Page 6 of 31
PE22.2 | Cyanotic Heart Disease — SDL Guide (Part 3)
Self-Assessment
Having worked through the clinical presentation, pathophysiology, five major lesions, investigation approach, and management of cyanotic congenital heart disease, this self-assessment section consolidates the high-yield factual knowledge that examiners target. The questions below span the full arc of the module — from the clinical patterns that should trigger recognition, through the haemodynamic reasoning that explains each lesion's behaviour, to the specific thresholds and procedural details that distinguish safe from unsafe practice. Work through each question before checking your answer. Pay particular attention to the numerical thresholds (PGE1 dose, morphine dose, repair timing) and the discriminating ECG feature of tricuspid atresia, as these are the most frequently tested and most consequential items. If you are uncertain on any question, return to the relevant section before your next clinical encounter.
Key questions for self-testing:
- Name the four anatomical components of Tetralogy of Fallot.
- What is the PGE1 (alprostadil) dose for a duct-dependent cyanotic lesion in a neonate?
- What is the initial management sequence for a tet-spell?
- Which is the only cyanotic CHD characterised by left axis deviation on ECG?
- What CXR finding is characteristic of TGA?
- In which cyanotic lesion is the Rashkind balloon atrial septostomy the first-line palliation?
- What is the 'hyperoxia test' and how do you interpret a PaO₂ of 90 mmHg on 100% O₂?
- Name two important long-term complications of chronic cyanosis and explain their mechanism.
Key numbers and thresholds:
• PGE1 dose: 0.05–0.1 mcg/kg/min IV
• Morphine for tet-spell: 0.1 mg/kg IV or SC
• Propranolol for tet-spell prevention: 1–2 mg/kg/day oral in 3 divided doses
• Arterial switch operation: within first 2 weeks of life for TGA
• TOF total repair: typically 3–6 months of age
• Cyanosis clinically apparent at reduced Hb ≥3–5 g/dL
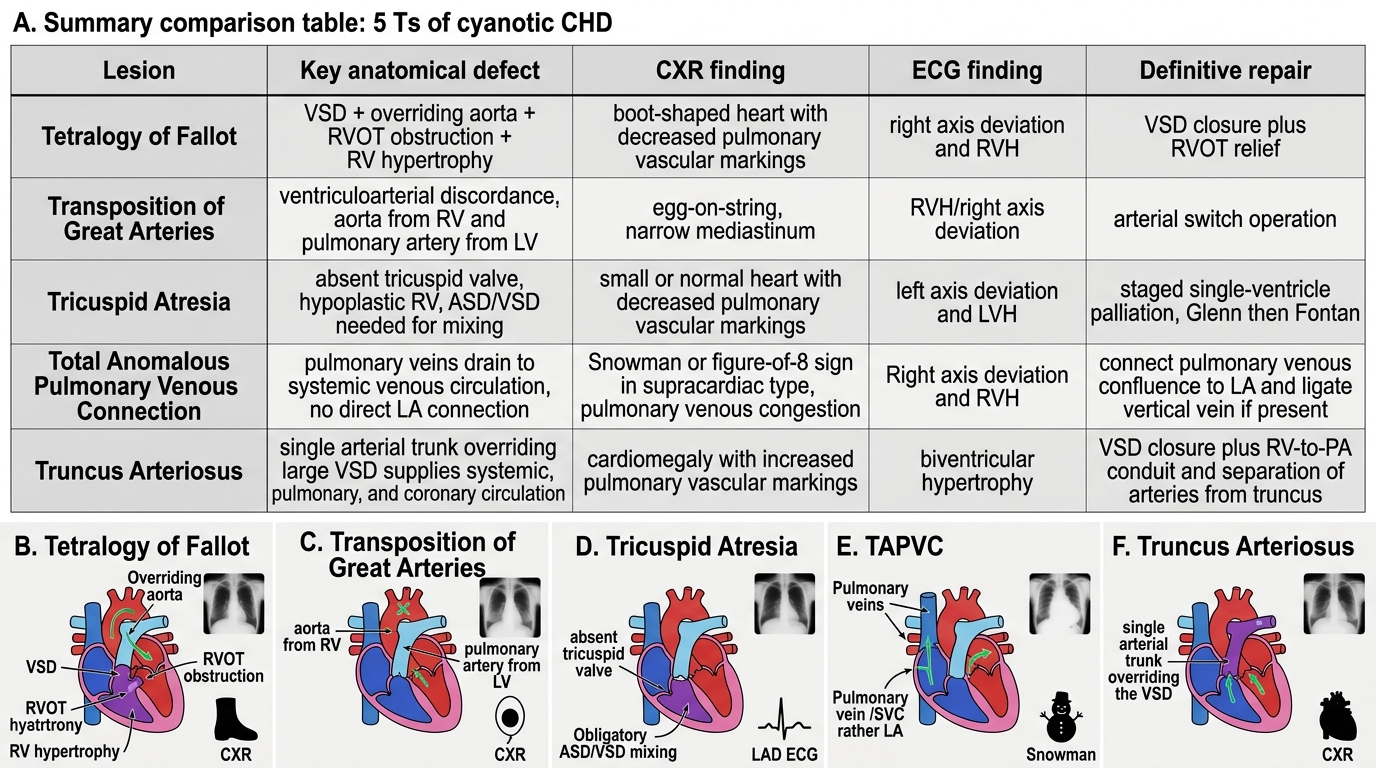
The 5 Ts of Cyanotic Congenital Heart Disease
SELF-CHECK
A 3-year-old child with unrepaired TOF presents with fever and right-sided hemiparesis. CT brain shows a ring-enhancing lesion. What is the most likely complication and its mechanism?
A. Cerebral venous thrombosis from polycythaemia
B. Brain abscess from paradoxical septic embolism bypassing pulmonary capillary filtration
C. Viral encephalitis from immunosuppression
D. Watershed infarction from low cardiac output
Reveal Answer
Answer: B. Brain abscess from paradoxical septic embolism bypassing pulmonary capillary filtration
Brain abscess is the classic CNS complication of cyanotic CHD in children >2 years. The right-to-left shunt allows septic emboli (bacteria in venous blood) to bypass pulmonary capillary filtration and directly seed the cerebral circulation. The ring-enhancing lesion on CT is characteristic of an abscess. Polycythaemia increases thrombosis risk but produces bland, not ring-enhancing lesions. Viral encephalitis and watershed infarction do not produce ring-enhancing lesions.