Page 5 of 30
PE20.2 | Acute Post Streptococcal Glomerulonephritis — SDL Guide (Part 2)
Management and Complications
Management of APSGN in children is fundamentally supportive, because the glomerular injury is immune-complex-mediated, self-limiting, and does not respond meaningfully to corticosteroids or immunosuppressants — a point that distinguishes APSGN sharply from steroid-responsive nephrotic syndrome (MCNS) and from crescentic GN. The clinician's role is therefore one of careful monitoring, prompt treatment of dangerous complications, and reassurance to families that recovery is expected in the great majority of cases. The four management priorities are: first, eradication of any residual GAS infection with a penicillin course; second, control of fluid overload and oedema with fluid restriction and diuretics; third, control of hypertension to prevent encephalopathy and cardiac failure; and fourth, identification of the small minority of children in whom oliguria progresses to acute renal failure requiring temporary dialysis. Antibiotics do not reverse or accelerate recovery from the glomerulonephritis itself — their purpose is to eliminate any remaining streptococcal organisms and reduce the risk of household transmission.
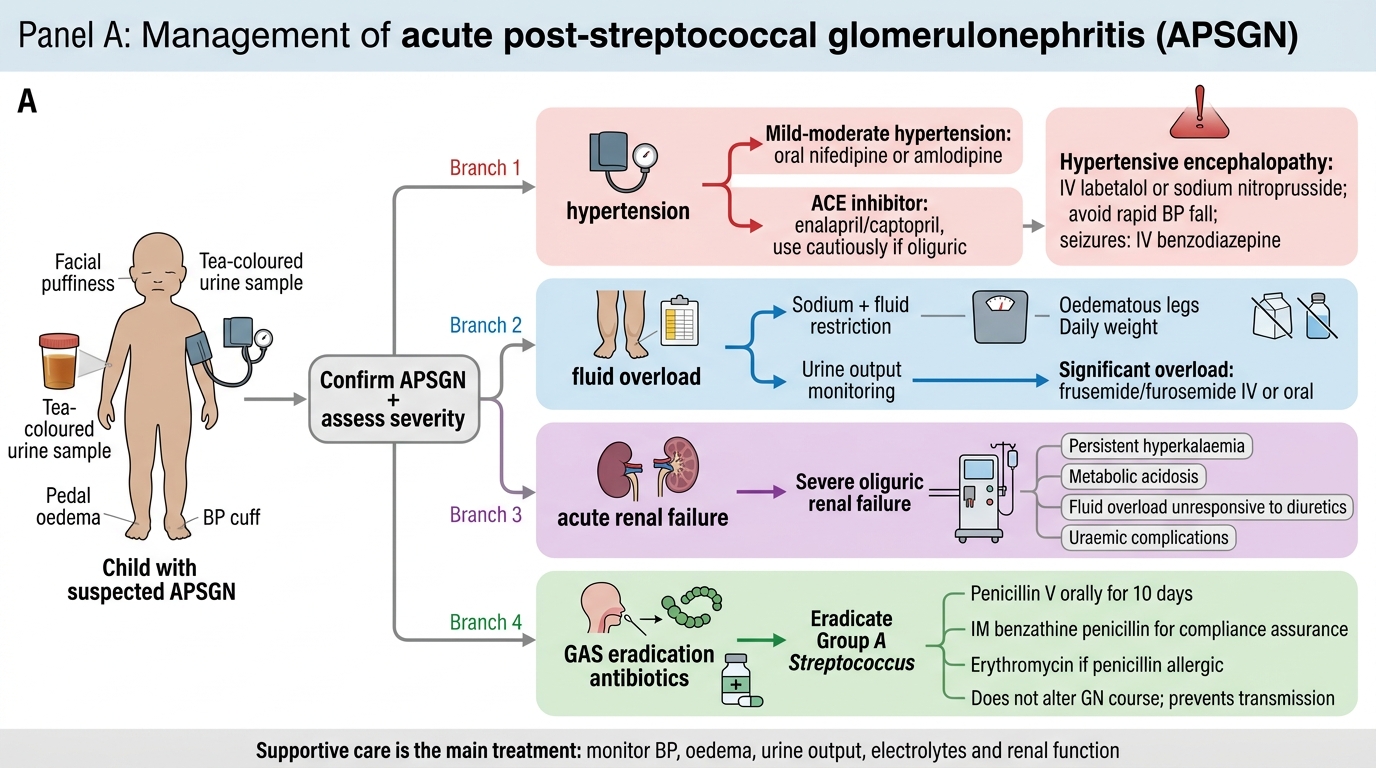
Management Flow Diagram for APSGN
Antibiotic therapy: a 10-day course of oral phenoxymethylpenicillin (penicillin V) or intramuscular benzathine penicillin (for compliance assurance) to eradicate GAS. Erythromycin is used in penicillin-allergic patients. This does NOT alter the course of GN but prevents ongoing streptococcal transmission.
Fluid and dietary management: sodium and fluid restriction commensurate with the degree of oedema and oliguria; daily weight and urine output monitoring. In patients with significant fluid overload, frusemide (furosemide) IV or oral accelerates diuresis and reduces oedema and hypertension.
Antihypertensive therapy:
• Mild-to-moderate hypertension: oral nifedipine (short-acting, for acute control) or amlodipine (for sustained control); ACE inhibitors (enalapril, captopril) reduce both BP and proteinuria but must be used cautiously in oliguric patients (risk of hyperkalaemia and worsening renal function).
• Hypertensive encephalopathy (severe hypertension + neurological symptoms): IV labetalol or sodium nitroprusside infusion for rapid controlled reduction; avoid precipitous drops. Seizures are managed with IV benzodiazepines.
Acute renal failure: if oliguric renal failure is severe (persistent hyperkalaemia, metabolic acidosis, fluid overload unresponsive to diuretics), peritoneal dialysis or haemodialysis may be required temporarily. Recovery is expected in most children.
Prognosis: >95% of children with sporadic APSGN recover completely with normal renal function. Microscopic haematuria may persist for up to 2 years without implying ongoing glomerulonephritis. Long-term CKD from APSGN in children is rare (<1% of sporadic cases), but epidemic forms (multiple cases from a single GAS strain) may have a slightly worse prognosis. Annual blood pressure and urinalysis follow-up is recommended for 1–2 years.
Self-Assessment
APSGN teaches several principles that recur across all of glomerular medicine: the latent period as an immunological timestamp, the complement pattern as a pathway indicator, the nephritic-nephrotic distinction as a management divider, and the expectation of self-limited recovery in most children. As you review the key themes below, pay particular attention to the facts that are most commonly tested and most commonly confused: the specific latent periods, the C3-low/C4-normal signature, the diagnostic role of anti-DNase B in pyoderma APSGN, and the indications for renal biopsy. Applying these correctly in a clinical scenario requires not just memorisation but pattern recognition — the ability to notice when a case deviates from the expected APSGN template and to ask whether a biopsy or alternative diagnosis is warranted.
- APSGN follows GAS pharyngitis (latent 1–2 weeks) or pyoderma (latent 3–6 weeks).
- Immune-complex deposition activates the alternative complement pathway: C3 LOW, C4 NORMAL.
- C3 must normalise within 6–8 weeks; persistence beyond 8–12 weeks mandates biopsy.
- Nephritic (not nephrotic) syndrome: haematuria + hypertension + oliguria + modest proteinuria.
- Dysmorphic RBCs and RBC casts on urine microscopy confirm glomerular origin.
- ASO elevated in post-pharyngitis APSGN; anti-DNase B is more sensitive for post-pyoderma APSGN.
- Management is supportive: penicillin to eradicate GAS, frusemide for fluid overload, antihypertensives for BP, dialysis if needed.
- Corticosteroids have no established role in typical APSGN.
- Prognosis is excellent in children: >95% recover completely.
SELF-CHECK
A 7-year-old girl presents with 'dark urine', periorbital puffiness, and a BP of 140/90 mmHg. She had impetigo on her lower leg 4 weeks ago. Which serological test is MOST likely to confirm streptococcal aetiology in this case?
A. ASO (anti-streptolysin O) titre
B. Anti-DNase B titre
C. ANCA (anti-neutrophil cytoplasmic antibody)
D. Anti-dsDNA antibody
Reveal Answer
Answer: B. Anti-DNase B titre
In post-impetigo/pyoderma APSGN, ASO titres are often normal or only marginally elevated, because streptolysin O activity is inhibited by skin lipids. Anti-DNase B is the more sensitive serological marker for post-skin streptococcal APSGN and should be the preferred test here. ANCA and anti-dsDNA are relevant to other GN (ANCA-vasculitis and lupus nephritis, respectively) and are not expected to be elevated in APSGN.