Page 4 of 16
PE15.2 | Sodium Potassium Imbalance — SDL Guide
Learning Objectives
- Recognise the clinical features of sodium and potassium disorders in children
- Explain the pathophysiology and common aetiologies of hyponatraemia, hypernatraemia, hypokalaemia, and hyperkalaemia
- Interpret a serum electrolyte report in clinical context
- Describe the safe management of sodium and potassium imbalance, including correction rates and emergency interventions
INSTRUCTIONS
Electrolyte disorders — particularly sodium and potassium imbalance — are among the most common and potentially dangerous abnormalities encountered in hospitalised children. A serum electrolyte report is one of the investigations you will interpret most frequently, and errors in correction rate can cause worse outcomes than the disorder itself. Rapid correction of chronic hyponatraemia can cause osmotic demyelination; inadequately treated hyperkalaemia can cause fatal arrhythmias. This module builds on your understanding of fluid physiology from the previous session and equips you to interpret and act safely on electrolyte results.
References
- Ghai Essential Pediatrics, 9th ed, Ch 18 (Fluid and Electrolyte Disturbances) (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Ch 68-69 (Electrolyte Disturbances) (textbook)
- IAP Standard Treatment Guidelines — Fluid and Electrolyte Management (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 7-year-old girl with nephrotic syndrome on long-term furosemide presents with generalised weakness and muscle cramps. Her electrolyte report shows: Na 128 mmol/L (normal 135-145), K 2.8 mmol/L (normal 3.5-5.5), Cl 90 mmol/L, bicarbonate 30 mmol/L. The ECG shows flattened T waves and prominent U waves. She is alert but drowsy with mild leg oedema. Her mother is alarmed — the doctor says she has 'low salt AND low potassium'. How do you interpret this report, and how do you correct it safely?
WHY THIS MATTERS
Sodium and potassium are the two most clinically critical electrolytes in paediatric practice. Sodium governs extracellular osmolality and therefore cell volume — a falling sodium causes brain cells to swell (risk of seizures and herniation) and a rapidly rising correction can shrink oligodendrocytes causing permanent osmotic demyelination. Potassium governs the resting membrane potential of myocardium and skeletal muscle — both hypokalaemia and hyperkalaemia produce life-threatening arrhythmias. These disorders are common in children with diarrhoea, renal disease, malnutrition, and on diuretics or IV fluids. Every doctor must be able to interpret an electrolyte report, identify the disorder's mechanism, and correct it at a safe rate.
RECALL
Before proceeding, recall: (1) What is the normal serum sodium range? Which osmoreceptors regulate ADH release, and how does aldosterone differ in its role? (2) What is the normal serum potassium range, and why does potassium have such a powerful effect on cardiac conduction despite its low extracellular concentration? (3) From your previous session on fluid requirements: how does severe diarrhoea affect both sodium and potassium simultaneously? Bring these mechanisms to mind before exploring the disorders below.
Clinical Presentation of Electrolyte Disorders
Electrolyte disorders rarely present with textbook-pure manifestations; they usually occur alongside the primary illness that caused them. However, recognising the clinical pattern pointing to a specific electrolyte abnormality is the trigger for ordering the report and the starting point for safe management. The severity of symptoms broadly correlates with the magnitude of the abnormality and, critically, with the speed at which it developed — a sodium of 125 mmol/L that developed over 48 hours causes far fewer symptoms than the same level reached in 4 hours.
Provided image
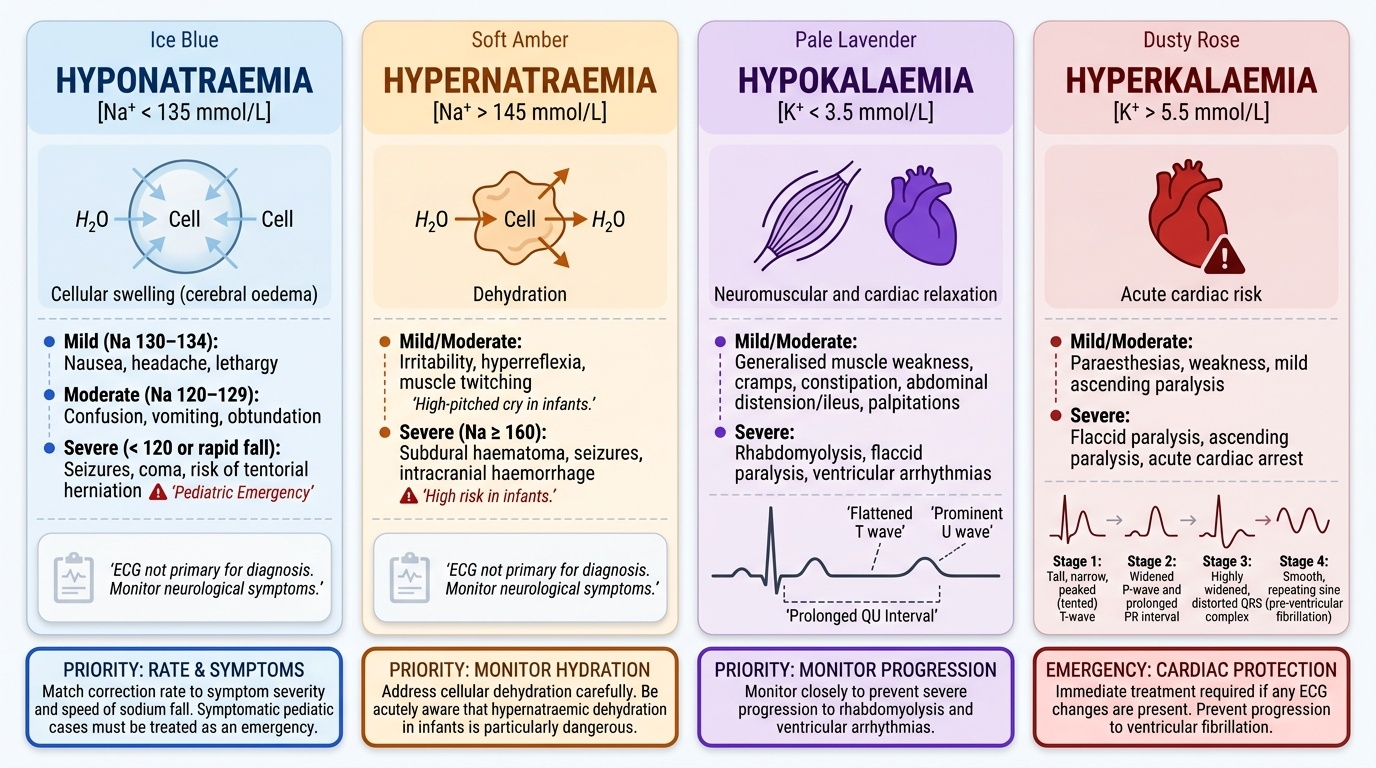
Hyponatraemia (Na < 135 mmol/L): Symptoms reflect cerebral oedema from water entry into brain cells. Mild (Na 130-134): nausea, headache, lethargy. Moderate (Na 120-129): confusion, vomiting, obtundation. Severe (Na < 120 or rapid fall): seizures, coma, risk of tentorial herniation. In children, symptomatic hyponatraemia must be treated as an emergency.
Hypernatraemia (Na > 145 mmol/L): Symptoms reflect cellular dehydration from water drawn out of cells. Irritability, high-pitched cry, hyperreflexia, muscle twitching. Severe hypernatraemia (Na > 160) may cause subdural haematoma from venous sinus stretching, seizures, or intracranial haemorrhage. Hypernatraemic dehydration in infants is particularly dangerous.
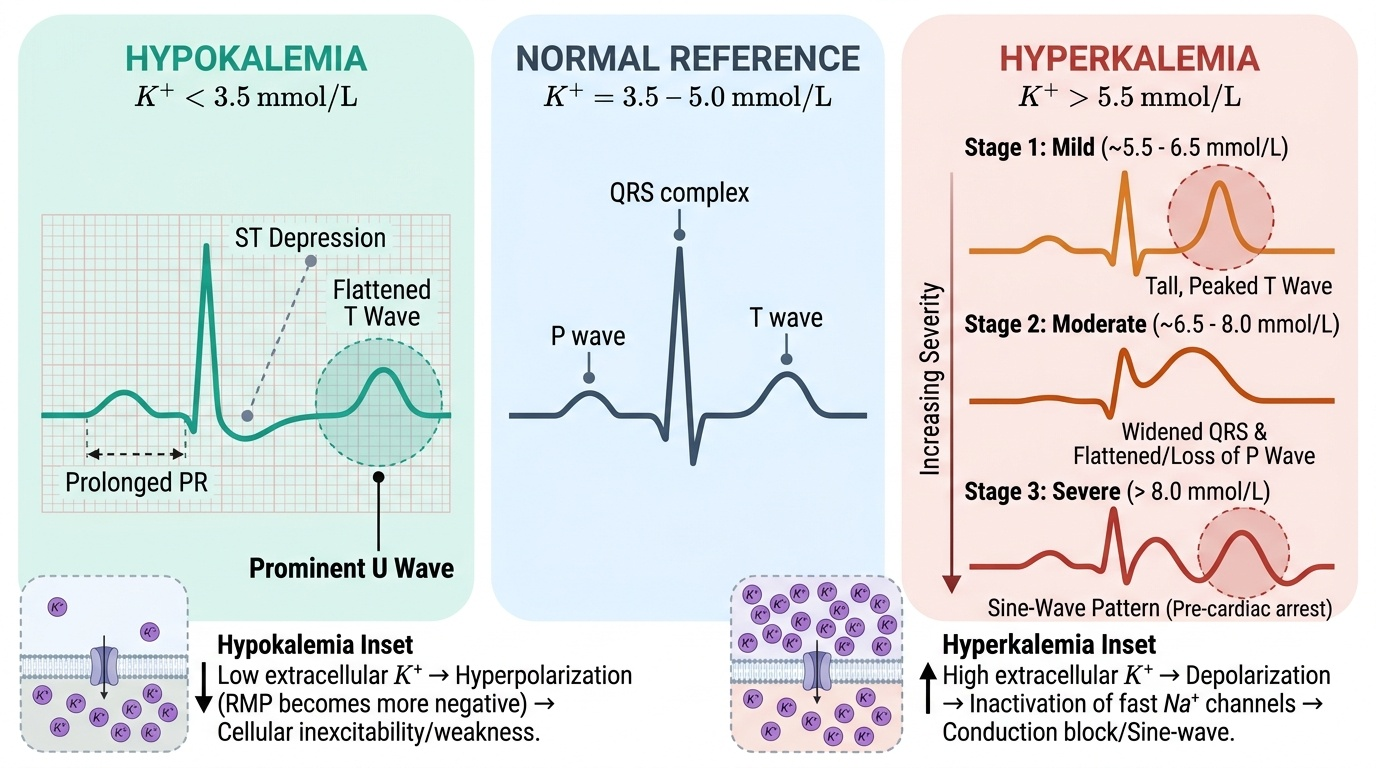
Hypokalaemia (K < 3.5 mmol/L): Generalised muscle weakness (may progress to paralysis), cramps, constipation, abdominal distension (ileus), palpitations. ECG: flattened T waves, prominent U waves (a positive deflection after the T wave), prolonged QU interval. Severe hypokalaemia causes rhabdomyolysis and ventricular arrhythmia.
Hyperkalaemia (K > 5.5 mmol/L): Paraesthesias, weakness, ascending paralysis. ECG changes are the critical warning: peaked/tented T waves (earliest), followed by widened P wave, prolonged PR, wide QRS, and finally the sine-wave pattern preceding ventricular fibrillation. Any ECG change with hyperkalaemia demands immediate treatment.
- Hyponatraemia symptoms → match symptom severity to sodium level and rate of fall
- Hypokalaemia ECG → flattened T + U waves (before arrhythmia)
- Hyperkalaemia ECG → peaked T waves → wide QRS → sine wave → VF
Pathophysiology and Aetiology of Sodium Disorders
Understanding sodium disorders requires understanding that serum sodium reflects not just sodium balance but the ratio of total body sodium to total body water. Hyponatraemia most often results from excess free water relative to sodium, and hypernatraemia from water deficit relative to sodium. Categorising hyponatraemia by volume status is the key diagnostic step.
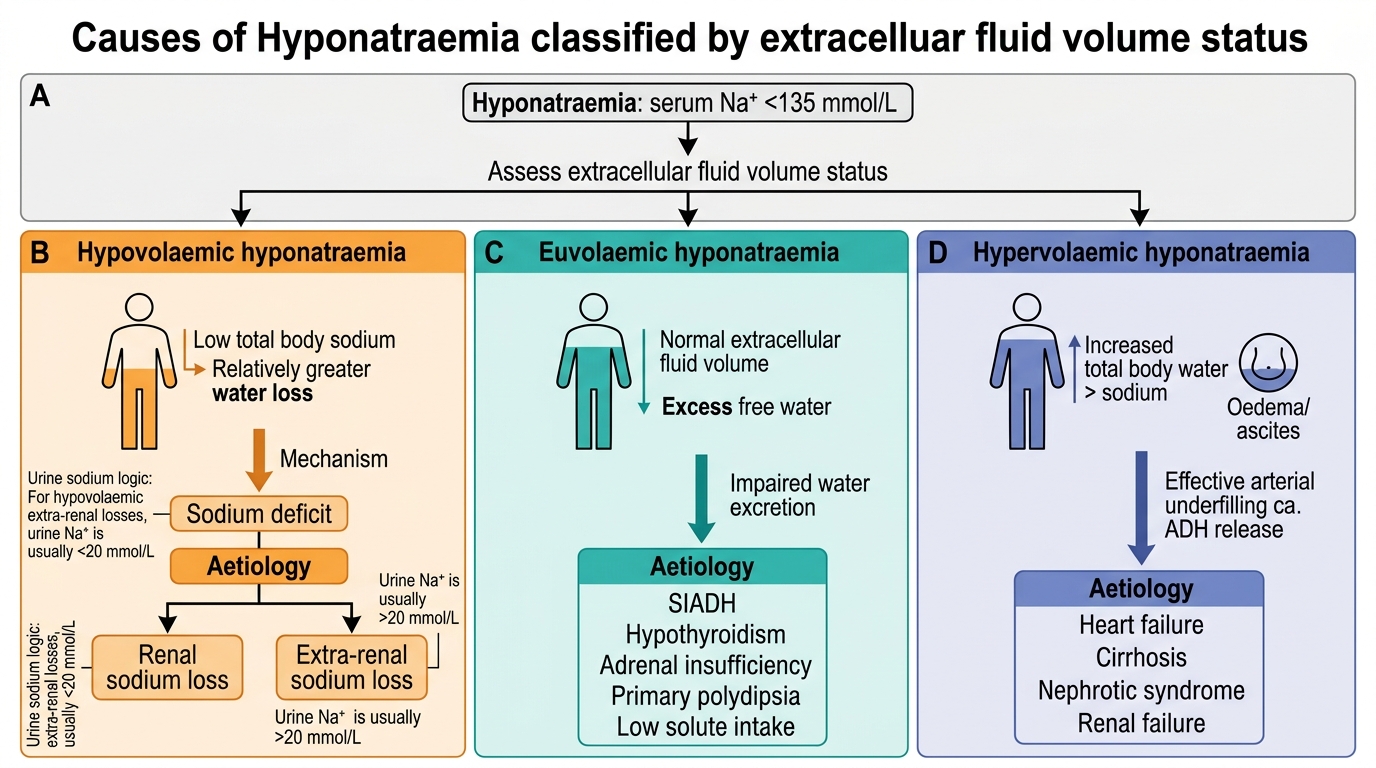
Hyponatraemia (Na < 135 mmol/L) by volume status:
Hypovolaemic hyponatraemia (low total body sodium AND water, but Na loss > water loss): most common in children — diarrhoea with hypotonic replacement, vomiting, diuretic use, adrenal insufficiency. The urinary sodium helps: renal losses have urine Na > 20 mmol/L; extra-renal losses (diarrhoea, vomiting) have urine Na < 10 mmol/L.
Euvolaemic hyponatraemia: SIADH (syndrome of inappropriate antidiuretic hormone secretion) — ADH is secreted despite normal or low plasma osmolality, causing free water retention. Causes in children: CNS disease (meningitis, encephalitis, head injury), pulmonary disease, pain, post-operative state, certain drugs (carbamazepine, SSRIs). Characterised by urine Na > 20 mmol/L and urine osmolality > plasma osmolality in a euvolaemic patient.
Hypervolaemic hyponatraemia (both sodium and water increased, but water excess > sodium excess): nephrotic syndrome, nephritic syndrome, cardiac failure, cirrhosis, severe malnutrition (kwashiorkor). The kidney retains sodium avidly (low urine Na < 10) despite dilutional hyponatraemia because of perceived underfilling.
Hypernatraemia (Na > 145 mmol/L): almost always reflects water deficit exceeding sodium deficit, or sodium excess relative to water. Common causes in children: (1) Inadequate water intake — poor breastfeeding, inability to access fluids (unconscious child), diabetes insipidus; (2) Excess water loss — high fever, tachypnoea, diarrhoea with hypotonic stools, burns; (3) Excess sodium intake — incorrectly prepared hypertonic feeds, inappropriate IV sodium bicarbonate. In hypernatraemic dehydration (common in breastfed neonates with poor intake), the child may appear deceptively well despite significant fluid deficit because hypernatraemia maintains ECF volume at the expense of intracellular water.
Causes of Hyponatraemia by Volume Status
Pathophysiology and Aetiology of Potassium Disorders
Potassium is the principal intracellular cation, with only 2% of total body potassium in the extracellular fluid. This small extracellular pool is tightly regulated because it determines the resting membrane potential (RMP) of excitable cells — cardiac myocytes, skeletal muscle, and neurons. The RMP is largely determined by the ratio of intracellular to extracellular potassium (the Nernst equation). Even small changes in serum potassium significantly alter this ratio and therefore cellular excitability, explaining why potassium disorders have such profound electrophysiological consequences.
Provided image
Hypokalaemia (K < 3.5 mmol/L): The extracellular K falls relative to intracellular K, hyperpolarising the cell membrane and making it harder to reach threshold — hence the weakness and arrhythmias (a hyperpolarised myocyte is resistant to normal conduction). Causes in children:
• Gastrointestinal losses: diarrhoea (most common), vomiting, nasogastric suction; diarrhoeal stool is rich in K (20-40 mmol/L)
• Urinary losses: diuretic therapy (loop diuretics — furosemide; thiazides), hyperaldosteronism, renal tubular acidosis
• Transcellular shift (K moves into cells): alkalosis (every 0.1 rise in pH shifts K down by ~0.6 mmol/L), insulin therapy, beta-2 agonists (salbutamol)
• Inadequate intake: prolonged IV fluids without K supplementation
Hyperkalaemia (K > 5.5 mmol/L): The elevated extracellular K depolarises the cell membrane, initially making cells more excitable, then paradoxically blocking them (sustained depolarisation inactivates fast sodium channels). This produces the dangerous progressive ECG changes. Causes in children:
• Renal failure: most common cause — decreased renal K excretion
• Transcellular release (K shifts out of cells): acidosis (every 0.1 fall in pH raises K by ~0.6 mmol/L), haemolysis, rhabdomyolysis, tumour lysis syndrome
• Adrenal insufficiency (Addison's disease): loss of aldosterone → K retention
• Excessive IV potassium supplementation — iatrogenic, especially dangerous in neonates
• Pseudohyperkalaemia: haemolysis of blood sample, prolonged sample transit — always repeat if unexpected
SELF-CHECK
A child with acute gastroenteritis has serum K 2.9 mmol/L, and the ECG shows flattened T waves with prominent U waves. Which of the following mechanisms best explains the ECG finding?
A. Hyperpolarisation of the myocyte membrane reduces excitability
B. Depolarisation of the myocyte membrane increases excitability
C. Intracellular potassium decreases faster than extracellular potassium
D. Hypovolaemia directly alters myocyte conduction
Reveal Answer
Answer: A. Hyperpolarisation of the myocyte membrane reduces excitability
In hypokalaemia, the extracellular K falls while intracellular K remains relatively high. This widens the intra:extracellular K ratio, hyperpolarising the cell membrane (making it further from threshold). This reduces excitability and slows repolarisation, producing the characteristic flattened T wave and U wave on ECG. The cell becomes harder — not easier — to depolarise.