥2 kg (for BCG), breastfeeding.
Step 2 — Determine due vaccines:
Match the child's actual chronological age to the NIS schedule. For a child with a gap, identify the last vaccine received and the current age, then apply the catch-up principle: continue the series, ensuring minimum intervals are respected. Do not restart a series. Minimum interval between doses in a primary series is generally 4 weeks for most vaccines.
Step 3 — Prescribe and document:
Write the vaccine name, dose, route, and site in the immunization card. Always administer vaccines at the correct site and route — intramuscular injections (pentavalent, HepB) go into the anterolateral thigh in infants under 12 months (not the deltoid, which lacks sufficient muscle mass); the deltoid becomes appropriate at 12 months or older. Intradermal injections (BCG, fIPV) require proper technique — a bleb must form.
If multiple vaccines are due simultaneously, they may be given at different sites on the same visit (recommended and evidence-based). Do NOT withhold a vaccine because another vaccine is being given concurrently.
SELF-CHECK
A 9-month-old child comes to the OPD with mild fever (temperature 37.9°C) and mild rhinorrhoea for 2 days. She is due for her MR vaccine. What is the correct action?
A. Postpone MR vaccine until she is completely well
B. Administer MR vaccine today as minor illness is not a contraindication
C. Administer only paracetamol and reschedule vaccine after 2 weeks
D. Check MR antibody titres before deciding
Reveal Answer
Answer: B. Administer MR vaccine today as minor illness is not a contraindication
Minor illness (mild fever, mild URTI, mild diarrhoea) is NOT a contraindication to immunization. Postponing vaccines for minor illness is a common false contraindication that creates missed opportunities and leaves children unprotected. The MR vaccine should be administered today. Checking antibody titres before vaccination is not routine practice and is not indicated here.
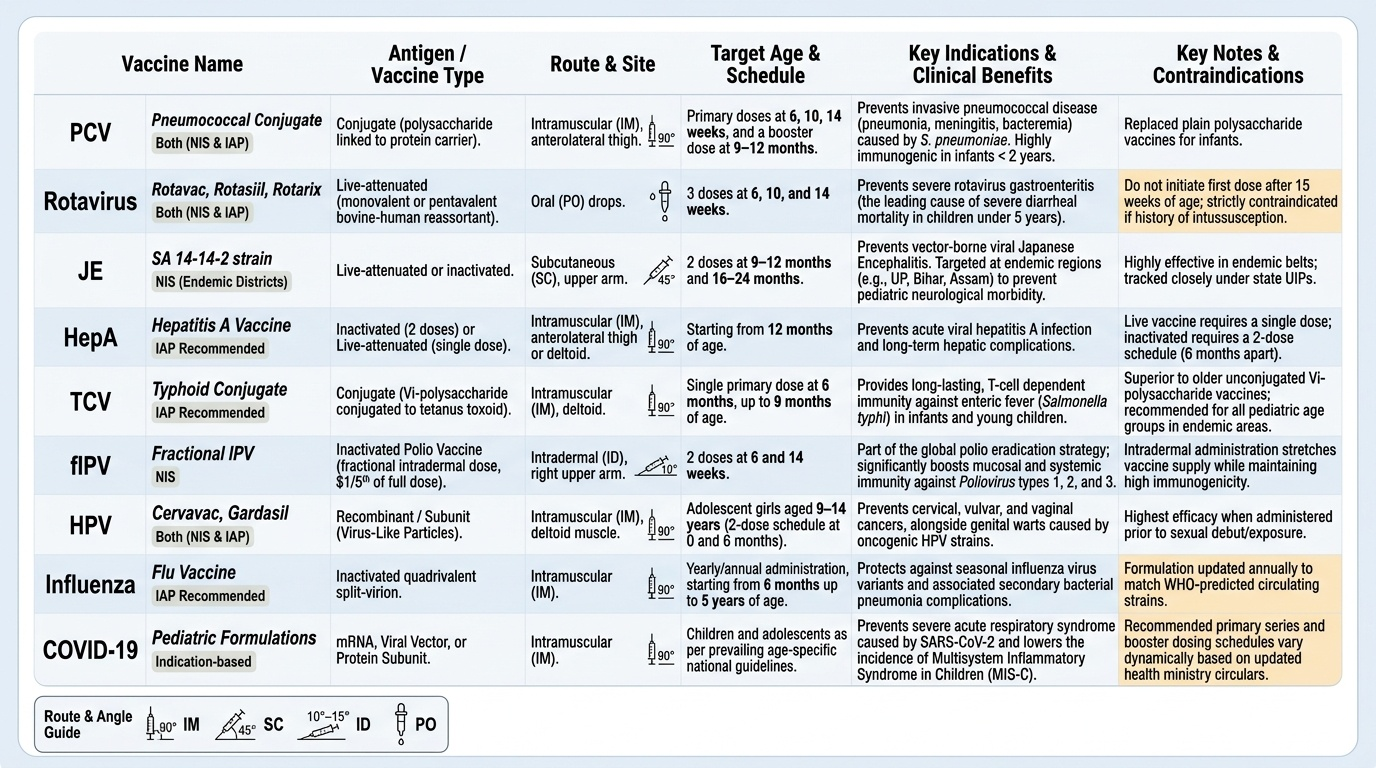
Newer Vaccines and Their Indications
The NIS and IAP schedule have progressively incorporated newer vaccines as evidence of safety, efficacy, and programme feasibility accumulates. Understanding these additions — their antigen type, target age, and specific indications — is now part of the NIS knowledge requirement at final-year level.
Provided image
Pentavalent vaccine combines DPT (diphtheria, pertussis, tetanus toxoids + acellular or whole-cell pertussis) with Hepatitis B (recombinant HBsAg) and Hib (Haemophilus influenzae type b conjugate) in a single injection. Introduced into the NIS nationally by 2011–2012, it replaced the separate DPT and HepB doses at 6/10/14 weeks, reducing injection burden. It prevents 5 diseases with 3 injections.
Pneumococcal conjugate vaccine (PCV) — PCV10 or PCV13 targets the most common serotypes of Streptococcus pneumoniae causing meningitis, pneumonia, and bacteraemia in children. PCV has been introduced in select Indian states under the UIP and is on the IAP recommended schedule. Administered at 6, 10, 14 weeks (primary) with a booster at 9–12 months (or per schedule). It is a conjugate vaccine (polysaccharide linked to protein carrier) — immunogenic in infants under 2 years unlike plain polysaccharide vaccines.
Rotavirus vaccine — India has two indigenous vaccines: Rotavac (Bharat Biotech, monovalent G9P[11] bovine-human reassortant) and Rotasiil (Serum Institute, pentavalent bovine-human reassortant), alongside Rotarix (GlaxoSmithKline, monovalent G1P[8] human). Oral, live-attenuated. Given at 6, 10, 14 weeks under NIS. Prevents severe rotavirus gastroenteritis — the commonest cause of severe diarrhoeal death in under-5 children. Contraindicated: intussusception history; do NOT initiate after 15 weeks of age (risk of intussusception).
Japanese Encephalitis (JE) vaccine — live attenuated SA 14-14-2 strain (indigenous, SA 14-14-2 manufactured in India). Two doses at 9–12 months and 16–24 months in endemic districts. JE is a vector-borne viral encephalitis endemic in Uttar Pradesh, Bihar, Assam, and other states; it causes severe neurological morbidity and mortality in children.
Hepatitis A vaccine — inactivated, 2 doses. IAP recommended; not yet in UIP/NIS nationally. Indicated for all children as HAV is endemic in India; especially important for children in areas with unsafe water and sanitation. Prevents acute hepatitis A and fulminant hepatic failure.
Typhoid Conjugate Vaccine (TCV) — Vi polysaccharide conjugated to tetanus toxoid. Single dose from 6 months onwards; NIS introduced TCV from 2022 in select states. Advantages over plain Vi polysaccharide: immunogenic in infants, generates T-cell-dependent immunity, likely longer duration. Typhoid fever remains highly endemic in India.
Fractional IPV (fIPV) — one-fifth the standard IPV dose delivered intradermally (0.1 mL ID). Introduced into NIS at 6 and 14 weeks to replace the type-2 component after global monovalent OPV-2 withdrawal (2016) and to conserve IPV supply. Intradermal delivery via the Mantoux technique exploits the high density of dendritic cells in the dermis, achieving comparable seroconversion to full-dose IPV.
HPV vaccine (Human Papillomavirus) — recombinant VLP-based. Protects against HPV types 16 and 18 (cervical cancer–causing) and types 6 and 11 (genital warts — quadrivalent/nonavalent). IAP recommends: 2 doses for girls aged 9–14 years (if series starts before 15th birthday); 3 doses (0, 1–2, 6 months) for those aged 15 years and above or immunocompromised. Ideally administered before sexual debut. Catch-up vaccination up to age 26 years. India's national programme (pilot 2023) targets school-age girls.
Influenza vaccine — inactivated trivalent or quadrivalent. IAP recommended annually for high-risk children (chronic pulmonary/cardiac disease, diabetes, immunocompromised, asplenia) and their household contacts. Not currently in UIP. Requires annual revaccination due to antigenic drift.
COVID-19 vaccine — multiple platforms (mRNA, recombinant protein, inactivated whole-virus). In India, COVAXIN (inactivated whole virus, Bharat Biotech) approved for children ≥6 years; CORBEVAX (RBD protein subunit) for 5–18 years. Schedule and recommendations continue to evolve per NTAGI/MoHFW guidance.
CLINICAL PEARL
Rotavirus vaccine timing trap: The first dose of rotavirus vaccine must NOT be initiated after 15 weeks of age (IAP/WHO recommendation). Beyond 15 weeks, the intestine's susceptibility to intussusception increases if a live rotavirus vaccine is given for the first time. If a child misses the first dose window, do NOT start rotavirus vaccination — omit it entirely and document. This is a firm cut-off, not a precaution. The last dose should also be completed by 32 weeks. Similarly, fIPV is given ID (not IM) at a 0.1 mL dose — administering full-dose IPV IM instead of fIPV ID is a common pharmacy-level error that wastes vaccine supply and must be caught at prescription.
Risks, Benefits, Side Effects and Contraindications
Every vaccine carries both a benefit (protection against disease) and a risk (adverse effects following immunization, AEFI). Understanding this balance is essential both for counselling parents and for recognising and managing AEFI when they occur.
Benefits of immunization far outweigh risks for all NIS vaccines. Measles vaccination prevents an estimated 2–3 million deaths annually worldwide. The eradication of smallpox and near-elimination of polio globally demonstrate the transformative power of vaccination programmes. At the individual level, completing the NIS protects against at least 12 major pathogens causing life-threatening disease in childhood. For every serious AEFI attributed to vaccination, thousands of deaths, hospitalisations, and cases of permanent disability are prevented — the benefit-risk calculation is decisively in favour of vaccination for every NIS-recommended vaccine. This does not mean risks are ignored: informed consent requires honest discussion of expected and rare adverse effects, and every immunization site must be equipped to manage anaphylaxis, however infrequent.
Adverse Events Following Immunization (AEFI) are classified as:
• Programme errors — wrong vaccine, wrong dose, wrong route, contaminated vial (preventable)
• Vaccine-induced — related to the vaccine's inherent properties:
- Local reactions: pain, redness, swelling at injection site (most common; resolve spontaneously)
- Systemic reactions: fever (especially after DPT — pertussis component is the commonest cause of post-vaccine fever), irritability, malaise (common; last 1–2 days)
- Specific reactions: BCG lymphadenitis (suppurative or non-suppurative); BCG ulcer (expected local reaction within 2–4 weeks); post-MR fever and mild rash at 7–12 days
- Severe/rare AEFI: anaphylaxis (1 per million doses for most vaccines — have adrenaline 1:1000 at 0.01 mg/kg IM available at all immunization sites); febrile seizures (DPT, fever-related); vaccine-associated paralytic poliomyelitis (VAPP, OPV — 1 per 2.7 million doses, eliminated as OPV replaced by fIPV for type 2); intussusception (rotavirus — risk confined to first dose if given after 15 weeks)
True contraindications (absolute):
• Prior anaphylaxis to the same vaccine or its components
• Live vaccines in severe immunodeficiency (SCID, HIV with CD4 <15%)
• Encephalopathy within 7 days of prior DPT dose (contraindication to pertussis component)
• Pregnancy (live vaccines — MMR, varicella; not a consideration for NIS given peri-adolescent scheduling)
Precautions (defer, do not permanently omit):
• Moderate-to-severe acute illness with fever >39°C — defer until recovered
• Recent receipt of blood/blood products (may inhibit live vaccine response — defer MR/varicella 3–11 months depending on product)
• Thrombocytopenia (relative precaution for MR — clinical judgment)
False contraindications (do NOT withhold vaccine):
• Mild fever / mild illness / mild diarrhoea
• Family history of adverse reactions
• Allergy to penicillin or unrelated allergens
• Stable neurological conditions (e.g., well-controlled epilepsy — DPT is NOT contraindicated)
• Prematurity (vaccinate at chronological age with full doses)
• Low birth weight (BCG: give at birth if weight ≥2 kg; if <2 kg, give at discharge when weight ≥2 kg or at 6 weeks)
• Breastfeeding
• Concurrent mild illness or minor surgery
• Previous history of measles, mumps, or rubella (still vaccinate)
| Vaccine | Common AEFI | Serious/Rare AEFI | True Contraindication |
|---|---|---|---|
| BCG | Local ulcer (expected), regional lymphadenitis | Disseminated BCG (immunocompromised) | Symptomatic HIV, SCID |
| DPT/Pentavalent | Fever, local pain/swelling, irritability | Febrile seizures, anaphylaxis | Anaphylaxis to prior dose, encephalopathy after prior DPT |
| OPV | Mild diarrhoea | VAPP (very rare) | Immunodeficiency (use IPV instead) |
| MR/MMR | Fever at 7–12 days, mild rash | Thrombocytopenic purpura (rare) | Anaphylaxis to prior dose, severe immunodeficiency |
| Rotavirus | Mild loose stools | Intussusception (if 1st dose after 15 wk) | Intussusception history; initiation after 15 weeks |
| HepB | Local soreness | Anaphylaxis (very rare) | Anaphylaxis to prior dose |