Page 7 of 20
PE21.3 | Kawasaki Disease — SDL Guide
Learning Objectives
- Describe the clinical features and diagnostic criteria of Kawasaki disease including the CREAM mnemonic and the concept of incomplete Kawasaki disease
- Explain the pathophysiology of medium-vessel vasculitis and the mechanism of coronary artery aneurysm formation in Kawasaki disease
- Apply the AHA 2017 diagnostic algorithm including supplemental laboratory and echocardiographic criteria for incomplete Kawasaki disease
- Outline the evidence-based management of Kawasaki disease: IVIG 2 g/kg within 10 days, aspirin phases, and management of IVIG resistance
- Describe the echocardiographic monitoring schedule and long-term coronary artery surveillance based on aneurysm classification
INSTRUCTIONS
Kawasaki disease is the leading cause of acquired heart disease in children in developed countries, and its prevalence is rising in India. It is a clinical diagnosis made at the bedside — no single laboratory test is diagnostic. The danger is entirely in the coronary arteries: a child who is treated with IVIG within 10 days has a less than 5% chance of developing a coronary aneurysm; a child who is missed or treated late has a 15–25% risk. The clinical features look deceptively like a viral fever, and the window of opportunity to prevent permanent cardiac damage is just 10 days. This module builds the clinical vigilance to recognise Kawasaki disease early and act within that window.
References
- Ghai Essential Pediatrics, 9th Ed, Ch 17 — Kawasaki Disease (textbook)
- Nelson Textbook of Pediatrics, 21st Ed, Ch 184 — Kawasaki Disease (textbook)
- AHA/AAP Scientific Statement on Kawasaki Disease Diagnosis, Treatment, and Long-Term Management, 2017 (guideline)
- IAP Subspecialty Chapter of Pediatric Cardiology — Kawasaki Disease Guidelines (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 3-year-old boy has had fever for 6 days. His parents took him to three different clinics and were told it was a viral fever each time. Today he is brought to you and you notice his eyes are red, his lips are cracked and bright red, and he has a lumpy, tender swelling on the left side of his neck. Yesterday his hands were 'puffy' and red. He has no runny nose and no cough. His CRP is 142 mg/L, ESR 88 mm/hr, WBC 19,400/µL, and platelet count is 489,000/µL. He has been febrile for 6 days. You realise this is not a viral fever — but it may still be within the 10-day treatment window. Every day of delay is a day the coronary arteries are exposed to inflammation. What is your next step?
WHY THIS MATTERS
Kawasaki disease is the leading cause of acquired heart disease in children under 5 years in Japan, the USA, and increasingly in India. In India, the incidence is rising — estimated at 8–80 per 100,000 children under 5 years in various regional studies, though it is likely underdiagnosed. The disease is entirely benign in the skin, joints, and mucous membranes — all those features resolve without permanent damage. The only lesion that matters long-term is the coronary artery aneurysm (CAA): it predisposes to coronary thrombosis, myocardial infarction, and sudden death — even in young adults who had Kawasaki disease in childhood. The treatment window is 10 days from fever onset. Miss it, and the outcome is determined by the extent of coronary damage that has already occurred. Every febrile child under 5 with prolonged fever deserves a Kawasaki screen.
RECALL
Before proceeding, recall from Anatomy: the coronary arteries — left main coronary artery dividing into left anterior descending (LAD) and circumflex (LCx), and the right coronary artery (RCA). Recall that the coronary arteries are medium-calibre muscular arteries with well-developed tunica media. Recall from Physiology: the inflammatory cascade — how cytokines (TNF-α, IL-1, IL-6) activate endothelial cells and recruit neutrophils; the concept of matrix metalloproteinases (MMPs) in extracellular matrix degradation. Recall from pathology: the classification of vasculitides by vessel size — small-vessel (HSP, ANCA-associated), medium-vessel (Kawasaki, polyarteritis nodosa), large-vessel (Takayasu). Kawasaki is the prototype medium-vessel vasculitis of childhood.
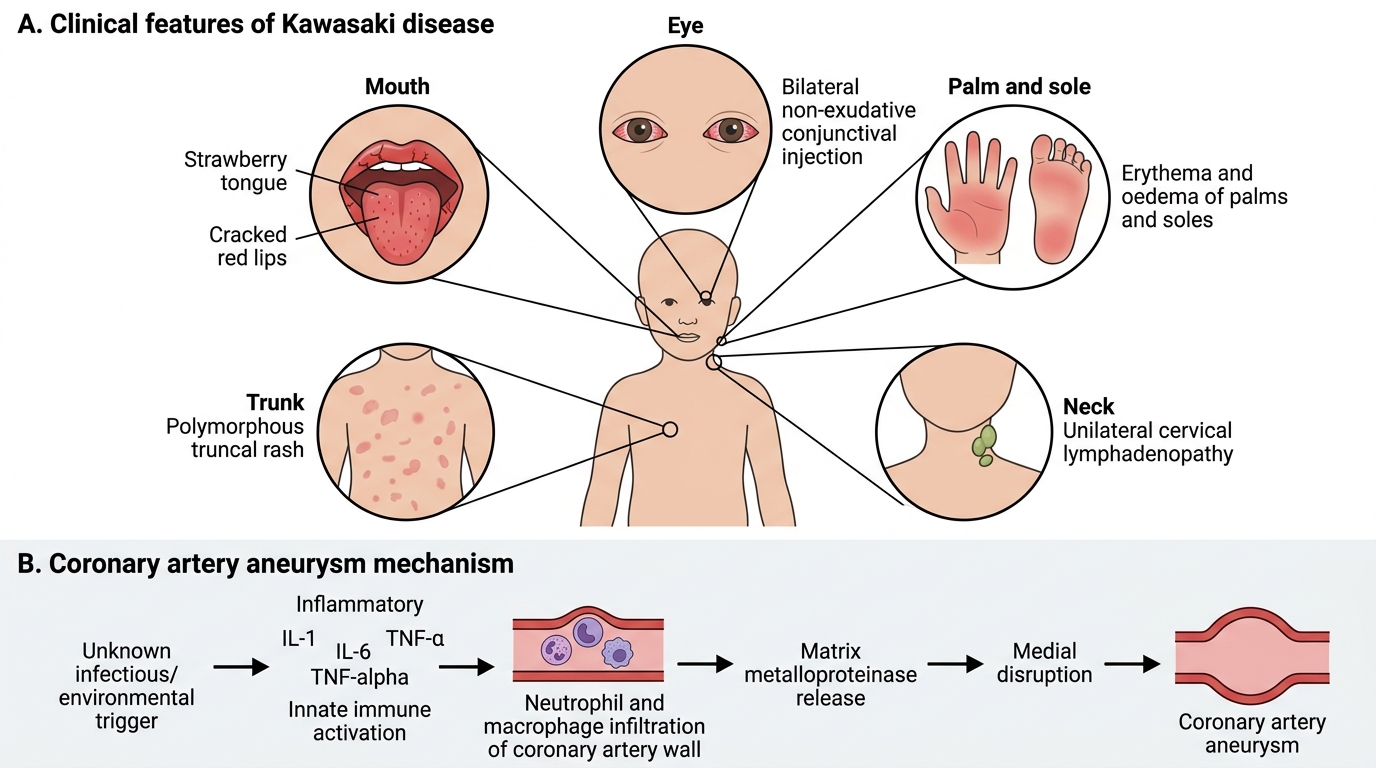
Clinical Presentation of Kawasaki Disease
Kawasaki disease presents as an acute febrile illness in young children, typically under 5 years, with a peak incidence at 12–24 months. The diagnosis is clinical and based on a characteristic constellation of features that have been given the mnemonic CREAM: Conjunctivitis, Rash, Extremity changes, Adenopathy, and Mucositis. The fever is the anchor criterion — it must be present for at least 5 consecutive days (or for any duration if all 5 other features are present simultaneously and the diagnosis is clinically certain).
The CREAM criteria in detail:
(C) Conjunctivitis: Bilateral, non-exudative (no discharge, no crusting) conjunctival injection — bulbar conjunctiva, sparing the limbus. This distinguishes it from bacterial conjunctivitis (which is exudative) and from the conjunctivitis of adenovirus (which is often exudative and associated with pharyngitis).
(R) Rash: Polymorphous (variable morphology — maculopapular, morbilliform, or erythroderma), truncal and perineal distribution. The perineal rash (erythema and early desquamation of the perineum/perianal area) is an early and diagnostically useful feature, easily missed if the nappy is not removed.
(E) Extremity changes — biphasic: Acute phase (days 1–14): erythema and indurated oedema of the palms and soles, causing the child to refuse to bear weight or use the hands. Subacute phase (day 14–28): periungual desquamation — peeling of the skin beginning at the fingertips and toes, starting at the nail margins. Desquamation may be the first feature noticed by parents after the fever resolves.
(A) Adenopathy: Unilateral cervical lymphadenopathy — at least one node ≥1.5 cm in diameter. This is the least commonly present criterion (~50% of cases). It is characteristically tender and firm, causing neck stiffness and sometimes leading to an initial diagnosis of bacterial lymphadenitis.
(M) Mucositis: Oral mucous membrane changes — strawberry tongue (prominent red papillae after white coating desquamates), cracked, fissured, and bright-red lips, and diffuse erythema of the oropharynx without exudate or ulceration.
Complete Kawasaki disease: fever ≥5 days + ≥4 of 5 CREAM criteria.
Incomplete Kawasaki disease: fever ≥5 days + 2 or 3 CREAM criteria, with laboratory or echocardiographic evidence (AHA 2017 algorithm). Incomplete Kawasaki is commoner in infants under 6 months and older children, and carries the SAME risk of coronary artery aneurysm as complete Kawasaki — hence it must not be dismissed.
Disease phases: Acute (day 1–14, fever + mucocutaneous features), subacute (day 14–28, periungual desquamation, thrombocytosis peaks, highest CAA risk if untreated), convalescent (day 28–60, normalisation of inflammatory markers, persisting CAA).
Kawasaki Disease: Clinical Features and Coronary Aneurysm Pathogenesis
Pathophysiology and Aetiology
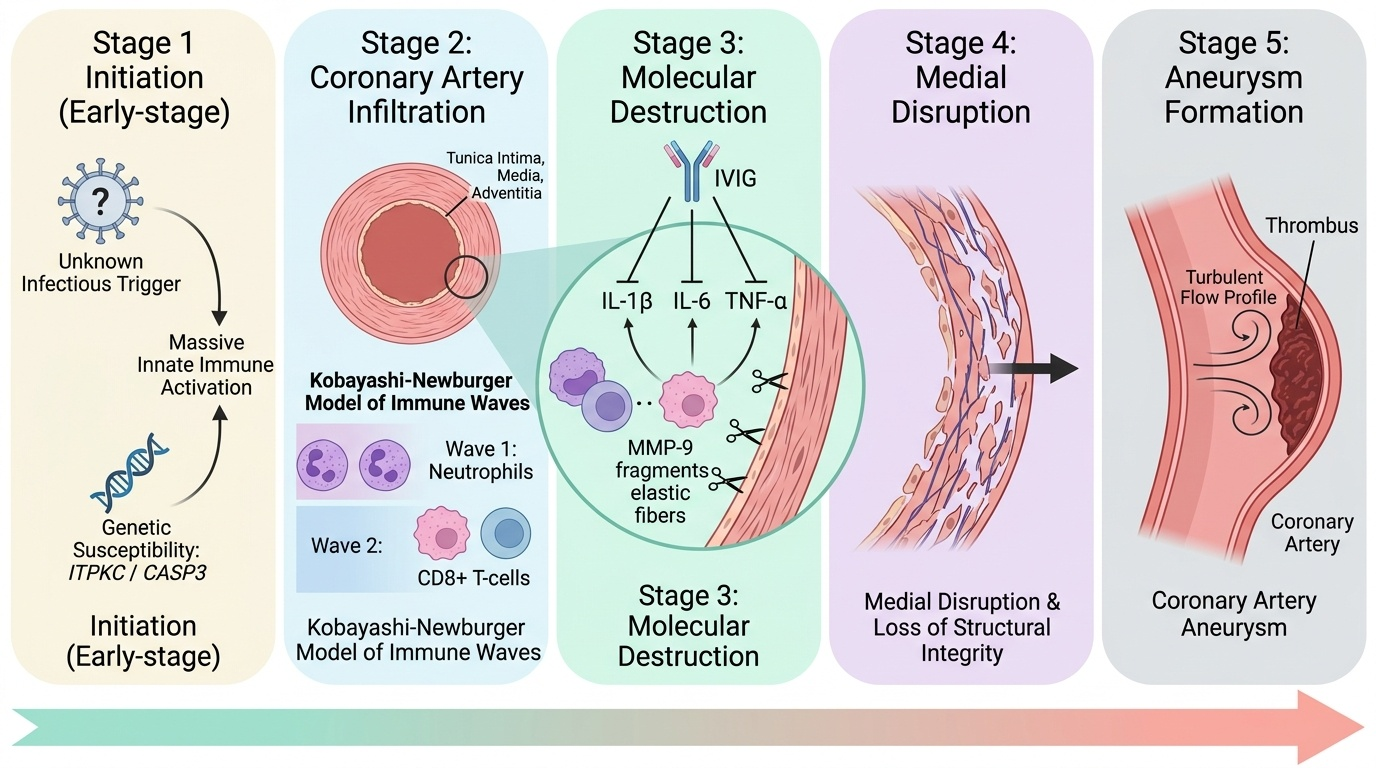
The aetiology of Kawasaki disease remains unknown despite 50 years of investigation. The leading hypothesis is that an unidentified infectious trigger (possibly a seasonal respiratory virus, a superantigen, or a novel RNA virus) drives massive innate immune activation in genetically susceptible children, predominantly those of East Asian ancestry but increasingly recognised in Indian and South Asian children.
Provided image
Genetic susceptibility is established: ITPKC and CASP3 polymorphisms (both involved in T-cell activation and apoptosis regulation) are associated with Kawasaki disease and coronary aneurysm risk in genome-wide association studies in Japanese and Asian-American populations. The seasonal clustering (winter-spring peaks) and geographic waves suggest an infectious or environmental trigger propagating through susceptible populations.
The immunopathology of the vasculitic phase involves a dramatic shift from innate to adaptive immune activation. An initial neutrophil-dominant infiltration of the coronary artery adventitia and media occurs within days of fever onset. This is followed by macrophage, CD8+ T-cell, and plasma cell infiltration — the Kobayashi-Newburger model of two overlapping immune waves. The infiltrating cells produce large quantities of matrix metalloproteinases (MMPs), particularly MMP-9, which degrades the extracellular matrix of the tunica media. Simultaneous production of IL-1β, IL-6, and TNF-α drives endothelial activation, thrombocyte aggregation, and further inflammatory recruitment.
The combination of medial destruction (from MMP-mediated matrix degradation) and outward force from intraluminal pressure causes the coronary artery wall to bulge — forming an aneurysm. Once formed, a giant aneurysm (Z-score ≥10 or diameter ≥8 mm) has a turbulent flow profile that promotes thrombosis within the aneurysm — the substrate for future myocardial infarction. IVIG works by suppressing this cytokine storm: its mechanism likely involves Fc-receptor blockade, regulatory T-cell induction, and suppression of pro-inflammatory cytokine production — but the exact mechanism is still debated.
SELF-CHECK
A 2-year-old girl has had fever for 7 days. She has bilateral conjunctival injection, strawberry tongue, and a maculopapular rash on her trunk. Her palms are red and swollen. Platelet count is 520 × 10³/µL (day 8 of illness). Echo shows the left anterior descending coronary artery Z-score of 2.8. Which statement about this child is correct?
A. She has incomplete Kawasaki disease because only 3 CREAM criteria are met
B. She has complete Kawasaki disease and her echo confirms coronary artery dilation
C. The elevated platelet count is the diagnostic criterion for Kawasaki disease
D. She should be treated with aspirin alone as the echo shows only mild dilation
Reveal Answer
Answer: B. She has complete Kawasaki disease and her echo confirms coronary artery dilation
This child has fever ≥5 days plus 4 CREAM criteria (conjunctivitis, rash, extremity changes/palm erythema/oedema, mucositis/strawberry tongue) — meeting criteria for complete Kawasaki disease. The echo showing LAD Z-score 2.8 (≥2.5) confirms coronary artery dilation, which is an additional marker of severity. Elevated platelets (thrombocytosis) in Kawasaki typically peaks in the second week and supports the diagnosis but is NOT a diagnostic criterion. Treatment is IVIG 2 g/kg (not aspirin alone) — she is still within the 10-day window if fever began on day 1 and this is day 8.
Diagnosis and Investigation
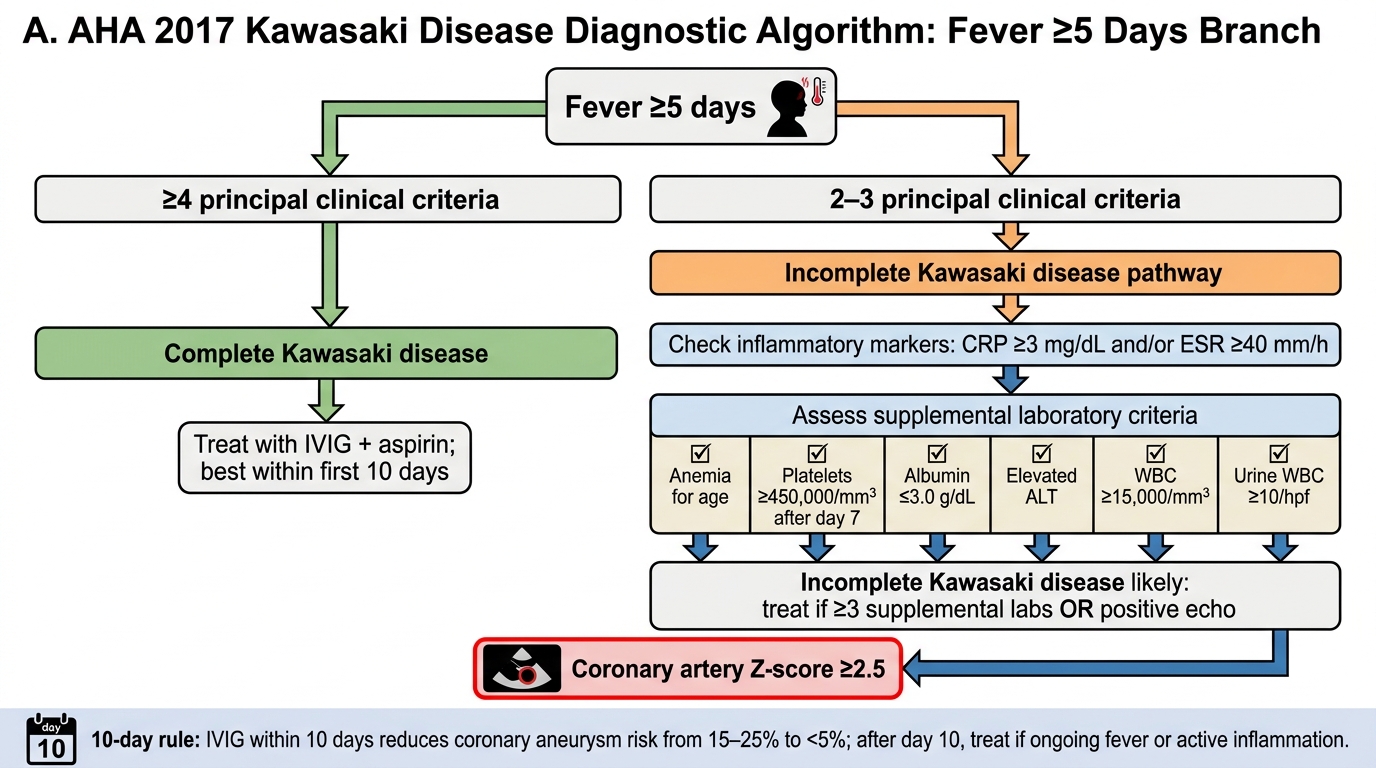
The diagnosis of Kawasaki disease is clinical, guided by the AHA/AAP 2017 algorithm, which provides a structured pathway for both complete and incomplete presentations. The algorithm is designed to prevent both under-diagnosis (missed incomplete cases with CAA risk) and over-diagnosis (unnecessary IVIG in other febrile illnesses).
Complete Kawasaki disease (straightforward): fever ≥5 days + ≥4 of 5 CREAM criteria. In a child with all 5 criteria, the diagnosis can be made on day 4 of fever if the clinical picture is unambiguous. A child with all 5 criteria and fever for <5 days can be diagnosed if the clinical picture is compelling — the 5-day rule exists to prevent treating ordinary viral fevers, not to create a mandatory waiting period when the diagnosis is certain.
Incomplete Kawasaki disease (AHA 2017 supplemental pathway): fever ≥5 days + only 2 or 3 CREAM criteria → perform CRP and ESR. If CRP ≥3 mg/dL OR ESR ≥40 mm/hr → check supplemental laboratory criteria. Treat if ≥3 of the following are present: albumin ≤3 g/dL, anaemia for age, ALT elevated above normal, platelets >450,000 after day 7, WBC ≥15,000/µL, urine ≥10 WBC/hpf (sterile pyuria). If <3 supplemental criteria → perform echocardiogram; if echo positive (Z ≥2.5 or pericardial effusion) → treat.
Echocardiography is the cornerstone investigation and should be performed in ALL suspected Kawasaki cases at diagnosis. The study images the left anterior descending (LAD), left main, and right coronary arteries. Results are reported as Z-scores (standard deviations from the mean adjusted for body surface area): Z <2.5 = normal; Z 2.5–5 = small dilation; Z 5–10 = medium aneurysm; Z ≥10 (or absolute diameter ≥8 mm) = giant aneurysm (highest thrombosis risk). Repeat echo at 2 weeks and 6 weeks after diagnosis.
Other investigations (supportive, not diagnostic):
• CBC: leucocytosis (WBC ≥15,000), normocytic anaemia, thrombocytosis (peaks week 2–3, often >600,000–1,000,000)
• CRP and ESR: markedly elevated (CRP >3 mg/dL, ESR >40 mm/hr)
• Albumin: low (marker of inflammation and capillary leak)
• Urinalysis: sterile pyuria (WBC in urine without bacteria) — from urethral inflammation, not infection
• LFTs: mild hepatitis, elevated GGT (occasional)
• Blood culture: to exclude bacterial causes of prolonged fever
IVIG resistance prediction — Kobayashi score: A scoring system using Na, bilirubin, AST, neutrophil %, platelets, CRP, and day of illness to predict children at high risk of IVIG non-response in Japanese populations; scores ≥4 predict resistance with ~75% sensitivity. Has been validated in some Indian centres but is not universally used outside Japan.
AHA 2017 Kawasaki Disease Diagnostic Algorithm
CLINICAL PEARL
The 10-day rule in Kawasaki disease is absolute: IVIG given within 10 days of fever onset reduces the risk of coronary artery aneurysm from 15–25% to less than 5%. IVIG given after day 10 may still reduce inflammation and is still recommended if the child has ongoing fever and/or signs of active disease, but the coronary protective effect is substantially diminished. When you see a febrile child on day 8 or 9 who fits incomplete Kawasaki, the calculus is simple — the risk of treating with IVIG unnecessarily (a mild aseptic meningitis rate of ~1–2%, haemolysis, volume overload) is vastly outweighed by the risk of missing the diagnosis and allowing coronary aneurysms to form. Treat early, investigate simultaneously.