Page 12 of 31
PE22.4 | Acute Rheumatic Fever — SDL Guide (Part 2)
Management of Acute Rheumatic Fever
Management of acute rheumatic fever addresses three parallel goals: eradicating residual GAS from the throat (preventing antigen-driven continuation of the immune response), suppressing the acute inflammatory process in joints and heart, and managing any cardiac failure that has resulted from acute carditis. The sequence is to address all three simultaneously, then transition to the long-term secondary prophylaxis regimen that is the most important intervention in ARF management. Bed rest during the acute phase reduces cardiac work and facilitates monitoring of the evolving clinical picture, particularly the trajectory of carditis. A structured approach ensures that no element of management is overlooked and that the transition from acute inpatient management to the long-term outpatient prophylaxis programme is explicitly planned before discharge.
A. Eradication of Group A Streptococcus:
- Benzathine penicillin G (IM, single dose) — drug of choice for eradication:
- <27 kg: 600,000 IU IM once
- ≥27 kg: 1,200,000 IU IM once
- Alternatively: oral phenoxymethylpenicillin (penicillin V) 12.5 mg/kg twice daily for 10 days, or oral amoxicillin 50 mg/kg once daily for 10 days.
- Penicillin allergy: erythromycin or azithromycin.
- Note: this eradication dose is NOT the same as the long-term prophylaxis regimen. Eradication occurs first; prophylaxis then continues long-term.
B. Anti-inflammatory therapy:
- Aspirin is the primary anti-inflammatory agent for ARF — the joint response to aspirin is so dramatic (pain relief within 24–48 hours) that it has diagnostic value. Dose: 60–100 mg/kg/day in 4 divided doses (max 4 g/day) for 4–6 weeks, then taper.
- Monitor for salicylate toxicity: tinnitus, hyperventilation, vomiting.
- Reye's syndrome risk — use the lowest effective dose and avoid in children with concurrent viral illness.
- Corticosteroids (prednisolone 2 mg/kg/day) — reserved for severe carditis with cardiac failure, pericarditis, or in children who cannot tolerate aspirin. Reduces inflammation faster than aspirin but does not prevent RHD progression.
- No aspirin for Sydenham chorea (aspirin has no role in chorea management). Chorea is managed with rest and pharmacological sedation if severe: haloperidol (0.01–0.03 mg/kg/day) or carbamazepine (5–10 mg/kg/day) for disabling chorea; valproate as an alternative.
C. Management of cardiac failure from acute carditis:
• Treat as cardiac failure (see PE22.3): bed rest, diuretics (furosemide), ACE inhibitors, digoxin.
• Restrict physical activity during active carditis — strenuous exercise is contraindicated.
• Echocardiographic monitoring of valve function.
D. Bed rest:
• Strict bed rest during acute phase (especially with active carditis): until inflammatory markers normalise and heart rate settles.
• Gradual ambulation guided by ESR, CRP, and cardiac status.
Secondary Prophylaxis and Rheumatic Heart Disease Prevention
Secondary prophylaxis — the regular long-term administration of penicillin to prevent recurrent GAS pharyngitis and thereby prevent recurrent episodes of ARF — is the most important intervention in the entire management of ARF. Every recurrence of ARF in a child with established rheumatic carditis adds further valve damage; each recurrence-free year is a year the mitral valve is protected. The duration of prophylaxis is determined by the severity of cardiac involvement at the index episode and at each subsequent review, because severity may evolve over time. In India, where follow-up is inconsistent and access to echocardiography variable, the default should be a longer duration of prophylaxis rather than a shorter one — the risk of undertreating is valve replacement surgery at age 25.
Provided image
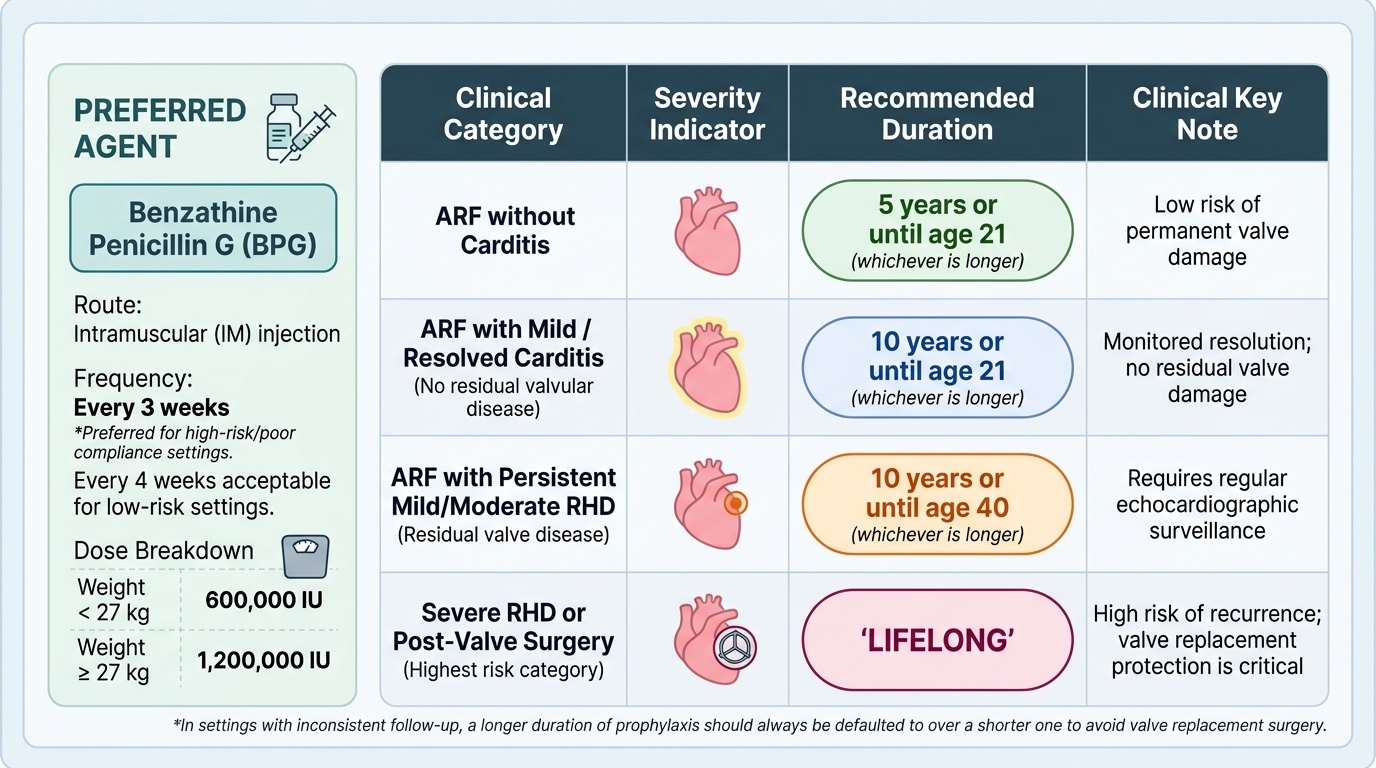
Benzathine penicillin G (BPG) — the drug of choice for secondary prophylaxis:
• Dose: 600,000 IU IM for <27 kg; 1,200,000 IU IM for ≥27 kg
• Frequency: every 3 weeks (preferred for high-risk populations including India where compliance monitoring is difficult); every 4 weeks acceptable in lower-risk settings
• Why IM not oral? Oral penicillin V requires daily compliance over years — adherence is poor. A 3-weekly injection, given in a clinic or at home by a trained person, is far more reliable.
Duration of prophylaxis (IAP/AHA guidelines — by severity of cardiac involvement):
| Category | Duration |
|---|---|
| ARF without carditis | 5 years or until age 21 (whichever is longer) |
| ARF with mild / resolved carditis (no residual valve disease) | 10 years or until age 21 (whichever is longer) |
| ARF with persistent mild/moderate RHD | 10 years or until age 40 (whichever is longer) |
| Severe RHD or post-valve surgery | Lifelong |
Primary prevention (preventing ARF):
Treat every GAS pharyngitis with a complete course of penicillin (benzathine IM once, or oral 10 days). In India, this requires rapid diagnostic capacity (rapid strep test or throat culture) and access to penicillin at the primary care level — the public health challenge.
Rheumatic heart disease register (RHD register):
Children diagnosed with ARF should be enrolled in a structured follow-up programme with regular echocardiographic surveillance and documentation of each prophylaxis injection. This is the programmatic implementation of secondary prophylaxis and is supported by IAP and WHO.
SELF-CHECK
A 12-year-old girl is diagnosed with ARF and is found on echocardiography to have moderate mitral regurgitation due to rheumatic carditis. She weighs 35 kg. Which secondary prophylaxis regimen is most appropriate?
A. Oral penicillin V 250 mg bd for 10 years or until age 21
B. Benzathine penicillin G 600,000 IU IM every 3 weeks for 5 years
C. Benzathine penicillin G 1,200,000 IU IM every 3 weeks for at least 10 years or until age 40
D. No prophylaxis needed as moderate regurgitation often resolves spontaneously
Reveal Answer
Answer: C. Benzathine penicillin G 1,200,000 IU IM every 3 weeks for at least 10 years or until age 40
She weighs 35 kg (≥27 kg), so the prophylaxis dose is 1,200,000 IU IM. She has moderate mitral regurgitation (persistent moderate RHD), placing her in the category requiring at least 10 years of prophylaxis or until age 40 (whichever is longer) — not just 5 years (which applies to ARF without carditis). Oral penicillin has poor adherence over years and is not preferred for high-risk children. No prophylaxis is never correct for any child with ARF, particularly with documented carditis.
Self-Assessment
This self-assessment section targets the high-yield clinical and prescribing knowledge from the ARF module. The Jones Criteria, the prophylaxis duration table, and the Sydenham chorea management are the three areas most commonly tested in final MBBS examinations and most consequential in clinical practice. A child who develops ARF and is not placed on adequate secondary prophylaxis will return 5–10 years later with mitral stenosis — a preventable outcome that is directly attributable to inadequate management at the initial presentation. Work through each question carefully, and pay particular attention to which features are major versus minor criteria — this distinction is frequently misclassified by students, often with clinical consequences when a borderline case is either over- or under-diagnosed.
Key self-test questions:
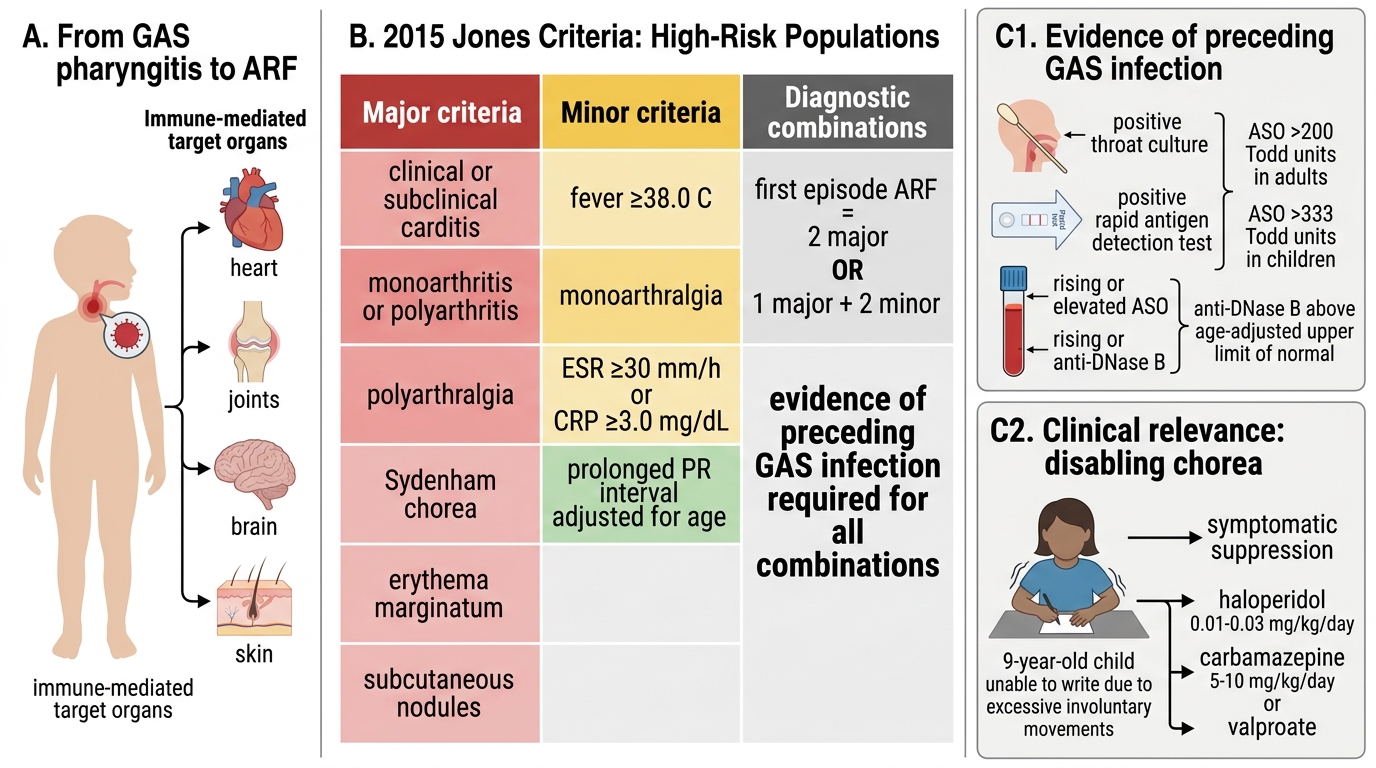
- List the five major and four minor Jones 2015 criteria for high-risk populations.
- Name two differences between the high-risk and low-risk Jones 2015 criteria.
- A 10-year-old weighing 28 kg has ARF. What dose of benzathine penicillin G do you give for (a) GAS eradication and (b) secondary prophylaxis? How often is prophylaxis given?
- A child with ARF has Sydenham chorea. Is aspirin indicated? What do you use instead?
- What duration of secondary prophylaxis would you recommend for: (a) ARF without carditis, (b) ARF with persistent moderate RHD?
- Why is IM benzathine penicillin preferred over oral penicillin V for secondary prophylaxis?
- Subcutaneous nodules in ARF are associated with which severity of cardiac involvement?
- Name the pathognomonic histological lesion of rheumatic carditis.
Key thresholds to memorise:
• BPG dose: 600,000 IU (<27 kg) | 1,200,000 IU (≥27 kg)
• BPG frequency: every 3 weeks (high-risk/India) or every 4 weeks
• Aspirin dose: 60–100 mg/kg/day in 4 divided doses
• ASO titre significant: >200 Todd units in children
2015 Jones Criteria for High-Risk Populations
SELF-CHECK
Sydenham chorea in a 9-year-old girl with ARF is severely disabling — she cannot feed herself or write. Which treatment is most appropriate for the chorea itself?
A. High-dose aspirin 100 mg/kg/day for 6 weeks
B. Oral corticosteroids (prednisolone 2 mg/kg/day)
C. Haloperidol or carbamazepine for symptomatic suppression of chorea
D. No treatment needed as Sydenham chorea resolves spontaneously within days
Reveal Answer
Answer: C. Haloperidol or carbamazepine for symptomatic suppression of chorea
Sydenham chorea is managed symptomatically. Aspirin has no role in chorea management (it is the anti-inflammatory agent for carditis and arthritis). Steroids are used for severe carditis, not chorea. When chorea is disabling (cannot feed, write, or ambulate safely), pharmacological suppression with haloperidol (0.01–0.03 mg/kg/day), carbamazepine (5–10 mg/kg/day), or valproate is indicated. Chorea does resolve spontaneously over weeks to months, but waiting without treatment when it is disabling is not appropriate clinical management.