Page 15 of 31
PE22.5 | Infective Endocarditis — SDL Guide (Part 2)
Management of Infective Endocarditis
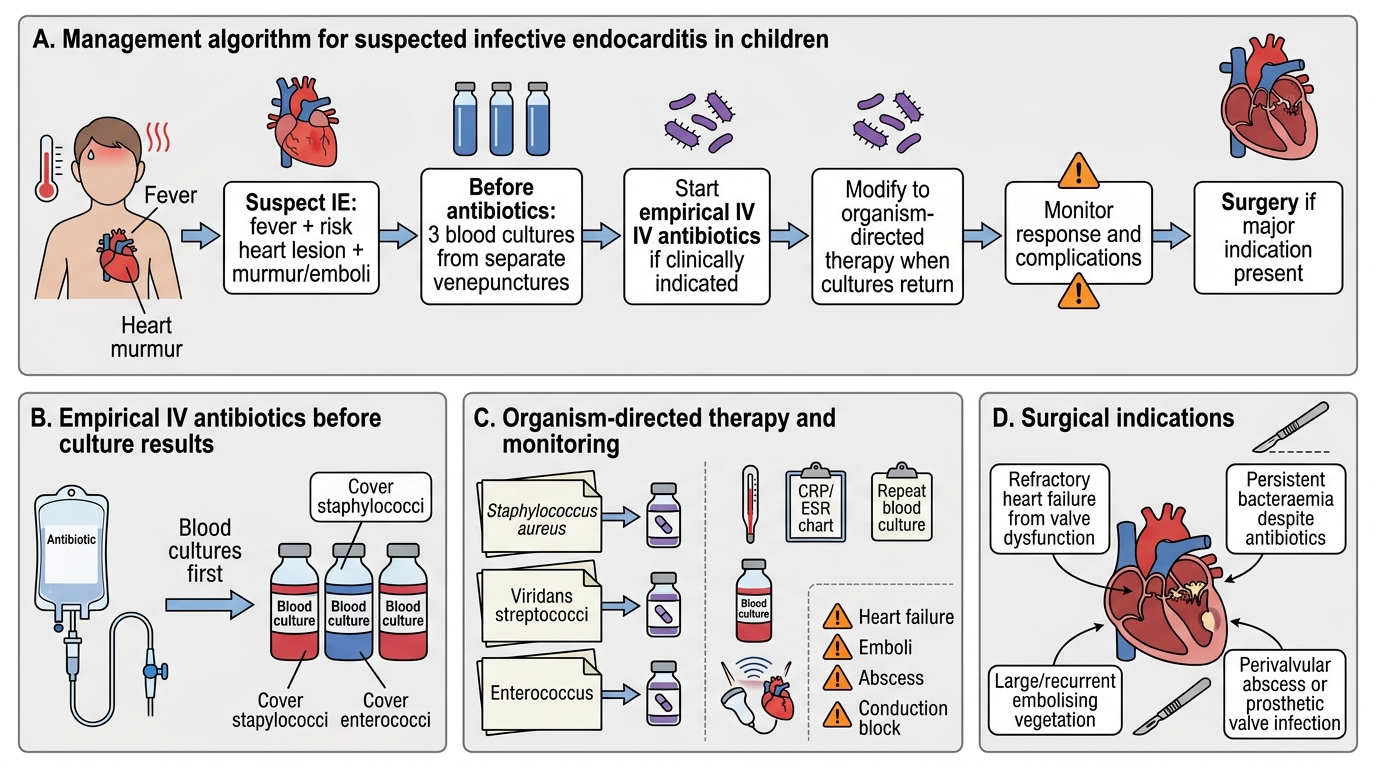
Management of infective endocarditis requires prolonged parenteral antibiotic therapy — the avascular interior of vegetations means that bacteria are shielded from antibiotic penetration, and oral bioavailability is insufficient to achieve the bactericidal concentrations required within the vegetation. Empirical antibiotic therapy is started after blood cultures are taken, then de-escalated or targeted once culture and sensitivity results return. The minimum duration of IV therapy is 4 weeks for viridans streptococcal IE on native valves; 6 weeks for Staph aureus, prosthetic valves, and any complicated IE. Monitoring for complications — particularly valve destruction leading to cardiac failure and embolic events — is continuous throughout the course of treatment, and surgical intervention is required in a substantial minority.
A. Empirical antibiotic therapy (before culture results — if clinically urgent):
- For native valve IE (most children):
- IV benzylpenicillin (or ampicillin) + IV gentamicin — covers streptococci and HACEK organisms
- If Staph aureus IE is likely (central line, acute onset, community-acquired): IV flucloxacillin + IV gentamicin
- If MRSA suspected or penicillin-allergic: IV vancomycin + IV gentamicin
- For prosthetic valve or post-cardiac surgery IE:
- IV vancomycin + IV gentamicin + oral rifampicin (covers MRSA and coagulase-negative staphylococci)
B. Targeted antibiotic therapy (after culture and sensitivity):
- Streptococcus viridans (penicillin-sensitive): IV penicillin G × 4 weeks (+ gentamicin for first 2 weeks for synergy in selected cases)
- Staphylococcus aureus (MSSA): IV flucloxacillin × 4–6 weeks
- Staphylococcus aureus (MRSA): IV vancomycin × 6 weeks
- Culture-negative IE: IV gentamicin + IV doxycycline (for Coxiella/Bartonella)
C. Monitoring during treatment:
• Blood cultures every 48–72 h until negative (confirms bacteraemia clearance)
• Serial echocardiography to monitor vegetation size and valve function
• Daily examination for new embolic events, development of cardiac failure, or signs of drug toxicity (vancomycin nephrotoxicity; gentamicin nephrotoxicity and ototoxicity — check trough levels)
D. Surgical indications (emergency or urgent surgery):
• Haemodynamic instability from severe valvular regurgitation or obstruction (cardiac failure not responding to medical management)
• Uncontrolled sepsis or failure to clear bacteraemia after 7–10 days of appropriate antibiotics
• Large mobile vegetation (>10 mm) with high embolic risk, particularly on left-sided valves
• Perivalvular extension (annular abscess, fistula)
• Fungal IE or organisms with poor antibiotic response
E. Antibiotic prophylaxis for high-risk CHD (prevention of IE):
Per AHA/IAP guidelines, prophylaxis is recommended ONLY for the highest-risk CHD categories:
• Unrepaired cyanotic CHD (including palliative shunts and conduits)
• Previous IE
• CHD with prosthetic cardiac valve or material
• CHD repaired within the last 6 months (until endothelialisation)
• Repaired CHD with residual defects at or adjacent to a prosthetic patch/device
Prophylaxis regimen: Amoxicillin 50 mg/kg oral (max 2 g), 30–60 minutes before dental procedure. Penicillin allergy: clindamycin 20 mg/kg (max 600 mg).
NOT recommended for routine CHD without the above risk factors, mitral valve prolapse without regurgitation, or ASD.
Management Algorithm for Pediatric Infective Endocarditis
SELF-CHECK
A 9-year-old with a repaired TOF (residual tiny VSD patch) is scheduled for dental extraction. The dentist asks if antibiotic prophylaxis is needed. According to AHA/IAP guidelines, what is the correct advice?
A. No prophylaxis needed as the TOF was surgically repaired
B. Prophylaxis recommended: amoxicillin 50 mg/kg oral (max 2g) 30–60 minutes before extraction
C. Prophylaxis only needed if the patient has a fever
D. Prophylaxis only needed if the patient has had a previous episode of IE
Reveal Answer
Answer: B. Prophylaxis recommended: amoxicillin 50 mg/kg oral (max 2g) 30–60 minutes before extraction
Repaired CHD with a residual defect at or adjacent to a prosthetic patch/device is one of the five highest-risk categories where prophylaxis is recommended per AHA/IAP guidelines. A residual tiny VSD patch qualifies. The correct regimen is amoxicillin 50 mg/kg oral (max 2g) 30–60 minutes before the dental procedure. Prophylaxis is NOT recommended for ALL repaired CHD — only for those with residual defects at/adjacent to prosthetic material (within 6 months of repair, full endothelialisation has not occurred), or those with previous IE, or unrepaired cyanotic CHD.
Self-Assessment
This self-assessment section consolidates the diagnostic, prescribing, and prophylaxis knowledge from the infective endocarditis module. The modified Duke Criteria, the blood culture protocol, the organism-context pairing, and the prophylaxis indications are the four domains most frequently tested in final MBBS examinations and most directly applicable to clinical practice. A systematic approach to these questions — working from the clinical picture to the Duke Criteria category to the blood culture plan to the antibiotic choice — is the same cognitive sequence you will use at the bedside. Note particularly the distinction between which CHD patients require prophylaxis and which do not, as this is one of the most commonly misapplied guidelines in paediatric cardiology, and getting it right directly affects whether a child like the one in the opening scenario ever needs to be hospitalised.
Key self-test questions:
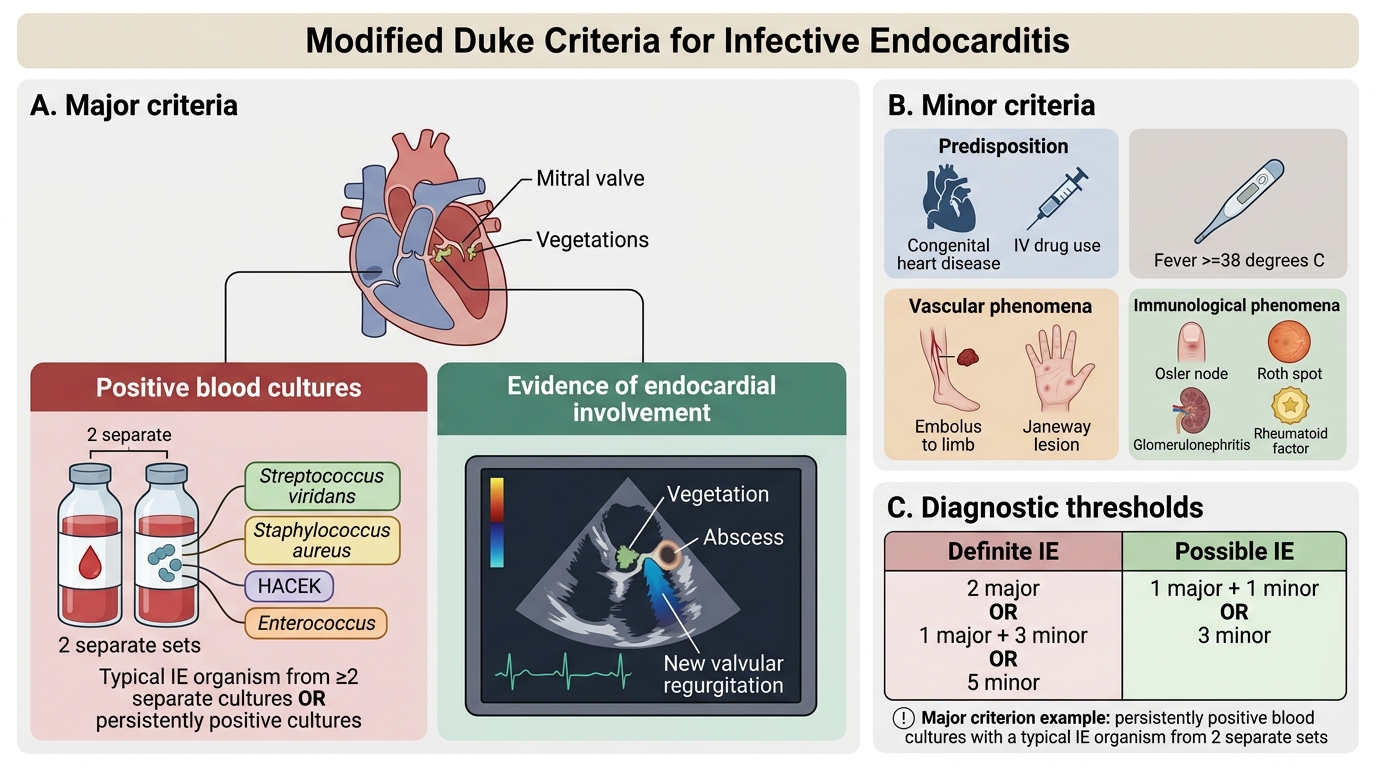
- List the two major Duke Criteria and five minor Duke Criteria for IE.
- How many blood culture sets are required? From which sites? When should they be drawn relative to antibiotics?
- Name the most common organism causing IE in a child with unrepaired VSD following a dental procedure.
- A child with Staph aureus IE develops a vegetation on the mitral valve with severe mitral regurgitation and worsening cardiac failure despite IV antibiotics for 5 days. What is the next management step?
- Which five categories of CHD require antibiotic prophylaxis before dental procedures per AHA/IAP guidelines?
- What is the prophylaxis antibiotic, dose, and timing?
- What are Osler nodes and Janeway lesions — how do they differ and what is the mechanism of each?
- What is the minimum duration of IV antibiotic therapy for native valve streptococcal IE?
Key numbers:
• Blood cultures: 3 sets from 3 separate venepunctures before antibiotics
• Amoxicillin prophylaxis: 50 mg/kg (max 2 g) oral 30–60 min before dental procedure
• Minimum IV therapy: 4 weeks (viridans streptococci); 6 weeks (Staph aureus, prosthetic valve)
Modified Duke Criteria for Infective Endocarditis
SELF-CHECK
Which of the following is a MAJOR Duke criterion for infective endocarditis?
A. Fever ≥38°C
B. Predisposing heart condition (CHD)
C. Persistently positive blood cultures with a typical IE organism from 2 separate sets
D. Osler nodes on the finger pads
Reveal Answer
Answer: C. Persistently positive blood cultures with a typical IE organism from 2 separate sets
Persistently positive blood cultures with a typical IE organism (Streptococcus viridans, Staph aureus, HACEK, etc.) from 2 separate blood culture sets is a MAJOR Duke criterion. Fever ≥38°C, predisposing heart condition, and Osler nodes (an immunological phenomenon) are all MINOR criteria. The two major criteria are: (1) positive blood culture (typical organism from ≥2 separate cultures or persistently positive); and (2) evidence of endocardial involvement (positive echo showing vegetation/abscess/new valvular regurgitation).