Page 11 of 20
PE21.4 | Systemic Lupus Erythematosus — SDL Guide (Part 2)
Management of Paediatric SLE
The management of paediatric SLE requires a tiered approach based on the severity of organ involvement. The overarching goals are suppressing active disease, preventing flares, minimising treatment toxicity, and preserving long-term organ function — particularly renal. Unlike many chronic diseases in paediatrics, SLE management is lifelong, and the cumulative burden of glucocorticoid toxicity (growth failure, avascular necrosis, metabolic syndrome) is a major concern in adolescents.
Tier 1 — Anchor therapy for all patients:
Hydroxychloroquine (HCQ) 5 mg/kg/day (max 400 mg/day) is the cornerstone disease-modifying drug for ALL children with SLE without contraindication. It reduces flare frequency, reduces corticosteroid requirements, prevents end-organ damage, and reduces mortality — the only drug in SLE with evidence of survival benefit. Mechanism: inhibits TLR7/9 activation (prevents endosomal recognition of nuclear DNA/RNA), suppresses cytokine production, and has antiplatelet effects. Monitor for retinal toxicity (annual ophthalmological review after 5 years of use). Sun avoidance and sunscreen SPF ≥30 (photosensitivity is both a symptom and a trigger for flares — UV light drives DNA photo-oxidation and increases nuclear auto-antigen availability).
Tier 2 — Mild to moderate SLE (constitutional, skin, joint, mild serositis — no renal, no CNS, no severe haematological):
• NSAIDs: naproxen or ibuprofen for arthritis/arthralgia and pleuritis (weight-based dosing)
• Low-to-moderate dose prednisolone 0.5–1 mg/kg/day: for flares, tapered over 6–8 weeks
• Add hydroxychloroquine if not already started
• Methotrexate or azathioprine as steroid-sparing agents for frequent relapses
Tier 3 — Severe SLE (lupus nephritis Class III/IV, CNS lupus, severe haematological):
Lupus nephritis (Class III/IV) — induction (6 months):
• Prednisolone 1–2 mg/kg/day (pulses of methylprednisolone 30 mg/kg IV on days 1–3 for severe nephritis) PLUS
• Mycophenolate mofetil (MMF) 600 mg/m²/dose twice daily (preferred — equivalent efficacy to cyclophosphamide with less gonadal toxicity, hair loss, and infection risk — IAP and EULAR recommended) OR
• Cyclophosphamide IV (Euro-Lupus pulse: 500 mg IV every 2 weeks × 6 doses) for rapidly progressive nephritis or unresponsive to MMF
Maintenance (years): hydroxychloroquine + low-dose prednisolone + MMF (or azathioprine 2 mg/kg/day)
CNS lupus: high-dose methylprednisolone pulses + cyclophosphamide for severe manifestations (psychosis, seizures, transverse myelitis)
Haematological crises (severe thrombocytopenia, haemolytic anaemia): IVIG 1–2 g/kg + high-dose steroids; rituximab for refractory cases
Monitoring schedule (every 1–3 months in active disease): BP, urinalysis + protein:creatinine ratio, serum creatinine/eGFR, CBC + differential, ESR/CRP, anti-dsDNA, complement C3/C4, fasting lipids (glucocorticoid-related dyslipidaemia), HbA1c (glucocorticoid-related hyperglycaemia), DEXA scan annually (bone density — glucocorticoid-related osteoporosis → calcium + vitamin D supplementation)
Vaccination: inactivated vaccines on schedule (flu annual, pneumococcal); live vaccines (MMR, varicella) — only in remission on ≤10 mg/day prednisolone and not on high-dose immunosuppression; avoid live vaccines on cyclophosphamide
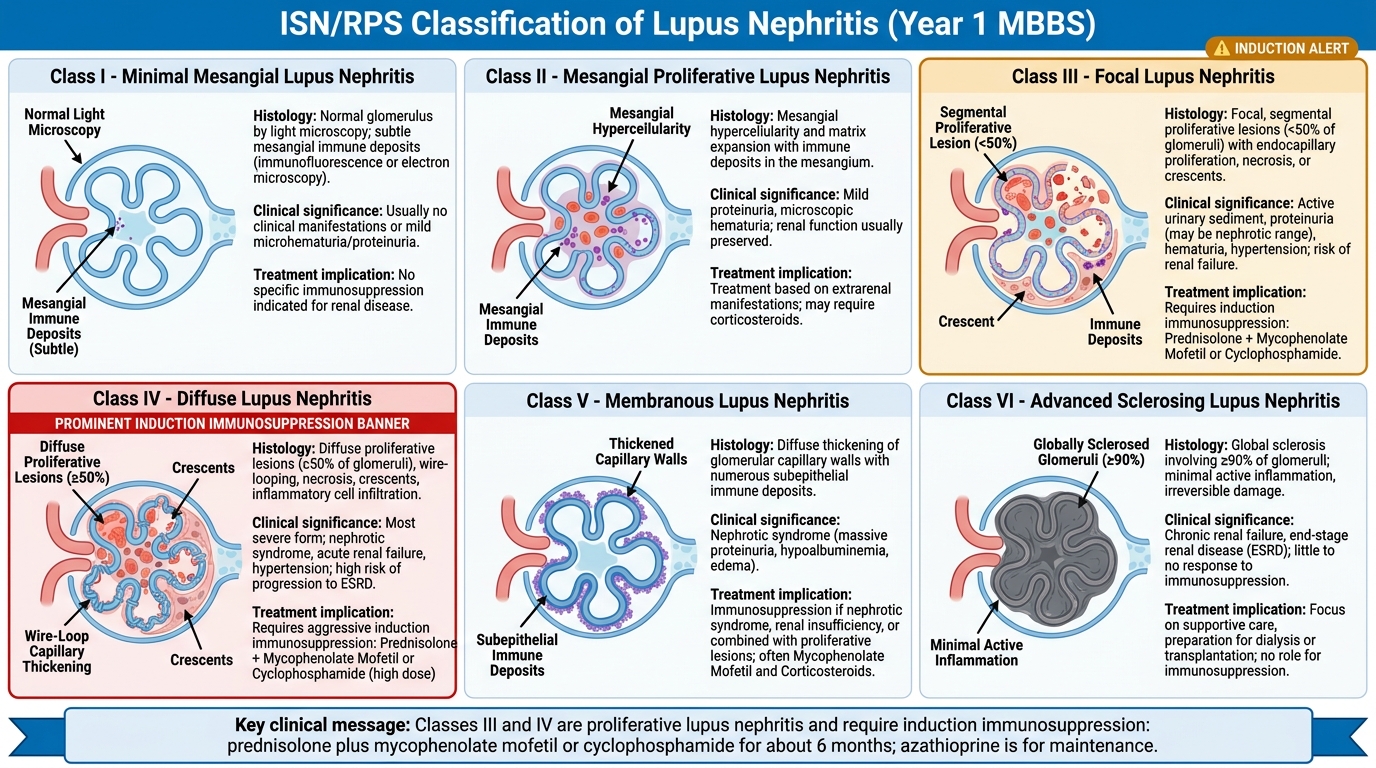
ISN/RPS Lupus Nephritis Classification
SELF-CHECK
A 13-year-old girl with SLE and biopsy-proven Class IV lupus nephritis (diffuse proliferative) is being started on induction therapy. Which of the following treatment combinations is evidence-based first-line induction for Class IV lupus nephritis in a paediatric patient?
A. Hydroxychloroquine alone — adequate for all classes of lupus nephritis
B. High-dose prednisolone alone for 6 months
C. Prednisolone + mycophenolate mofetil (or cyclophosphamide) for 6 months
D. Prednisolone + azathioprine — first-line for Class IV nephritis
Reveal Answer
Answer: C. Prednisolone + mycophenolate mofetil (or cyclophosphamide) for 6 months
Class IV lupus nephritis (diffuse proliferative — ≥50% of glomeruli affected) is the most severe and most common class in paediatric SLE. It requires aggressive induction therapy to prevent progression to end-stage renal disease. Evidence-based induction (EULAR, IAP, and ACR guidelines) is prednisolone PLUS either mycophenolate mofetil (MMF) or cyclophosphamide for 6 months. MMF is preferred in most paediatric centres because it achieves equivalent efficacy with less gonadal toxicity, less infection risk, and fewer adverse effects than cyclophosphamide. Azathioprine is used for maintenance (not induction). Hydroxychloroquine alone is not adequate for Class IV nephritis — it is the anchor for mild-moderate disease.
Self-Assessment
Apply your understanding of paediatric SLE to these clinical scenarios.
Case 1: A 16-year-old girl presents with a 4-month history of fatigue, joint pain (wrists, fingers), a facial rash, and hair loss. On examination: butterfly malar rash, mouth ulcers, mild synovitis of both wrists. CBC: Hb 9.8 g/dL (normocytic), WBC 2,800/µL, platelets 88,000/µL. Urinalysis: 3+ protein, 2+ blood. BP: 136/86 mmHg. How many SLICC criteria does she meet? Which investigations should you order next?
Expected answer: SLICC clinical criteria met: malar rash (1) + oral ulcers (1) + non-scarring alopecia (1) + arthritis (1) + leukopenia <4,000 (1) + thrombocytopenia <100,000 (1) + renal (proteinuria >500 mg/24h implied by 3+ on dipstick) (1) = 7 clinical criteria. Need at least 1 immunological criterion to classify. Order: ANA, anti-dsDNA, anti-Sm, antiphospholipid antibodies, complement C3/C4, direct Coombs test. If ANA positive (very likely given this picture), she meets SLICC criteria. Also: urine protein:creatinine ratio, serum creatinine — if nephritis confirmed, renal biopsy to determine ISN/RPS class.
Case 2: A 14-year-old with SLE on hydroxychloroquine and low-dose prednisolone has been in remission for 8 months. At today's visit: no symptoms, BP normal, urine dipstick negative, Hb 12.2 g/dL, WBC 5,200/µL, platelets 180,000/µL. But anti-dsDNA has risen from 45 to 210 IU/mL and C3 has fallen from 0.94 to 0.52 g/L. What is the significance of these results and what is your next step?
Expected answer: Rising anti-dsDNA + falling C3 indicates an impending flare (serologically active SLE), even though the patient is currently asymptomatic. This pattern predicts nephritis flare days to weeks before clinical manifestations. Next step: repeat urine protein:creatinine ratio and creatinine to check for early renal involvement; increase monitoring frequency to every 2–4 weeks; discuss with rheumatology about whether to increase hydroxychloroquine or add azathioprine/MMF before the flare becomes clinically overt. Do not wait for symptoms.
Case 3: A 12-year-old boy with SLE develops sudden-onset severe headache, confusion, and a generalised tonic-clonic seizure. He has been off prednisolone for 2 months (family stopped it themselves). His last CBC showed thrombocytopenia. ANA 1:640, anti-dsDNA markedly elevated, C3 undetectable. What is the diagnosis and immediate management?
Expected answer: Neuropsychiatric SLE (CNS lupus) — seizure as presentation, likely exacerbated by stopping immunosuppression. Must exclude other causes (intracranial infection, hypertensive encephalopathy, thrombotic microangiopathy in antiphospholipid syndrome). Immediate: secure airway, IV access, IV methylprednisolone 30 mg/kg (pulse), anti-epileptic as needed. Admit to HDU. Urgent MRI brain (NPSLE can show white-matter changes, cerebral vasculitis, posterior reversible encephalopathy). Restart and intensify immunosuppression under rheumatology/neurology guidance.