Page 10 of 53
PE19.4 | Birth Asphyxia — SDL Guide (Part 2)
Diagnosis and Staging of HIE — Sarnat Classification
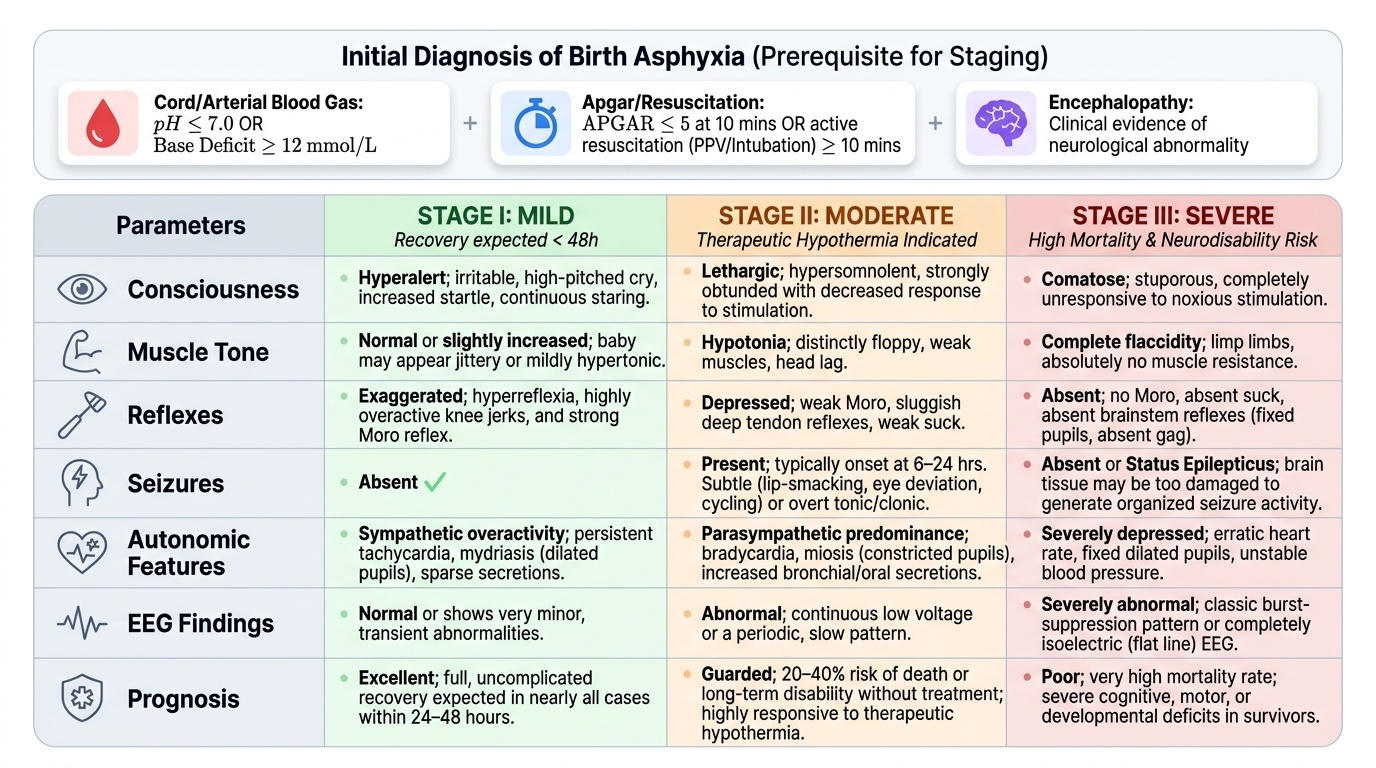
The diagnosis of significant birth asphyxia rests on a combination of clinical criteria and laboratory evidence. No single parameter is sufficient; the diagnosis is based on the totality of evidence. The most commonly used diagnostic criteria (based on NICHD trial entry criteria) include: (a) cord blood or early arterial pH <7.0, OR base deficit >12 mmol/L; (b) APGAR ≤5 at 10 minutes, OR requirement for resuscitation (PPV or intubation) for ≥10 minutes; (c) clinical evidence of encephalopathy. In practical terms, a neonate who required prolonged resuscitation and shows neurological abnormalities on examination warrants careful monitoring for HIE even if cord gas is not available.
Provided image
Sarnat Staging (Sarnat & Sarnat, 1976, validated by multiple subsequent studies) is the bedside clinical classification of HIE severity. It is the gating criterion for therapeutic hypothermia eligibility and the most important examination topic in neonatal neurology for final-year students.
Sarnat Stage I (Mild HIE):
- Consciousness: hyperalert (increased startle, staring)
- Tone: normal or slightly increased (jittery)
- Reflexes: exaggerated (hyperreflexia, strong Moro)
- Seizures: absent
- Autonomic: sympathetic overactivity (tachycardia, mydriasis, sparse secretions)
- EEG: normal or slightly abnormal
- Prognosis: full recovery expected in nearly all cases; resolves within 24–48 hours
Sarnat Stage II (Moderate HIE):
- Consciousness: lethargic (hypersomnia, reduced response to stimulation)
- Tone: hypotonia (floppy)
- Reflexes: depressed (weak Moro, reduced tendon reflexes)
- Seizures: present (typically onset at 6–24 hours; subtle: lip smacking, cycling, eye deviation, apnoea episodes; or overt tonic/clonic)
- Autonomic: parasympathetic predominance (bradycardia, increased secretions, miosis)
- EEG: abnormal (low voltage, periodic pattern)
- Prognosis: 20–40% mortality or major disability without treatment; therapeutic hypothermia indicated
Sarnat Stage III (Severe HIE):
- Consciousness: coma (no response to any stimulation)
- Tone: complete flaccidity
- Reflexes: absent (no Moro, no suck, absent brainstem reflexes — fixed dilated pupils, absent gag)
- Seizures: may be absent (brain too injured to generate organised seizure activity) or status epilepticus
- EEG: burst-suppression or isoelectric (flat)
- Prognosis: high mortality (50–90%); severe disability in most survivors; therapeutic hypothermia indicated but prognosis remains poor
Investigations to support diagnosis and management:
- Cord blood gas / arterial blood gas (first 30–60 min): pH, pCO₂, pO₂, base deficit, lactate. Most informative biochemical marker.
- Blood glucose: hypoglycaemia worsens HIE — maintain glucose >2.6 mmol/L (47 mg/dL)
- Cranial ultrasonography: assesses for haemorrhage, cerebral oedema (slit ventricles), echogenicity changes — available at the bedside, radiation-free
- Amplitude-integrated EEG (aEEG): continuous bedside monitoring of background cerebral electrical activity; helps confirm HIE severity and monitor treatment response
- MRI brain (at 4–7 days): diffusion-weighted imaging (DWI) shows areas of restricted diffusion in the acutely injured brain; most sensitive for predicting neurodevelopmental outcome
SELF-CHECK
A 39-week neonate at 4 hours of age is lethargic, hypotonic, and has had two episodes of lip-smacking movements. Cord blood pH was 7.02, base deficit 14 mmol/L. What is the Sarnat stage and is therapeutic hypothermia indicated?
A. Sarnat I — therapeutic hypothermia not indicated
B. Sarnat II — therapeutic hypothermia indicated if within 6 hours of birth
C. Sarnat III — therapeutic hypothermia indicated but prognosis is guarded
D. Sarnat II — therapeutic hypothermia not indicated because the neonate is still having seizures
Reveal Answer
Answer: B. Sarnat II — therapeutic hypothermia indicated if within 6 hours of birth
The combination of lethargy (altered consciousness), hypotonia, and seizures (lip-smacking = subtle neonatal seizure) in the context of cord blood pH <7.1 and base deficit >12 mmol/L classifies this as Sarnat Stage II (moderate HIE). Therapeutic hypothermia is indicated for Sarnat II and III in neonates ≥36 weeks when initiated within 6 hours of birth. At 4 hours of age, the 6-hour window is still open — initiation should be urgent. Active seizures are not a contraindication to TH; in fact, seizure control (phenobarbitone) and hypothermia are often initiated simultaneously.
Management of Birth Asphyxia and HIE
The management of birth asphyxia and HIE is divided into immediate resuscitation (at birth), stabilisation and supportive NICU care, and the disease-specific intervention of therapeutic hypothermia. The principles of management reflect the dual goal of preventing ongoing injury while supporting organ function during the recovery period.
Immediate management — resuscitation at birth: As detailed in pe11-neonatal-resuscitation, the first priority is effective ventilation and restoration of adequate oxygenation and perfusion. PPV, supplemental oxygen (titrated by pulse oximetry), and chest compressions if HR <60 bpm are initiated per the NRP/HBB algorithm. Avoiding both hyperoxia (which generates excessive ROS) and hypoxia (which perpetuates ischaemia) is important: in HIE, PaO₂ should be maintained at 50–80 mmHg and SpO₂ targeted at 94–98%, not 100%.
Supportive NICU care:
- Glucose homeostasis: maintain blood glucose between 2.6–7.0 mmol/L (47–125 mg/dL); hypoglycaemia worsens neuronal injury. Neonates with HIE often require IV dextrose (10% dextrose at maintenance rate via Holliday-Segar); avoid bolus dextrose (causes rebound hypoglycaemia)
- Fluid management: restrict fluids to 60–80 mL/kg/day initially due to risk of SIADH (syndrome of inappropriate ADH secretion) causing hyponatraemia and cerebral oedema; monitor urine output, serum sodium, and renal function
- Temperature: before hypothermia is initiated, avoid hyperthermia (even 0.5°C above normal worsens HIE outcome) — passive cooling (removing blankets, neutral room temperature) may be appropriate during transfer
- Cardiovascular support: dopamine or dobutamine for hypotension; monitor for HIE-associated cardiomyopathy on echocardiography
- Seizure control: phenobarbitone (phenobarbital) 20 mg/kg IV slow infusion over 30 minutes is the first-line anticonvulsant for neonatal seizures; may repeat 10 mg/kg (total max 40 mg/kg). Second-line: levetiracetam 40–60 mg/kg IV or phenytoin 20 mg/kg IV
- Respiratory: many HIE neonates require mechanical ventilation; avoid hypocapnia (reduces cerebral blood flow)
Therapeutic hypothermia (TH) — the evidence-based neuroprotective treatment:
Therapeutic hypothermia is the only intervention proven to reduce death and neurodisability in moderate-to-severe HIE (TOBY, NICHD, CoolCap trials). The protocol is:
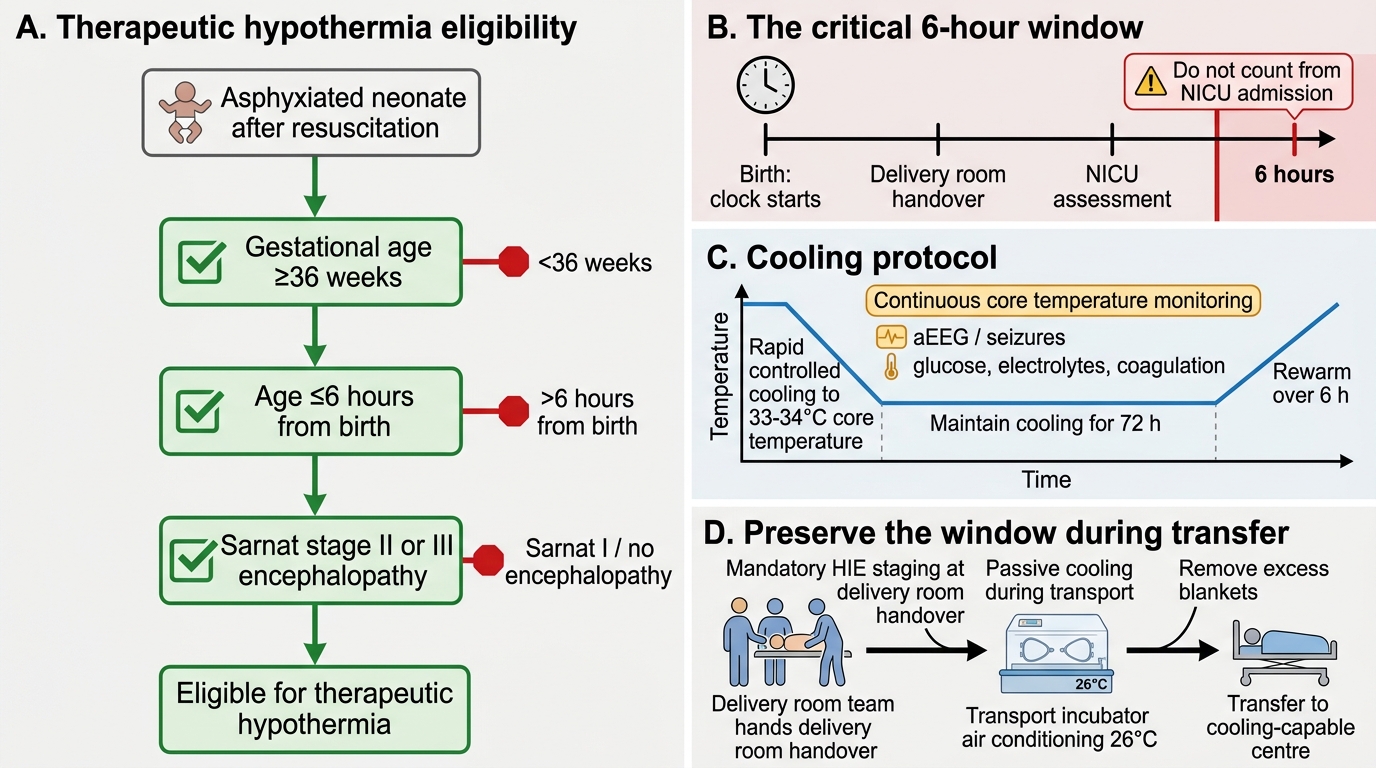
- Eligibility criteria (ALL three must be met):
1. Gestational age ≥36 weeks (evidence base is for near-term/term neonates; efficacy in preterm <34 weeks uncertain, risk of haemorrhage)
2. Sarnat Stage II or III (moderate or severe HIE)
3. Within 6 hours of birth (the latent phase; after 6 hours, secondary failure is established and benefit not demonstrated)
- Method: Whole-body cooling using a servo-controlled cooling blanket OR, where this is unavailable, passive cooling (cold gel packs in improvised systems during transport). Target core temperature 33–34°C (rectal or oesophageal probe), maintained for 72 hours
- Rewarming: gradual, at ≤0.5°C/hour, over approximately 6 hours; rapid rewarming precipitates seizures
- Side effects of TH to monitor: bradycardia, thrombocytopaenia, coagulopathy (clotting screen), hypoglycaemia, hypotension, pulmonary hypertension
- During TH: continue aEEG monitoring; treat seizures; avoid feeding (enteral feeds only after rewarming and clinical stability)
Contraindications to TH: severe congenital anomaly incompatible with life, severe coagulopathy unresponsive to treatment, extreme prematurity <34 weeks.
Therapeutic Hypothermia Eligibility and Protocol
CLINICAL PEARL
The 6-hour window is the most critical number in neonatal neurology — and it is also the most common clinical failure point. After resuscitation of an asphyxiated neonate, teams often focus on stabilisation and forget to ask: 'How old is this baby now, and does it qualify for cooling?' The clock starts at birth, not at the time of admission to the NICU. A neonate born at 2 AM, resuscitated for 10 minutes, stabilised in the delivery room, transferred to the NICU, and finally assessed by the neonatologist at 7 AM has almost certainly missed the window. The solution is to make HIE staging and cooling eligibility assessment a mandatory step at the time of delivery room handover — as routine as assigning the APGAR score. Passive cooling during transport (removing blankets, air conditioning set to 26°C in transport incubator) is a legitimate bridge strategy to preserve the window until the baby reaches a centre equipped for whole-body cooling.
Self-Assessment: Birth Asphyxia Reasoning
Use these integrative scenarios to consolidate your understanding before examinations.
Case 1 — Staging and eligibility: A 37-week neonate born after cord prolapse has cord blood pH 6.95, base deficit 16 mmol/L, APGAR 2 at 5 minutes. At 3 hours of age: lethargic, hypotonic, 3 episodes of tonic eye deviation. What is the Sarnat stage? Is TH indicated? What is the most urgent next action? (Answers: Sarnat Stage II — lethargy + hypotonia + seizures; TH indicated — ≥36 weeks, Sarnat II, within 6 hours; most urgent action = initiate cooling immediately, draw blood for glucose/gas/CBC/coagulation, set up aEEG, start IV dextrose.)
Case 2 — Phenobarbitone dosing: The same neonate develops a generalised tonic seizure at 5 hours of age while awaiting transfer. What do you give? (Answer: Phenobarbitone 20 mg/kg IV slow infusion — for a 3.2 kg baby, this is 64 mg IV over 30 minutes. Check blood glucose before and after.)
Case 3 — Stage III scenario: A term neonate is comatose with fixed dilated pupils, no suck or gag reflex, and a flat EEG. Cord blood pH 6.8. TH is initiated. How would you counsel the parents? (Answer: Sarnat Stage III HIE has very high mortality (50–90%) and severe disability in most survivors even with TH. Honest, compassionate communication with the family is essential — TH is indicated (it reduces the already high risk) but does not guarantee survival or normal outcome.)
Key discriminators:
| Parameter | Value |
|---|---|
| Cord blood pH for significant acidosis | <7.0 (or <7.1 with BD >12) |
| Base deficit threshold | >12 mmol/L |
| Sarnat II hallmarks | Lethargy + hypotonia + seizures |
| Sarnat III hallmarks | Coma + flaccidity + absent brainstem reflexes |
| TH eligibility GA | ≥36 weeks |
| TH window | Within 6 hours of birth |
| TH temperature | 33–34°C core |
| TH duration | 72 hours |
| Rewarming rate | ≤0.5°C/hour over ~6 hours |
| First-line anticonvulsant | Phenobarbitone 20 mg/kg IV |
SELF-CHECK
Therapeutic hypothermia for HIE is indicated when ALL of the following are present EXCEPT:
A. Gestational age ≥36 weeks
B. Sarnat Stage II or III HIE
C. Initiation within 6 hours of birth
D. Active seizures have been controlled with phenobarbitone
Reveal Answer
Answer: D. Active seizures have been controlled with phenobarbitone
Therapeutic hypothermia requires: (1) GA ≥36 weeks, (2) moderate-severe HIE (Sarnat II/III), and (3) initiation within 6 hours of birth. Active seizures are NOT a contraindication to cooling — seizure control with phenobarbitone and cooling are often initiated simultaneously. In fact, seizures in the context of HIE indicate more severe injury (Sarnat II/III) that makes TH MORE, not less, appropriate. Waiting until seizures are controlled before initiating cooling risks missing the 6-hour window.