Page 14 of 30
PE20.5 | Acute Renal Failure — SDL Guide (Part 2)
Management
Management of paediatric AKI is structured around the underlying category, the degree of fluid and electrolyte disruption, and the presence of life-threatening complications. The first goal is always to identify and reverse any reversible cause while preventing further renal injury.
1. Prerenal AKI — fluid resuscitation:
A fluid challenge is both diagnostic and therapeutic. Give 10–20 mL/kg of isotonic saline (0.9% NaCl) or Ringer's lactate over 30–60 minutes. A brisk urine response (>1 mL/kg/h) within 2 hours confirms prerenal aetiology and mandates continued rehydration with ongoing loss replacement. Absence of response after 1–2 fluid boluses (total 20–40 mL/kg) implies intrinsic AKI, and further fluid loading risks pulmonary oedema — switch to strict fluid restriction.
2. Fluid management in established AKI (oliguric phase):
Once intrinsic AKI is diagnosed, fluid intake is restricted to insensible losses (~400 mL/m²/day in children) + measured urine output + ongoing losses. Daily weights guide the prescription — weight gain >0.5–1% per day indicates fluid overload. Avoid hypo-osmolar fluids (risk of hyponatraemia). During the diuretic/recovery phase, urine output increases dramatically — replace losses to prevent dehydration.
3. Hyperkalaemia — stepwise treatment:
Hyperkalaemia is the most immediately dangerous electrolyte complication of AKI and the leading cause of cardiac arrest. Management is staged by severity:
• Mild (K⁺ 5.5–6.5, no ECG changes): dietary restriction, calcium resonium (ion-exchange resin, 1 g/kg/dose orally or rectally) to increase GI potassium loss
• Moderate-severe (K⁺ >6.5 or ECG changes): emergency sequence:
1. Calcium gluconate 10%: 0.5–1 mL/kg IV over 5–10 minutes (cardioprotection; does not lower K⁺ — stabilises the myocardial membrane)
2. Sodium bicarbonate: 1–2 mEq/kg IV (drives K⁺ into cells; useful if acidosis is present)
3. Salbutamol (nebulised or IV): 2.5–5 mg nebulised (β₂ stimulation drives K⁺ intracellularly)
4. Glucose + insulin: 0.5 g/kg glucose + 0.1 unit/kg actrapid IV (transcellular shift; monitor blood glucose)
5. Dialysis: if K⁺ does not respond, continues to rise, or is >7 mEq/L
4. Nutrition and other supportive measures:
• Protein restriction (0.5–1 g/kg/day) to limit uraemia during the oliguric phase; avoid during the recovery phase.
• Treat hypertension with amlodipine, hydralazine, or labetolol depending on severity; hypertensive emergency (encephalopathy) requires IV agents.
• Treat anaemia conservatively in HUS (transfuse if Hb <7 g/dL, irrespective of platelet count, using washed packed red cells).
• Avoid nephrotoxic drugs (NSAIDs, aminoglycosides, contrast without pre-hydration).
• HUS-specific: supportive care only — no antibiotics, no steroids, no antithrombotic agents in typical D+HUS. Plasma exchange/eculizumab reserved for atypical HUS (complement-mediated).
5. Dialysis indications (AEIOU mnemonic):
• Acidosis: pH <7.1 unresponsive to bicarbonate
• Electrolytes: K⁺ >6.5–7 mEq/L refractory, or severe hyponatraemia
• Intoxication: dialysable poisons (salicylates, methanol, lithium)
• Overload: pulmonary oedema from fluid overload not responding to diuretics
• Uraemia: BUN >200 mg/dL, or uraemic encephalopathy/pericarditis
Modalities: peritoneal dialysis (PD) is most commonly used in young children and in resource-limited settings; haemodialysis for older children and rapid correction needs; continuous renal replacement therapy (CRRT) in haemodynamically unstable ICU patients.
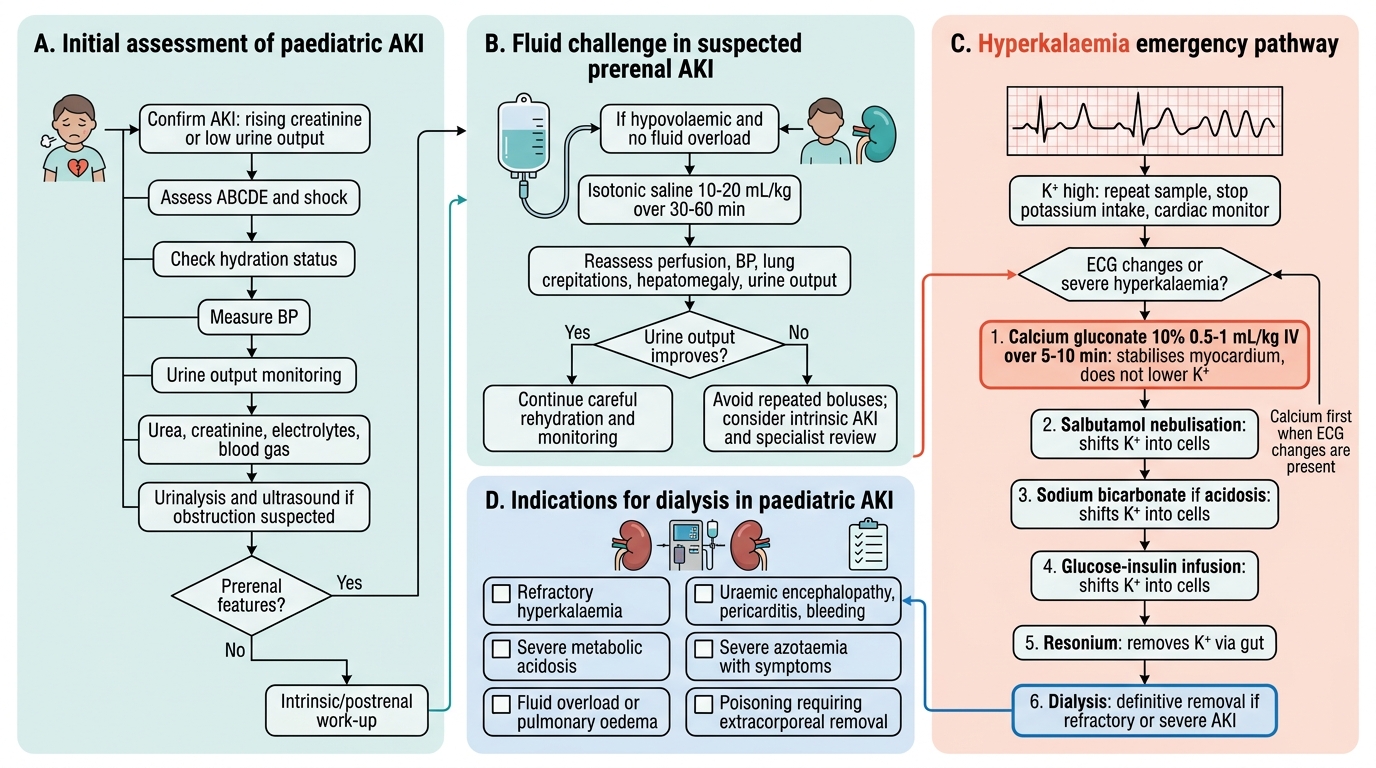
Paediatric AKI Management Algorithm
SELF-CHECK
A 3-year-old with HUS and AKI has potassium 7.2 mEq/L with peaked T waves on ECG. What is the FIRST drug to administer?
A. Sodium bicarbonate 2 mEq/kg IV to correct metabolic acidosis and shift K⁺ intracellularly
B. Calcium gluconate 10% (0.5–1 mL/kg IV over 5–10 minutes) to stabilise the myocardium
C. Salbutamol nebulisation (2.5 mg) to drive potassium into cells via β₂ stimulation
D. Glucose-insulin infusion (0.5 g/kg glucose + 0.1 unit/kg actrapid) to lower serum potassium
Reveal Answer
Answer: B. Calcium gluconate 10% (0.5–1 mL/kg IV over 5–10 minutes) to stabilise the myocardium
When ECG changes (peaked T waves, or worse — wide QRS, sine-wave) are present with hyperkalaemia, the immediate priority is cardiac membrane stabilisation with calcium gluconate. Calcium gluconate does NOT lower serum potassium — it stabilises the cardiac myocyte membrane threshold, preventing arrhythmia while the subsequent measures (bicarbonate, salbutamol, glucose-insulin, resonium) actually lower potassium levels. The sequence must be: calcium first (cardioprotect) → bicarbonate/salbutamol/glucose-insulin (transcellular shift) → resonium/dialysis (removal).
Complications and Prognosis
Paediatric AKI, if inadequately managed, carries a spectrum of life-threatening short-term complications and significant risk of long-term renal sequelae. The complications arise directly from the two fundamental derangements of AKI — failure to excrete potassium and acid (causing hyperkalaemia and metabolic acidosis) and failure to regulate fluid balance (causing fluid overload). Superimposed on these are uraemic toxin accumulation, hypertension from volume expansion, and haematological dysfunction. Understanding the mechanistic basis of each complication allows the clinician to anticipate its emergence and intervene before it becomes irreversible. Long-term consequences of AKI in childhood are increasingly recognised: even a single episode of AKI sufficient to require hospitalisation is an independent risk factor for chronic kidney disease, hypertension, and proteinuria in later life.
Provided image
Short-term complications:
- Hyperkalaemia: the most immediately life-threatening complication; risk of fatal ventricular arrhythmia
- Hypertensive emergencies: encephalopathy with seizures, intracranial haemorrhage — more common in children than adults with AKI due to the rapidity of blood pressure rise
- Fluid overload and pulmonary oedema: especially if fluids are continued without recognising the transition from prerenal to intrinsic AKI
- Metabolic acidosis: bicarbonate is lost via impaired tubular reabsorption and H⁺ cannot be excreted; respiratory compensation (Kussmaul breathing) may develop
- Hyponatraemia: dilutional, from inappropriate fluid administration
- Uraemia: encephalopathy (confusion, seizures), uraemic pericarditis (friction rub), bleeding (platelet dysfunction)
- Anaemia: from impaired erythropoiesis, haemolysis (HUS), and haemodilution
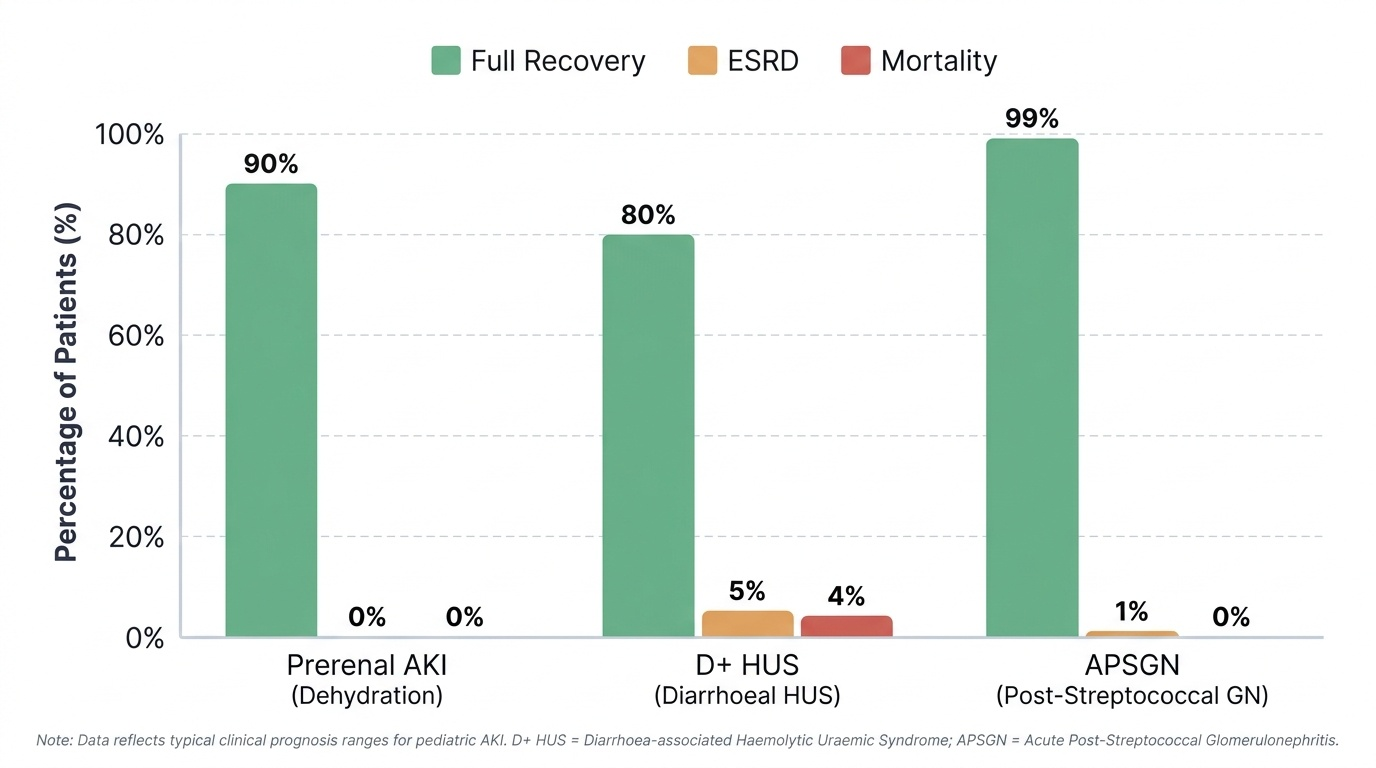
Prognosis:
The prognosis of AKI in children depends critically on the underlying aetiology:
• Prerenal AKI from dehydration: full recovery in >90% with prompt rehydration; risk of permanent damage if ATN supervenes
• HUS (D+HUS): ~80% full recovery with supportive care; ~5% end-stage renal disease (ESRD); ~3–5% mortality; neurological complications (seizures, stroke) in ~20%; atypical HUS (complement-mediated) carries 50% ESRD risk
• APSGN: excellent prognosis in children; <1% progress to ESRD; complete recovery within 4–6 weeks in most
• Bilateral cortical necrosis (prolonged severe hypoperfusion): poor prognosis, often leads to CKD
Long-term follow-up is mandatory for all children with significant AKI: annual BP measurement, urinalysis, and GFR estimation for at least 5 years, as AKI is a recognised risk factor for CKD (see PE20.6).
Self-Assessment: AKI in Children
Before attempting the assessments for this cluster, take a few minutes to work through each of the following reflective prompts without referring to your notes. Self-testing through active retrieval practice at this stage substantially strengthens long-term retention compared to passive re-reading, and the evidence from cognitive science consistently shows that the effort of recalling information — even when partially unsuccessful — produces stronger memory consolidation than re-exposure to the material. These prompts target the high-yield concepts that are most commonly examined and most clinically dangerous if forgotten. For each question, try to generate your answer in full sentences, including the underlying mechanism — not just the correct label. If you find a gap, revisit the relevant content block before proceeding.
- Can you classify the following into prerenal/intrinsic/postrenal and name the mechanism: acute gastroenteritis with dehydration; D+HUS; aminoglycoside toxicity; posterior urethral valves; APSGN?
- Recite the KDIGO Stage 1, 2, and 3 creatinine criteria. Why does a paediatric creatinine of 1.2 mg/dL demand attention even though it is 'in the normal adult range'?
- A child with suspected HUS has K⁺ 6.8 mEq/L, peaked T waves, and Hb 6.5 g/dL. Walk through your immediate management sequence step by step, including your decision about antibiotics.
- What are the five AEIOU dialysis indications? Which would apply first in a child with pulmonary oedema from fluid overload?
- Why does prerenal AKI show FENa <1% while ATN shows FENa >2%? What is the tubular mechanism?
- What long-term complication must you counsel the family about after a child survives a significant AKI episode?
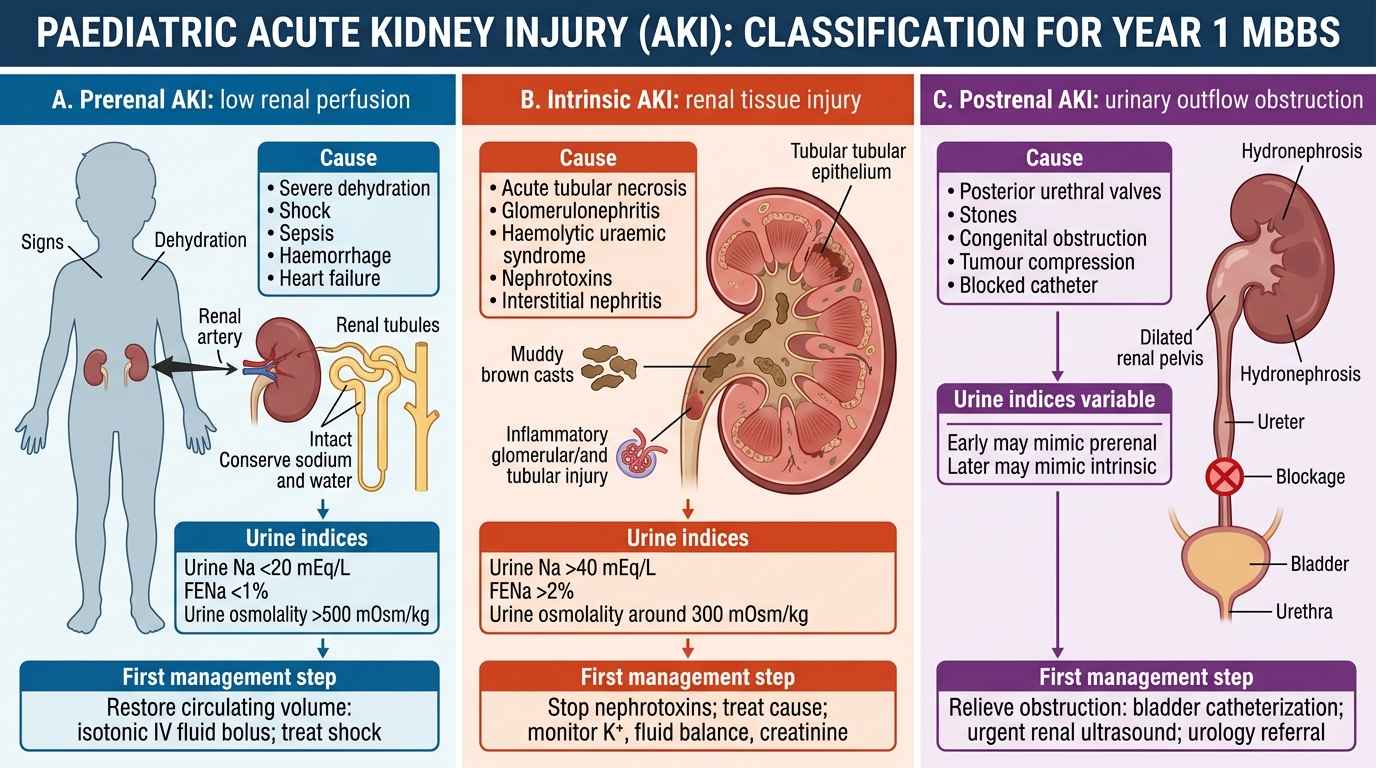
Paediatric AKI Classification: Causes, Urine Indices, and First Management
SELF-CHECK
Which urine index pattern is MOST consistent with prerenal AKI from severe dehydration in a 2-year-old?
A. Urine sodium 60 mEq/L, FENa 3.5%, urine osmolality 280 mOsm/kg
B. Urine sodium 12 mEq/L, FENa 0.5%, urine osmolality 650 mOsm/kg
C. Urine sodium 55 mEq/L, FENa 4.2%, urine osmolality 320 mOsm/kg
D. Urine sodium 45 mEq/L, FENa 2.8%, urine osmolality 290 mOsm/kg
Reveal Answer
Answer: B. Urine sodium 12 mEq/L, FENa 0.5%, urine osmolality 650 mOsm/kg
In prerenal AKI, the tubules are structurally intact and respond to reduced perfusion by maximally conserving sodium (urine Na <20 mEq/L, FENa <1%) and water (concentrated urine, osmolality >500 mOsm/kg). Option B shows urine Na 12, FENa 0.5%, and high osmolality 650 — the hallmark of prerenal physiology. Options A, C, and D all show high urine sodium and FENa >2%, which indicate tubular injury (intrinsic AKI, ATN), where the concentrating and sodium-conserving mechanisms are disrupted.