Page 37 of 53
PE19.13-14 | Neonatal Sepsis — SDL Guide
Learning Objectives
- Describe the clinical features of neonatal sepsis, recognising that early signs are non-specific and require a high index of suspicion
- Distinguish early-onset sepsis (EOS) from late-onset sepsis (LOS) by timing, organisms, and risk factors
- Describe the features of perinatal (TORCH) infections and their congenital sequelae
- Interpret the neonatal sepsis screen and explain the role of blood culture as the gold standard
- Prescribe weight-based empirical antibiotic therapy for EOS and LOS, and outline supportive management
INSTRUCTIONS
Neonatal sepsis is the third leading cause of neonatal mortality in India, accounting for approximately 19% of all neonatal deaths (National Family Health Survey). The challenge is that its early clinical features — poor feeding, temperature instability, lethargy — are shared with virtually every other neonatal illness, including hypoglycemia, metabolic disorders, and HIE. A high index of clinical suspicion, a structured diagnostic approach using the sepsis screen and blood culture, and prompt empirical antibiotic therapy are the core skills this module develops. This SDL also covers perinatal infections (PE19.14), the TORCH group, because they share the clinical presentation of a 'sick neonate' but require entirely different investigations and management.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 7 — Neonatal Sepsis and Infections (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 123 — Neonatal Sepsis and Infections (textbook)
- NNF India — Evidence-Based Clinical Practice Guidelines: Management of Neonatal Sepsis (2020) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-hour-old, 2.2 kg neonate born at 37 weeks is brought by the nurse because 'she is not feeding well and looks pale.' The mother had prolonged rupture of membranes for 22 hours before delivery. On examination, the baby's temperature is 36.0°C (below normal), respiratory rate is 68/minute, there is mild intercostal recession, and the baby is lethargic with a weak cry. Blood glucose is 44 mg/dL. Is this sepsis? What organisms must you cover empirically? What investigations do you order, and what antibiotic regimen do you start — and at what weight-based dose?
WHY THIS MATTERS
Neonatal sepsis (systemic infection in the first 28 days of life) affects approximately 2–4% of all live births in India but has a mortality rate of 10–40% in resource-limited settings, making it the third leading cause of neonatal death nationally. The causative organisms differ fundamentally between early-onset and late-onset disease, and choosing the wrong empirical regimen — for instance, treating an EOS case caused by Group B Streptococcus with only gentamicin (which has poor streptococcal coverage) — can be fatal. Perinatal infections from the TORCH group (Toxoplasma, rubella, CMV, herpes, syphilis, hepatitis B) cause congenital infection with sequelae ranging from hearing loss and chorioretinitis to microcephaly and cardiac defects — many of which are preventable with antenatal screening and neonatal prophylaxis. Recognising the overlap between these conditions and other neonatal emergencies is one of the most important clinical skills in neonatology.
RECALL
From Immunology and Physiology, recall that neonates have several innate immune deficiencies that explain their disproportionate susceptibility to infection. Maternal immunoglobulin G (IgG) is transferred across the placenta, predominantly in the third trimester — so preterm neonates have particularly low serum IgG levels. IgM and IgA do not cross the placenta, so the neonate has no pre-existing adaptive antibody response to most pathogens. Neutrophil production is limited: the bone marrow neutrophil storage pool in neonates is only 20–30% of adult capacity, and it is rapidly depleted during overwhelming sepsis — leading to neutropenia (a bad prognostic sign). The complement system is immature, with C3 and opsonising capacity reduced to 50–70% of adult levels. Pattern recognition (toll-like receptor signalling) is functional but produces an exaggerated inflammatory cytokine response to gram-negative lipopolysaccharide (LPS), explaining why gram-negative sepsis is particularly severe in neonates. From microbiology, recall that Group B Streptococcus (GBS, Streptococcus agalactiae) colonises the maternal genital tract in 15–30% of women and is the leading cause of EOS in developed countries, though in India Klebsiella and E. coli are more common.
Clinical Presentation of Neonatal Sepsis
The clinical presentation of neonatal sepsis is notoriously non-specific. Unlike older children or adults who develop fever, rigors, and localising signs, neonates often manifest sepsis through subtle, non-localising changes in behaviour and physiology that are easily attributed to feeding difficulties, cold stress, or normal newborn variation. The bedside maxim for neonatal sepsis is the 'rule of not-doing-well': any neonate who is not feeding well, not looking well, or not acting like themselves requires urgent sepsis evaluation, regardless of whether a specific source is identified. A high index of clinical suspicion — particularly in neonates with known risk factors such as prolonged rupture of membranes, maternal fever, or prematurity — is the most important diagnostic tool.
Early non-specific signs (present in >80% of neonatal sepsis):
- Poor feeding, weak suck, feeding refusal — often the first sign noticed by the mother or nurse
- Lethargy, reduced activity, hypotonia — the baby is less responsive than expected
- Temperature instability — either fever (>38°C axillary) or hypothermia (<36°C); hypothermia is more common in preterm and LBW neonates and is a worse prognostic sign than fever
- Respiratory distress — tachypnoea (RR >60/min), grunting, intercostal recession, apnoea in preterm neonates
- Pallor, mottling, poor peripheral perfusion — prolonged capillary refill time >3 seconds; indicates cardiovascular compromise
Later/severe signs (indicate systemic involvement):
- Jaundice — unconjugated or conjugated (direct) jaundice can be a sepsis sign; gram-negative sepsis classically causes conjugated hyperbilirubinaemia with hepatitis
- Abdominal distension — ileus from sepsis; may indicate necrotising enterocolitis (NEC) in preterm neonates
- Seizures — from meningitis, metabolic disturbances, or direct cerebral involvement
- Bleeding tendencies — disseminated intravascular coagulation (DIC) in overwhelming sepsis
- Sclerema — hardening of subcutaneous tissue; indicates severe sepsis and hypothermia in LBW neonates; poor prognosis
The skin is an important examination site: petechiae or purpura suggest gram-negative sepsis or thrombocytopenia; vesicles suggest HSV; a diffuse maculopapular rash with hepatosplenomegaly may suggest congenital syphilis or CMV.
Aetiology: EOS vs LOS and Perinatal Infections
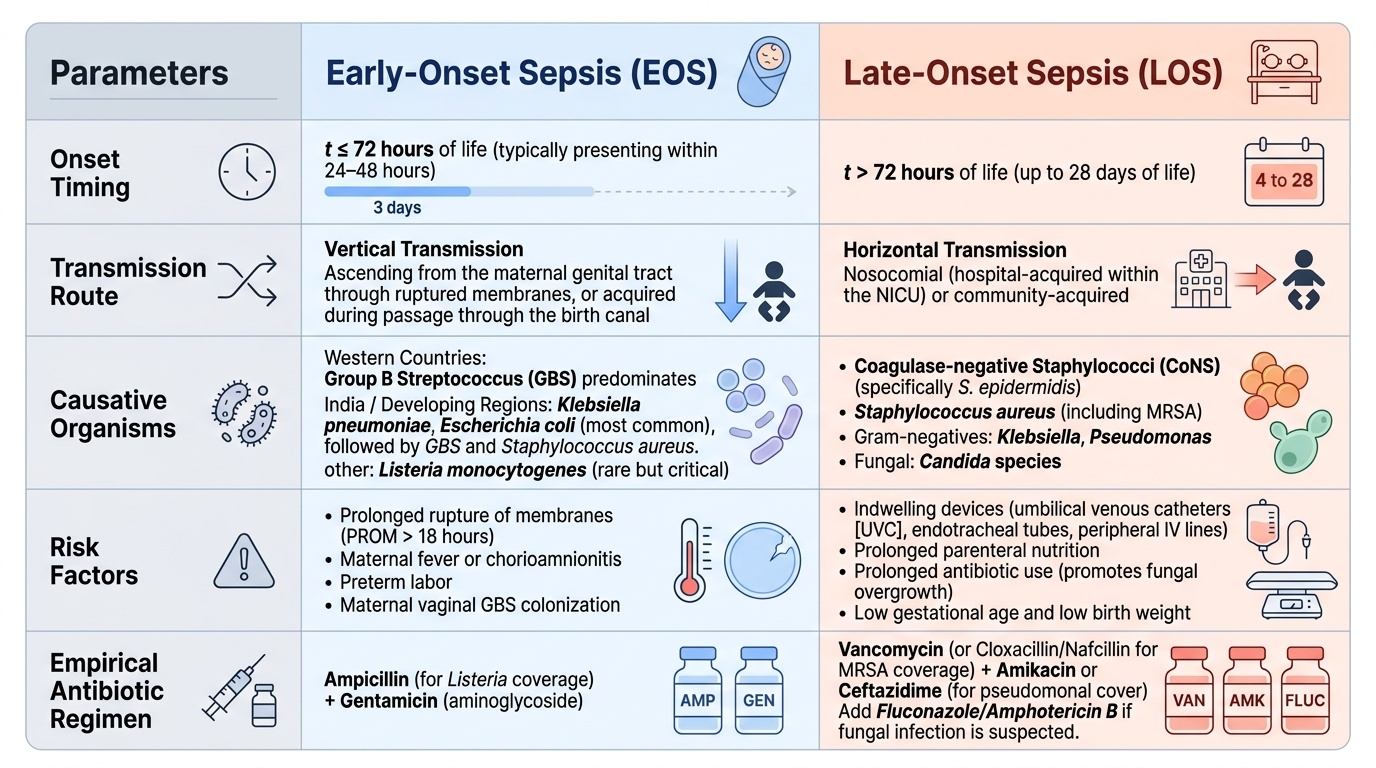
The aetiology of neonatal sepsis is fundamentally shaped by the route of transmission. Early-onset sepsis (EOS), presenting within the first 72 hours of life, results from vertical transmission — organisms colonising the maternal genital tract ascend through ruptured membranes or are acquired during passage through the birth canal. The characteristic risk factors are prolonged rupture of membranes (>18 hours), maternal fever, chorioamnionitis, preterm labour, and GBS vaginal colonisation. The organism profile in EOS reflects the maternal genital flora: in India, Klebsiella pneumoniae and Escherichia coli are the most common EOS pathogens, followed by Group B Streptococcus (GBS) and Staphylococcus aureus. In Western countries, GBS predominates. Listeria monocytogenes, though rare, is an important cause of EOS associated with granulomatosis infantiseptica and must be covered by ampicillin.
Provided image
Late-onset sepsis (LOS), presenting after 72 hours (and up to 28 days), is predominantly nosocomial in hospitalised neonates or community-acquired in those discharged home. In the NICU, coagulase-negative staphylococci (CoNS, particularly Staphylococcus epidermidis), Staphylococcus aureus (including MRSA), Klebsiella, Pseudomonas, and Candida spp. are the dominant LOS pathogens. Risk factors include indwelling devices (umbilical venous catheters, endotracheal tubes, peripheral IV lines), prolonged parenteral nutrition, prolonged antibiotic use (promotes Candida overgrowth), low gestational age, and low birth weight.
Perinatal infections (TORCH) represent a distinct group of congenital infections transmitted transplacentally or at delivery, causing multisystem disease:
- Toxoplasma gondii: triad of chorioretinitis, intracranial calcifications, and hydrocephalus; treatment with pyrimethamine + sulphadiazine
- Other — congenital syphilis: Treponema pallidum; snuffles, hepatosplenomegaly, periostitis, skin rash, saddle nose, interstitial keratitis; treated with benzathine penicillin. Hepatitis B: perinatal transmission (HBeAg-positive mothers); prevented with HBIg + HBV vaccine within 12 hours
- Rubella: first trimester infection → deafness, cataracts, cardiac defects (PDA, pulmonary artery stenosis), blueberry muffin rash
- CMV (cytomegalovirus): most common congenital infection; IUGR, microcephaly, periventricular calcifications, petechiae, hepatosplenomegaly, sensorineural hearing loss; ganciclovir for symptomatic cases
- HSV (herpes simplex): acquired at delivery (HSV-2 genital herpes); three forms — SEM (skin-eye-mouth), disseminated, CNS; acyclovir 60 mg/kg/day IV × 14–21 days
Pathophysiology: Host Defences and Immune Immaturity
The extraordinary susceptibility of neonates to bacterial infection — and the severity of sepsis when it occurs — reflects a combination of quantitative and qualitative immune deficiencies that are intrinsic to normal neonatal development. These deficiencies are not pathological; they represent the immature state of a system that is adapted to the sterile intrauterine environment and has not yet been 'trained' by environmental microbial exposure. Understanding these deficiencies explains why certain organisms — particularly gram-negative bacilli and encapsulated bacteria — are disproportionately dangerous in neonates, and why standard infection-control measures in the NICU (hand hygiene, catheter bundles, rational antibiotic stewardship) are neonatal safety imperatives rather than optional practices.
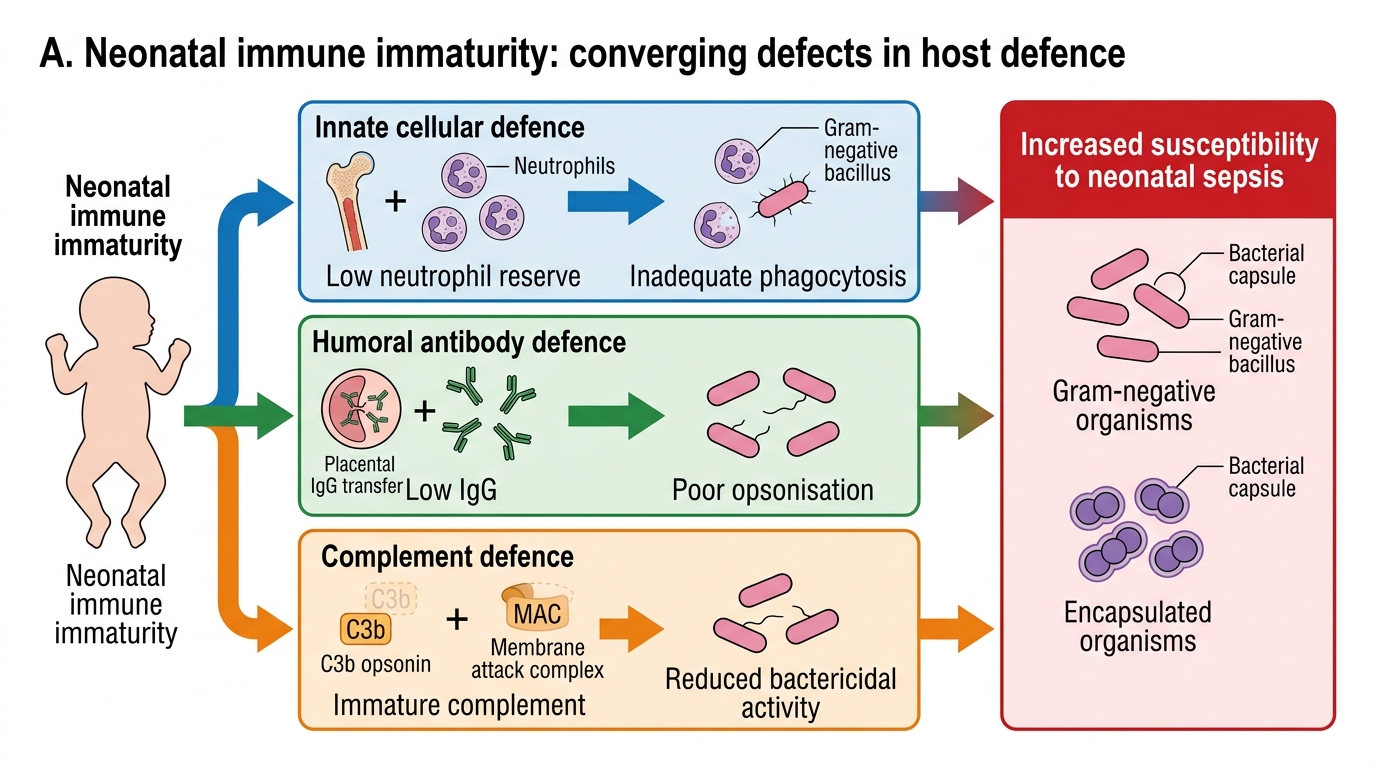
The principal immune deficiencies in neonates are:
1. Reduced neutrophil reserve: Neonates have a bone marrow neutrophil storage pool only 20–30% of adult size. During overwhelming gram-negative sepsis, circulating neutrophils are rapidly consumed; the bone marrow cannot replenish them fast enough, leading to neutropenia (absolute neutrophil count <1,500/µL in the neonate). Neutropenia in the context of clinical sepsis is a marker of severe disease and significantly worsens prognosis.
2. Low immunoglobulin: Maternal IgG crosses the placenta from 32 weeks onward (active transport via FcRn receptors on syncytiotrophoblast). Preterm neonates have correspondingly lower IgG — a 28-week neonate may have only 30–40% of term IgG levels. IgM and secretory IgA are absent at birth (both must be synthesised by the neonate). The result is markedly reduced opsonisation capacity, particularly against gram-negative organisms and encapsulated bacteria (GBS, Haemophilus, Pneumococcus) that rely on antibody-mediated phagocytosis.
3. Immature complement: The classical and alternative complement pathways are present but at reduced activity (50–70% of adult). This reduces the membrane attack complex-mediated killing of gram-negative organisms and reduces C3b-mediated opsonisation.
4. Impaired natural killer (NK) cells and T-cell function: Neonatal T-cells have a Th2-skewed cytokine profile (promotes tolerance, not inflammation — appropriate for the immunologically novel intrauterine environment), which reduces Th1-mediated intracellular pathogen clearance. This impairs defence against Listeria, CMV, HSV, and mycobacteria.
Neonatal Immune Immaturity and Sepsis Susceptibility
SELF-CHECK
A 36-hour-old neonate born after 24 hours of rupture of membranes has temperature 36.0°C, poor feeding, and tachypnoea. The sepsis screen shows TLC 3,800/µL, I:T ratio 0.28, CRP 2.1 mg/dL, and micro-ESR 18 mm/hr. How many sepsis screen criteria are positive, and what does this mean?
A. 2 criteria positive — screen negative, observe without antibiotics
B. 3 criteria positive — screen positive, start empirical antibiotics
C. 4 criteria positive — screen positive, start empirical antibiotics
D. 5 criteria positive — screen positive, but blood culture is still needed before starting antibiotics
Reveal Answer
Answer: C. 4 criteria positive — screen positive, start empirical antibiotics
The NNF sepsis screen criteria are: TLC <5,000 or >15,000/µL; I:T ratio >0.2; CRP >1 mg/dL; micro-ESR >15 mm/hr (first 7 days); gastric aspirate polymorphs >5/HPF. In this case: TLC 3,800/µL (positive, <5,000), I:T ratio 0.28 (positive, >0.2), CRP 2.1 mg/dL (positive, >1), micro-ESR 18 mm/hr (positive, >15) = 4 criteria positive. A screen is positive if ≥3 of 5 criteria are met. 4 positive criteria is a strongly positive screen — start empirical antibiotics immediately after taking a blood culture. Waiting for culture results before starting antibiotics in a sick neonate is wrong; treatment must not be delayed.