Page 23 of 30
PE20.8-9 | Urine and KUB Interpretation — SDL Guide (Part 2)
Interpretation of Urinalysis Findings
Systematic interpretation of urinalysis proceeds through three sequential and complementary layers — physical examination of the urine, dipstick chemical analysis, and urine microscopy — each adding information that the others cannot provide independently. The clinical value of urinalysis lies in integrating all three layers to reach a coherent diagnostic conclusion rather than interpreting individual analytes in isolation; a single positive dipstick analyte is often non-specific, but a consistent pattern across all three layers is highly diagnostic. The most specific and diagnostically powerful element of urinalysis is urine microscopy, particularly the identification and classification of urinary casts, which provides direct anatomical information about the precise nephron segment that is injured and the nature of that injury.
Physical examination of the urine:
- Colour: pale yellow = normal (dilute); dark yellow/amber = concentrated; red/pink = haematuria (haemoglobin) or myoglobinuria; cola/brown = haemoglobin (haemolysis), myoglobin (rhabdomyolysis), or bilirubin (obstructive jaundice); turbid/cloudy = pyuria, phosphaturia (benign after meals), or bacteriuria
- Specific gravity: 1.001–1.030; fixed at ~1.010 (isosthenuria) in advanced CKD (loss of concentrating and diluting ability); specific gravity >1.025 suggests adequate tubular function
- Odour: sweet/fruity = ketonuria (DKA, starvation); ammoniacal = old specimen or urea-splitting organisms (Proteus UTI)
Dipstick interpretation:
Dipstick chemistry is the first step in chemical screening and guides selection of microscopy targets. Each analyte should be read and documented before interpreting the whole picture:
- Protein (albumin): 1+ ≈ 30 mg/dL; 3+ ≈ >300 mg/dL; massive proteinuria (3+/4+) + hypoalbuminaemia = nephrotic syndrome; 1+/2+ + haematuria = nephritic syndrome; orthostatic proteinuria (benign, disappears supine) = common in school-age children and adolescents
- Blood: positive = haemoglobin (haemolysed RBCs from any cause), intact RBCs, or myoglobin; dipstick CANNOT distinguish haematuria from myoglobinuria — microscopy is required
- Leucocyte esterase: positive = pyuria (WBCs ≥5/HPF); combined positive leucocyte esterase + positive nitrite has >90% PPV for UTI
- Nitrites: positive = gram-negative bacteria (reduce dietary nitrates to nitrite); false negative = gram-positive UTI (Enterococcus), low dietary nitrate, high urine flow
- Glucose: in the absence of hyperglycaemia, glucosuria suggests proximal tubular dysfunction (Fanconi syndrome: also phosphaturia, aminoaciduria, uricosuria, RTA)
- Ketones: ketonuria in children is common with fasting, vomiting, febrile illness; marked ketonuria with glucosuria = DKA
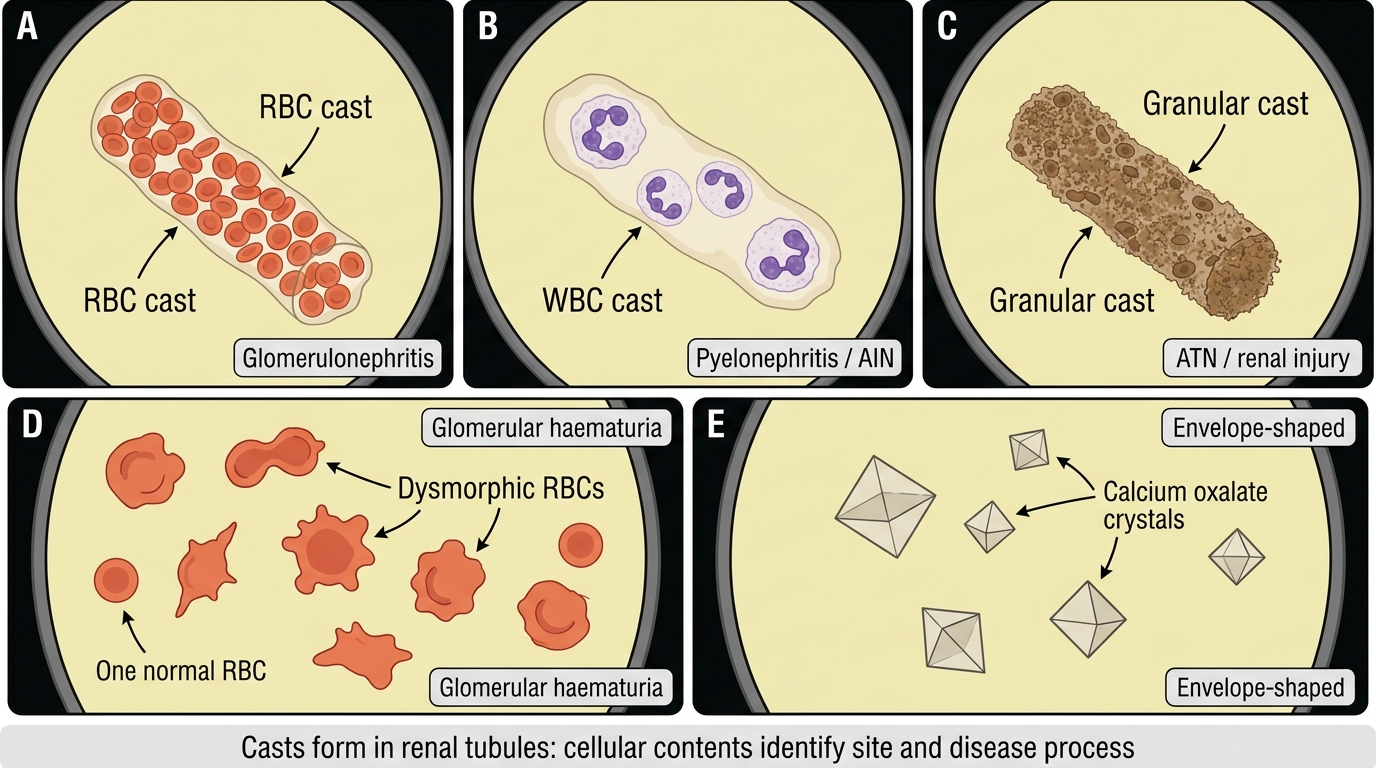
Urine Microscopy: Casts, Dysmorphic RBCs, and Calcium Oxalate Crystals
Cast interpretation — the most specific urinalysis finding:
| Cast type | Composition | Clinical significance |
|---|---|---|
| Hyaline | Pure Tamm-Horsfall protein | Benign; dehydration, fever, post-exercise — not pathological |
| RBC (red cell) | Red blood cells in protein matrix | Pathognomonic of glomerulonephritis (APSGN, IgA nephropathy, RPGN, lupus nephritis) |
| WBC (white cell) | Leucocytes in protein matrix | Pyelonephritis or acute interstitial nephritis |
| Granular | Degenerated cellular debris | Non-specific; seen in ATN, CKD, or any significant renal injury |
| Waxy | Highly refractile, brittle | Advanced/chronic renal disease; renal tubular stasis |
| Fatty | Fat droplets (cholesterol) | Nephrotic syndrome (lipiduria) |
| Broad | Very wide; collecting duct origin | Severe chronic renal failure |
Crystals: calcium oxalate = dihydrate (envelope/square, most common), monohydrate (dumbbell); uric acid = yellow-brown rhomboid (acidic urine); struvite = triple phosphate (coffin-lid shape; alkaline urine, Proteus UTI); cystine = hexagonal plates (cystinuria).
CLINICAL PEARL
Dipstick blood positive + microscopy no RBCs = myoglobinuria, not haematuria. The dipstick blood analyte detects haem pigment — which includes both intact RBC haemoglobin and free myoglobin. When dipstick blood is strongly positive but microscopy shows few or no red blood cells, the discordance points to myoglobinuria (rhabdomyolysis — muscle injury, viral myositis, extreme exercise) or haemoglobinuria (haemolytic anaemia, HUS, transfusion reaction). The clinical importance is significant: myoglobinuria causes AKI by direct tubular toxicity, and management (aggressive IV hydration to dilute myoglobin) is entirely different from haematuria. Always perform microscopy whenever dipstick blood is positive — never accept the dipstick alone.
Interpretation of Plain X-Ray KUB
Systematic reading of a plain X-ray KUB requires a disciplined, structured approach that covers every anatomical region of interest in a fixed and reproducible order to avoid missing incidental findings that fall outside the clinician's preformed hypothesis. The most common error in plain film interpretation — in examinations and in clinical practice equally — is looking only at the area suggested by the clinical question and missing a second or third abnormality that changes the management completely. The standard approach uses a systematic sequential review of the film through defined anatomical areas, documented in a fixed mnemonic sequence, so that the process becomes automatic over time. The student who develops and habitually applies such a sequence will interpret KUB films reliably and accurately regardless of which specific abnormality is present.
Provided image
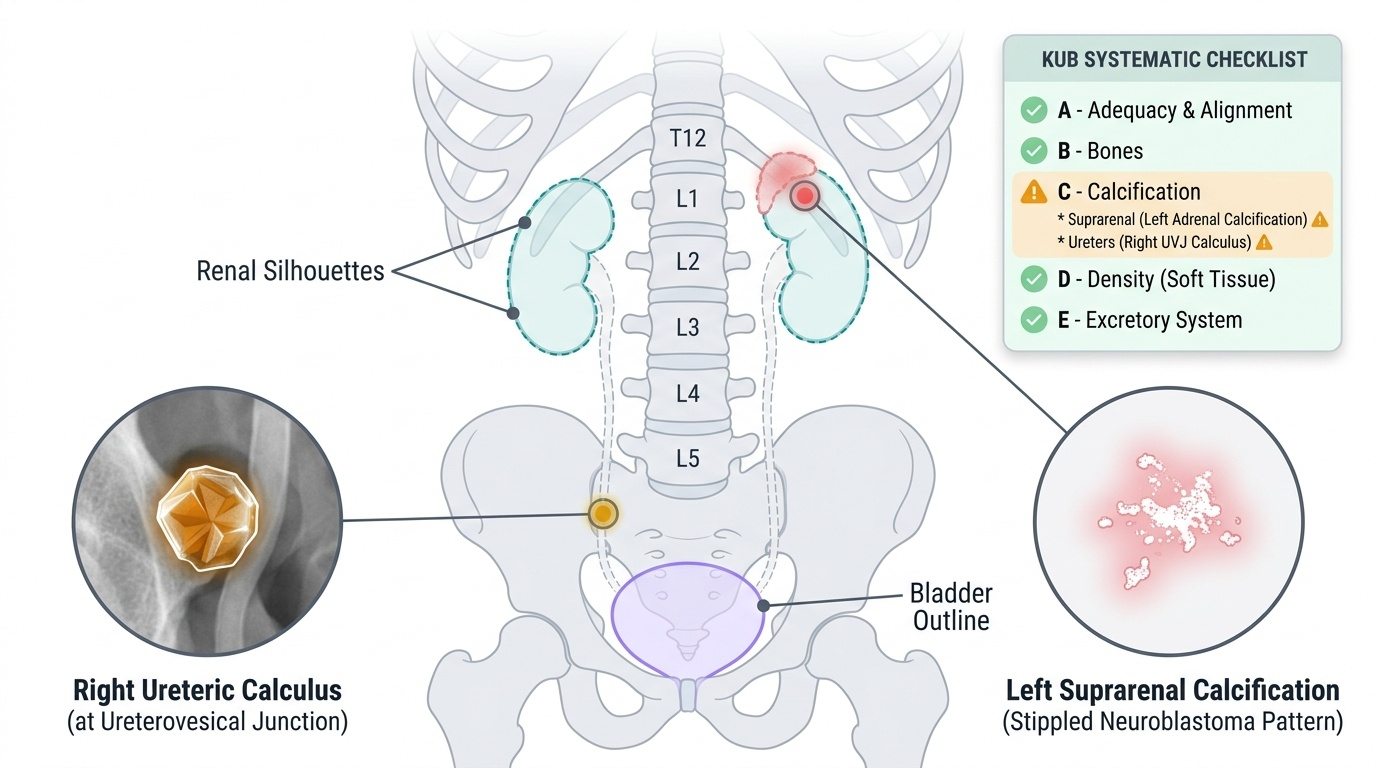
Systematic approach to reading a KUB (ABCDE framework adapted for urinary tract):
- Adequacy and alignment: check that both renal areas, both ureters, and the full bladder region are included; assess spinal alignment (scoliosis may indicate underlying renal/vertebral anomaly)
- Bones: examine vertebrae and ribs for fractures, sclerotic/lytic lesions, or spina bifida (associated with neurogenic bladder)
3. Calcification — the key KUB finding:
The single most important purpose of a paediatric KUB is to detect and localise calcification. Ask systematically: is there calcification at (a) the renal poles — intrarenal calculi, medullary nephrocalcinosis (hyperparathyroidism, RTA, hyperoxaluria)? (b) the course of the ureters — ureteric calculi, typically at three sites of physiological narrowing: pelvi-ureteric junction, crossing the iliac vessels, ureterovesical junction? (c) the bladder — bladder calculi (visible as opacities overlying the pelvis)? (d) the suprarenal region — adrenal calcification (neuroblastoma = stippled/amorphous; ~85% of neuroblastomas calcify; Wilms = very rare, faint)?
- Density (soft tissue outlines): assess the renal silhouettes — are they visible, the correct size (~width of L2–L3 vertebrae in young children), bilaterally symmetrical? Loss of the psoas shadow suggests retroperitoneal pathology (abscess, haematoma). A large soft-tissue mass displacing bowel loops may represent a renal tumour (Wilms) or suprarenal mass (neuroblastoma).
- Excretory structures and gas patterns: check the bowel gas distribution for obstruction or displacement; a distended bladder suggests outflow obstruction (PUV, neurogenic bladder); absent bowel gas shadow in the pelvis may indicate a large pelvic/bladder mass.
Radio-opacity of common urinary calculi:
Calcium oxalate (most common in children) and calcium phosphate are radio-opaque (white on film). Struvite (staghorn, associated with Proteus UTI) is radio-opaque and fills the pelvicalyceal system. Cystine calculi are faintly opaque. Uric acid calculi are radiolucent — they are completely invisible on plain film; CT urogram is required for diagnosis. This distinction is clinically important: a child with suspected renal colic and a negative KUB may still have calculus disease (uric acid or small calcium calculi <3 mm).
SELF-CHECK
A 5-year-old boy with frank haematuria has urinalysis showing 3+ blood on dipstick, numerous RBCs on microscopy, and RBC casts. Which diagnosis is MOST consistent and what is the pathophysiological basis of the RBC casts?
A. Urinary tract infection — RBC casts form when bacteria lyse RBCs that enter the bladder during infection
B. Glomerulonephritis — RBC casts form when RBCs leak through the damaged glomerular filtration barrier into the tubular lumen and become enmeshed in Tamm-Horsfall protein
C. Renal calculus — RBC casts form from RBCs shed from the urothelial surface damaged by the calculus
D. Wilms tumor — RBC casts form from tumour cells invading the collecting system
Reveal Answer
Answer: B. Glomerulonephritis — RBC casts form when RBCs leak through the damaged glomerular filtration barrier into the tubular lumen and become enmeshed in Tamm-Horsfall protein
RBC casts are pathognomonic of glomerulonephritis. The mechanism is: (1) damaged glomerular filtration barrier allows RBCs to pass into the tubular lumen; (2) in the distal tubule and collecting duct, the RBCs become enmeshed in a Tamm-Horsfall protein gel (formed under conditions of low flow, high protein, and acid pH) to create an RBC cast. RBC casts cannot form from non-glomerular haematuria (UTI, calculus, tumour) because those RBCs are isomorphic and enter the urinary collecting system below the nephron, where cast formation does not occur. The presence of an RBC cast mandates urgent glomerulonephritis workup — ASOT, complement, anti-dsDNA/ANA, renal biopsy if atypical.
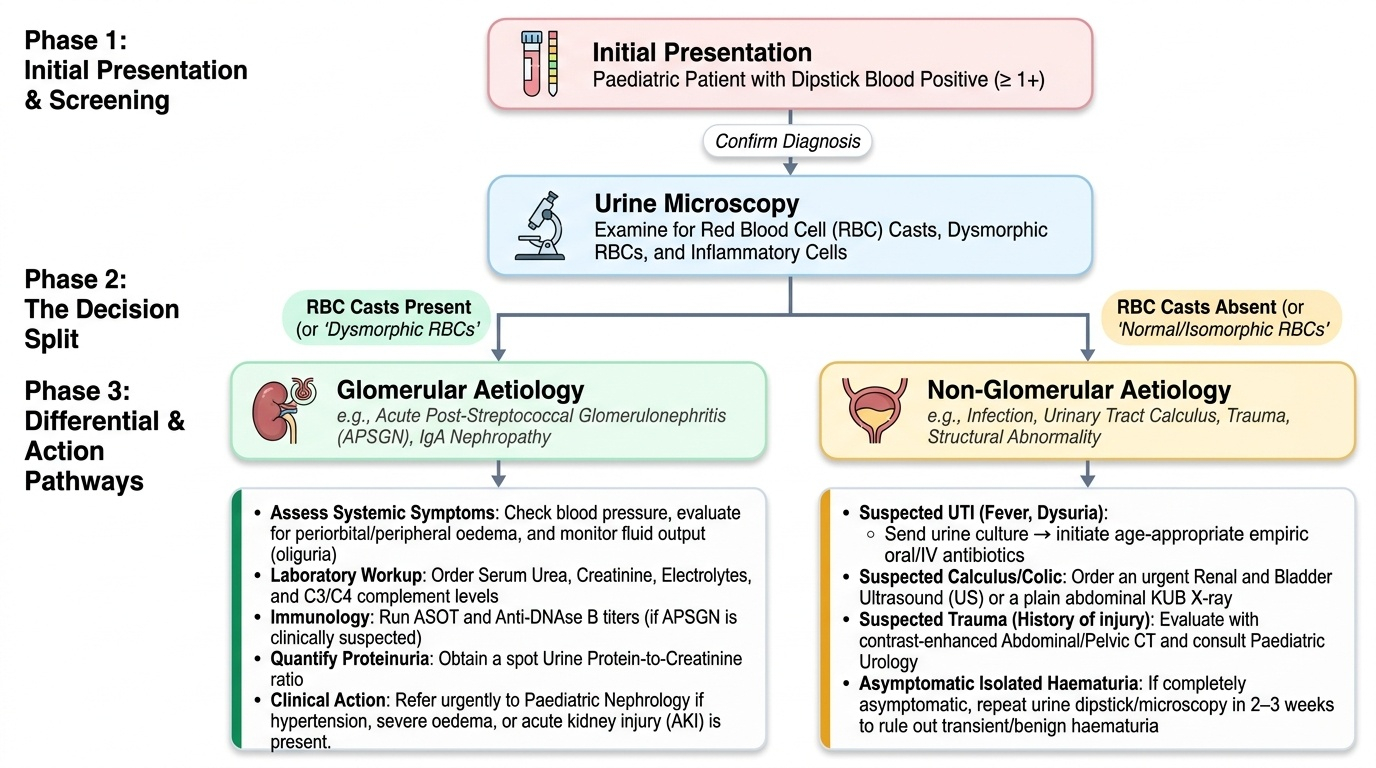
Applied Practice: Clinical Integration
The real clinical value of urinalysis and KUB emerges not from interpreting the tests in isolation but from integrating their findings into specific paediatric renal and urological clinical presentations. This integrative step — from test result to differential diagnosis to clinical action — is the core skill that distinguishes a clinician who has memorised normal ranges from one who can act at the bedside. Working through representative case patterns in this structured format consolidates both the interpretation skills developed in the previous sections and the clinical reasoning required to select the correct next investigation or treatment. The five patterns below are chosen to cover the most commonly examined clinical scenarios in final-year paediatric written examinations and OSCEs, as well as the most common presentations you will encounter in clinical postings.
Provided image
Pattern 1 — UTI in a toddler: Dipstick: leucocyte esterase 2+, nitrite positive, trace protein. Microscopy: 15–20 WBCs/HPF, bacteriuria, no casts. Interpretation: bacterial UTI (gram-negative, as nitrite positive). Action: confirm by SPA/catheter in infants; prescribe age-appropriate antibiotics after urine culture sent; renal ultrasound for first UTI in a child <2 years.
Pattern 2 — Post-streptococcal glomerulonephritis (APSGN): Dipstick: 3+ blood, 2+ protein. Microscopy: numerous dysmorphic RBCs, RBC casts. KUB: normal. Interpretation: glomerulonephritis — RBC casts are pathognomonic. Action: ASOT, throat swab, complement C3 (low in APSGN), renal function, BP. Manage fluid restriction, antihypertensives; penicillin if active streptococcal infection.
Pattern 3 — Nephrotic syndrome: Dipstick: 3+/4+ protein, trace blood, glucose negative. Microscopy: fatty casts (lipiduria), oval fat bodies, no RBC casts. KUB: normal. Interpretation: heavy proteinuria (nephrotic range). Action: 24-hour protein or UPCR, albumin, lipid profile, renal function. Commence prednisolone if first episode of childhood nephrotic syndrome.
Pattern 4 — Renal colic / ureteric calculus: Dipstick: 1+–2+ blood. Microscopy: RBCs (isomorphic), no casts. KUB: radio-opaque density along the right ureter at the level of the pelvis. Interpretation: calcium oxalate or phosphate calculus at the ureterovesical junction. Action: renal-ureteric ultrasound (first line in children) or CT urogram for full stone characterisation; analgesia, hydration; urological referral if stone >5 mm.
Pattern 5 — Adrenal mass with calcification on KUB: Dipstick: normal. Microscopy: normal. KUB: amorphous stippled calcification in the left suprarenal region. Interpretation: adrenal calcification in this clinical context (toddler with abdominal mass) is neuroblastoma until proven otherwise — Wilms rarely calcifies, and adrenal calcification is not normal. Action: ultrasound first, CT for staging; urine VMA/HVA; paediatric oncology referral.