Page 10 of 16
PE15.3-4 | Emergency Vascular Access — SDL Guide (Part 3)
Self-Assessment: Vascular Access Scenarios
The following scenarios test your ability to apply the decision rules and technique knowledge from this module to realistic clinical situations. For each, decide on the correct action before reading the answer. These scenarios represent the type of reasoning you will need to demonstrate in both the OSCE and in real paediatric emergencies.
Provided image
Scenario A: A 3-year-old girl is brought to casualty in septic shock. GCS 9/15, HR 180, BP unrecordable. Two nurses have attempted IV cannulation in both antecubital fossae — no success after 90 seconds. You are the intern on duty. What do you do?
Answer: Proceed immediately to IO access at the proximal tibia. The 90-second / 2-attempt threshold has been reached in a critically ill child. Do not attempt a third peripheral IV. While you establish IO access, another team member should continue resuscitation (oxygen, airway positioning). Once IO is confirmed, give a 20 mL/kg IV fluid bolus (Ringer's lactate or normal saline) as per septic shock protocol.
Scenario B: You have inserted an IV cannula in a 10-month-old infant and flushed 2 mL of normal saline. The area around the cannula tip swells and feels boggy, and the infant cries loudly. What has happened and what do you do?
Answer: Extravasation/infiltration — the cannula tip has exited the vein. Remove the cannula immediately. Elevate the limb and apply a cold compress. Because only normal saline was given, no tissue necrosis risk. Attempt another IV site; if two attempts fail, proceed to IO.
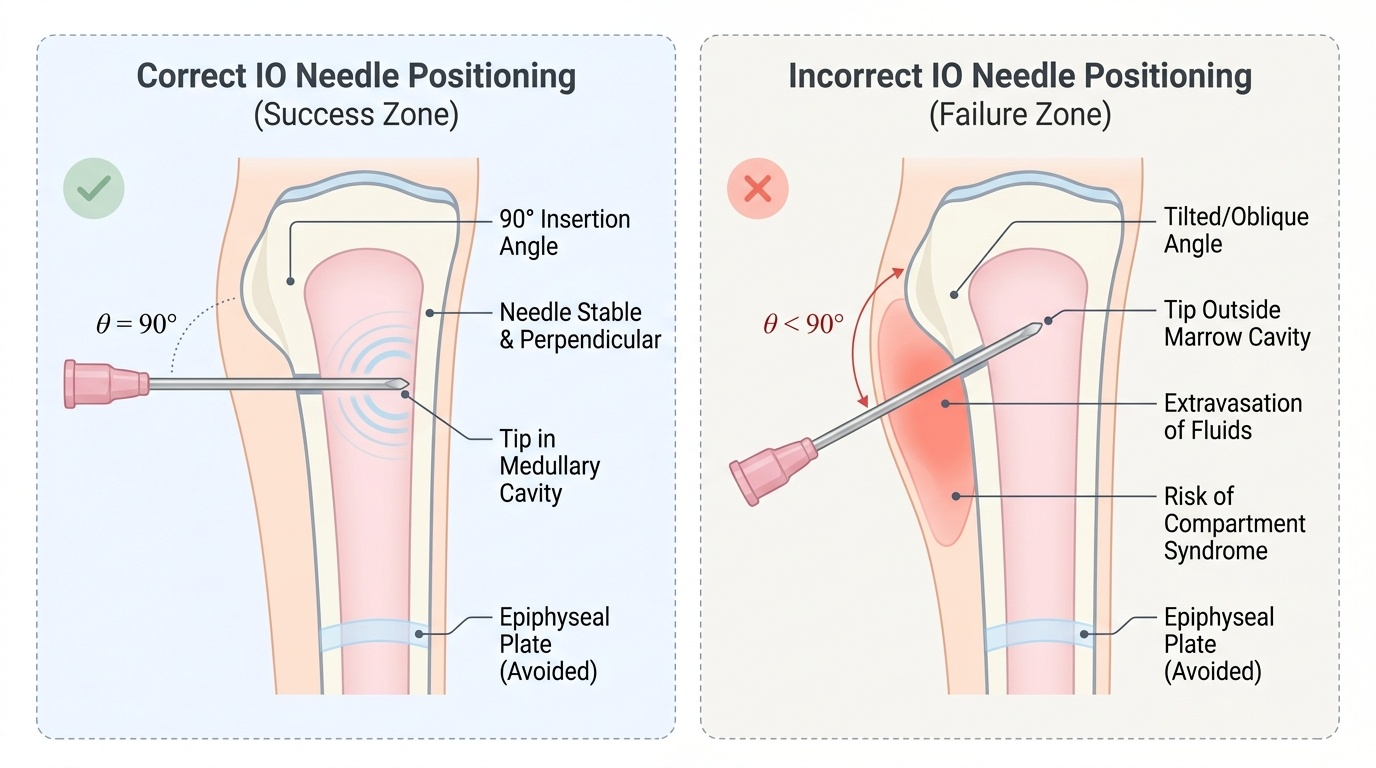
Scenario C: You attempt IO insertion in the proximal tibia of a 2-year-old. After drilling, the needle stands upright. You flush 8 mL of normal saline. During infusion the nurses notice the child's calf is becoming progressively swollen and tense. What is the diagnosis, and what do you do?
Answer: Posterior compartment leakage / early compartment syndrome — fluid is tracking into the posterior tibial compartment, likely from a needle that passed through both cortices or from tissue plane extravasation. Stop the IO infusion immediately. Remove the IO needle. Elevate the limb and monitor neurovascular status (sensation, capillary refill, pain on passive stretch). Notify a surgeon urgently if compartment syndrome is suspected.
CLINICAL PEARL
The IO needle IS an IV line for drug purposes. Every drug and fluid that can be given IV can be given IO in a resuscitation — including adrenaline, atropine, adenosine, sodium bicarbonate, glucose, blood products, and all standard IV antibiotics. The only differences are: (1) a saline flush of 5-10 mL after each drug pushes it from the marrow into the central circulation; (2) infusion pressures are slightly higher for IO than peripheral IV — use a pressure bag or a syringe pump set to deliver against higher resistance if gravity drip flow is slow. Do not hesitate to use IO — a correctly placed IO line in a child in cardiac arrest is life-saving within seconds of insertion.