Page 13 of 53
PE19.5 | Neonatal Respiratory Distress — SDL Guide (Part 2)
Management — RDS, TTN, and MAS
Management of neonatal respiratory distress follows a severity-stratified, condition-specific approach. The common principles are: maintain adequate oxygenation (SpO₂ 91–95% in preterm, 94–99% in term), avoid hyperoxia (causes retinopathy of prematurity in preterm and oxidative injury in all neonates), maintain normothermia and normoglycaemia, and provide nutritional support. Beyond these common supports, each condition has a distinct specific treatment.
Management of RDS:
Prevention — antenatal corticosteroids: This is the most impactful intervention in preterm RDS management. Betamethasone 12 mg IM every 24 hours for 2 doses (or dexamethasone 6 mg IM every 12 hours for 4 doses) given to mothers at risk of delivery between 24 and 34 weeks of gestation (extended to 34+6 weeks in some guidelines) accelerates type II pneumocyte maturation, increases surfactant production, and reduces RDS severity, intraventricular haemorrhage (IVH), necrotising enterocolitis (NEC), and mortality. The steroids should be given ≥24 hours before anticipated preterm delivery for maximum benefit.
Respiratory support:
- CPAP (Continuous Positive Airway Pressure) via nasal prongs at 5–8 cm H₂O: first-line respiratory support for spontaneously breathing preterm neonates with mild-moderate RDS. CPAP keeps alveoli open at end-expiration (functional PEEP), reducing the work of breathing and surfactant consumption. The COIN and CURPAP trials validated CPAP-first as the standard of care.
- Endotracheal intubation + mechanical ventilation: for neonates who fail CPAP (FiO₂ >0.3–0.4, worsening PCO₂, apnoea, severe distress on Silverman-Anderson ≥7)
- Exogenous surfactant therapy: beractant (Survanta) 100 mg/kg (= 4 mL/kg) or poractant alfa (Curosurf) 200 mg/kg (first dose), administered via ETT directly into the trachea. The INSURE technique (INtubate–SURfactant–Extubate to CPAP) minimises ventilator exposure. Surfactant dramatically reduces the work of breathing, improves oxygenation, and reduces pneumothorax risk.
Management of TTN:
TTN is managed conservatively. Supplemental oxygen is given to maintain SpO₂ ≥94%. Oral feeds are withheld while RR is >60/min (risk of aspiration), and IV glucose maintains nutrition. Antibiotics are started if pneumonia cannot be excluded. No specific treatment accelerates lung fluid clearance — the condition resolves as pulmonary lymphatics resorb the retained fluid over 24–72 hours. CPAP is occasionally needed for SpO₂ maintenance. The key management task is monitoring for clinical deterioration that would suggest an alternative diagnosis.
Management of MAS:
Management of MAS is primarily supportive but may require escalating respiratory support:
- Mild MAS: supplemental oxygen, monitoring, minimal stimulation (stimulation precipitates PPHN crises)
- Moderate-severe MAS: CPAP or mechanical ventilation; avoid excessive PIP (worsens air trapping and risk of pneumothorax)
- Surfactant lavage: surfactant (large volume diluted dose) instilled via ETT to dilute and displace meconium; used in severe MAS
- Inhaled nitric oxide (iNO): for PPHN complicating MAS — iNO selectively dilates the pulmonary vasculature, reducing right-to-left shunting and improving oxygenation. Starting dose: 20 ppm
- HFOV (High-Frequency Oscillatory Ventilation): for severe MAS with air leak syndrome
- ECMO (Extra-Corporeal Membrane Oxygenation): last resort for MAS with refractory PPHN at tertiary centres
- Prevention at delivery: for non-vigorous MSAF babies, immediate airway assessment and suctioning under direct vision if meconium visible below the cords
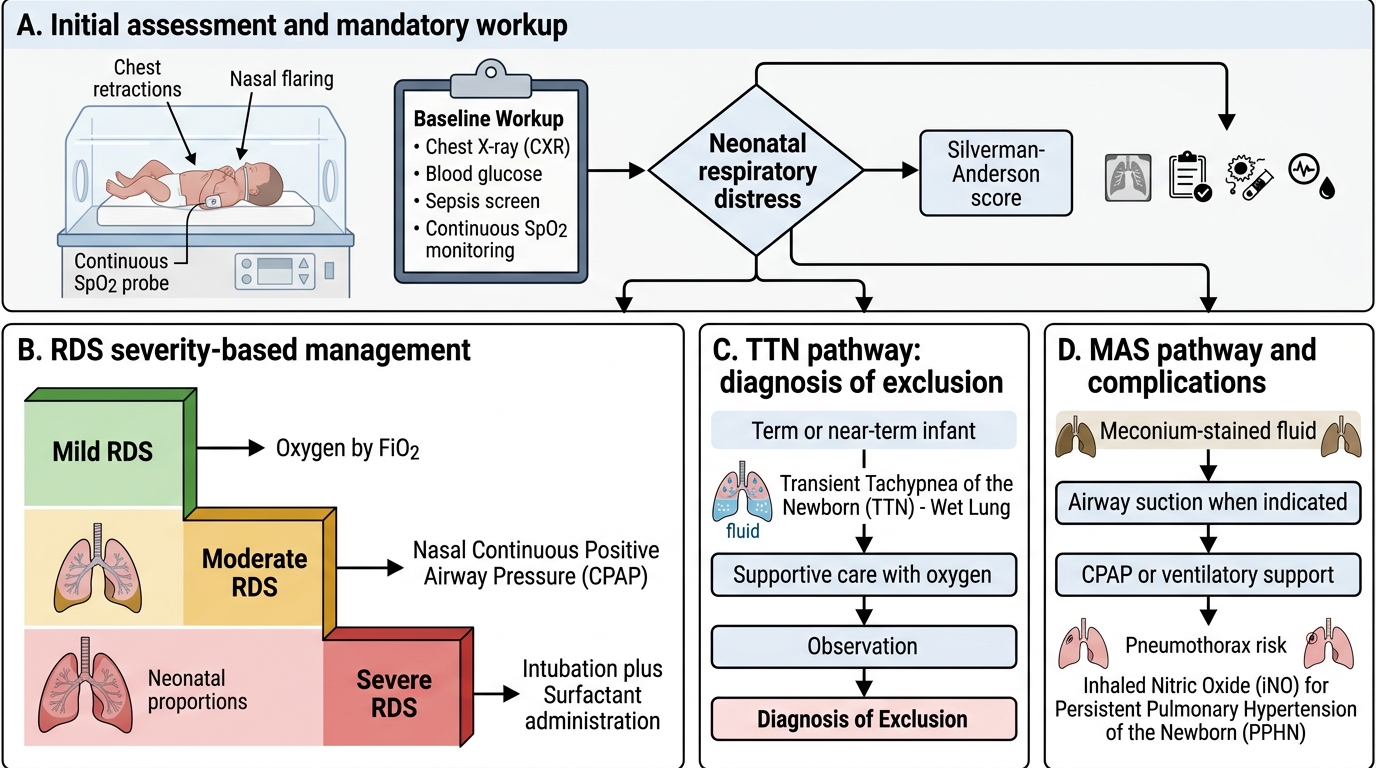
Management Algorithm for Neonatal Respiratory Distress
CLINICAL PEARL
The most dangerous diagnostic error in neonatal respiratory distress is reassurance. TTN is the most common and most benign cause — but it is a diagnosis of exclusion. Before attributing respiratory distress to TTN, you must exclude: neonatal pneumonia (Group B Strep typically presents at 6–12 hours, E. coli at 12–24 hours, indistinguishable from TTN/RDS on X-ray in the first 24 hours), cyanotic congenital heart disease (CHD — the 'hyperoxia test' can help: give 100% O₂ for 10 minutes and measure PaO₂; PaO₂ <150 mmHg suggests intracardiac R-to-L shunt), and pneumothorax (particularly in MAS where air trapping predisposes). The rule: every neonate with respiratory distress gets a CXR, a blood glucose, a sepsis screen, and SpO₂ monitoring — then you make the diagnosis. Never manage a 'presumed TTN' without this baseline workup.
Self-Assessment: Distinguishing Causes of Neonatal Respiratory Distress
Use these discriminating scenarios to practise clinical reasoning before examinations.
Case 1 — The preterm with progressive distress: A 31-week neonate is intubated at birth for severe respiratory distress. CXR: bilateral ground-glass haze, air bronchograms, small lung volumes. ABG: pH 7.22, PaO₂ 45 mmHg, PaCO₂ 58 mmHg on FiO₂ 0.6. Diagnosis? Treatment? (Answers: RDS — give surfactant via ETT: poractant alfa 200 mg/kg or beractant 100 mg/kg. Could the mother have received antenatal betamethasone? If given ≥24 hours before delivery, the course would likely have been milder. INSURE or LISA technique for surfactant delivery if available.)
Case 2 — The term baby after CS: A 38-week neonate born by elective CS has RR 74/min and mild subcostal retractions at 4 hours. CXR shows perihilar streaks and a fluid line in the horizontal fissure. SpO₂ 93% in room air. Diagnosis? Management? (Answers: TTN — supportive care; supplemental oxygen via nasal prongs to target SpO₂ ≥94%; withhold feeds while tachypnoeic; IV glucose; monitor for improvement over 24–72 hours. Reassure parents this is self-limiting.)
Case 3 — MAS with PPHN: A 40+2-week post-term neonate born through thick MSAF is cyanosed at birth (SpO₂ 70% despite FiO₂ 1.0), has grunting and barrel chest, CXR shows hyperinflation with patchy bilateral opacities. Echo: right ventricular hypertension, right-to-left ductal shunting. Diagnosis? Specific treatment? (Answers: MAS with PPHN — intubate and ventilate, minimise stimulation, surfactant lavage, inhaled nitric oxide 20 ppm for PPHN, avoid metabolic acidosis, refer for ECMO if refractory.)
Key discriminators table:
| Silverman-Anderson score | Interpretation | Action |
|---|---|---|
| 0 | No distress | Routine care |
| 1–3 | Mild distress | Supplemental O₂, monitoring |
| 4–6 | Moderate distress | CPAP, investigations |
| ≥7 | Severe distress | NICU, consider intubation |
Three-condition discrimination summary:
| Feature | RDS | TTN | MAS |
|---|---|---|---|
| GA | <34 wk | Term/late preterm | Term/post-term |
| CXR hallmark | Ground-glass + air bronchograms | Perihilar streaks + fissure fluid | Hyperinflation + patchy opacities |
| Specific treatment | Surfactant + CPAP | Supportive only | CPAP ± iNO for PPHN |
| Prevention | Antenatal corticosteroids | Labour before CS | Avoid post-term; manage MSAF |
SELF-CHECK
Antenatal corticosteroids (betamethasone) are given to reduce the severity of RDS. Their primary mechanism is:
A. Directly replacing surfactant in fetal alveoli
B. Accelerating type II pneumocyte maturation and surfactant synthesis
C. Preventing preterm labour and extending gestational age
D. Reducing fetal lung fluid production in the third trimester
Reveal Answer
Answer: B. Accelerating type II pneumocyte maturation and surfactant synthesis
Antenatal corticosteroids act by accelerating the maturation of type II alveolar pneumocytes and upregulating the enzymes responsible for surfactant phospholipid synthesis (particularly DPPC). This increases both the quantity and composition quality of surfactant available at birth, making alveolar collapse at end-expiration less likely and reducing RDS severity. They do not directly replace surfactant (that is what exogenous surfactant therapy does postnatally), do not consistently prevent preterm labour, and do not primarily reduce lung fluid production (that effect is minor compared to their surfactant-stimulating action).